")
Back to Journals » Journal of Inflammation Research » Volume 17
Successful Treatment of Pediatric Generalized Pustular Psoriasis (GPP) with Spesolimab: 5 Case Reports and Evaluations of Circulating IL-36 Levels
Authors Chen Y , Wang Z, Liang Y, Shen C, Jiao L, Xiang X, Miao C, Xu Z
Received 21 August 2024
Accepted for publication 24 October 2024
Published 4 November 2024 Volume 2024:17 Pages 8199—8206
DOI https://doi.org/10.2147/JIR.S485077
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yunliu Chen,1,2,* Zhaoyang Wang,1,2,* Yuan Liang,1,2 Chunping Shen,1,2 Lei Jiao,1,2 Xin Xiang,1,2 Chaoyang Miao,1,2 Zigang Xu1,2
1Department of Dermatology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijng, People’s Republic of China; 2Key Laboratory of Major Diseases in Children, Ministry of Education, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zigang Xu, Email [email protected]
Background: Generalized pustular psoriasis (GPP) is a rare, severe, and potentially life-threatening inflammatory cutaneous disease. IL-36 is a key treatment target in GPP. Spesolimab, a humanized monoclonal antibody of the IL-36 receptor, has demonstrated a good efficacy and a favorable safety profile in adults with GPP. However, data on its use in children are scarce.
Methods: We treated patients aged 4– 12 years with GPP with a single dose of spesolimab. The Generalized Pustular Psoriasis Physician Global Assessment (GPPGA) total score, GPPGA pustulation sub-score, Generalized Pustular Psoriasis Area and Severity Index (GPPASI), and the Japanese Dermatological Association severity index for GPP were evaluated. The levels of IL-36α, IL-36β, and IL-36γ were detected by the magnetic bead-based immunoassays, and the levels of IL-17A, IL-17C, IFN-γ, TNF, IL-6, and IL-8 were measured by the Olink proximity extension assay technology.
Results: We included five patients (four boys and one girl) with a median age was 6.9 years old (range: 4.8 to 10.6 years), and a median age of onset of 1.7 years (range: 3 months– 10 years and 5 months). After 1 week of spesolimab administration, all patients had a total GPPGA score of 0/1 and pustulation subscore of 0, all patients had a GPPASI of 50, and four patients had a GPPASI of 75. Meanwhile, plasma levels of IL-36α, IL-36β, IL-36γ, IL-17A, IL-17C, IFN-γ, TNF, IL-6, IL-8 all decreased, and those of IL-36α, IL-36β, IL-17A, IL-17C, and IL-6 were statistically significant. There was no recurrence after 2 to 8 months of treatment. No other adverse event was recorded apart from one patient who experienced an upper respiratory infection in the first week.
Conclusion: Spesolimab might be a prospective option for children aged 4 to 12 years.
Keywords: generalized pustular psoriasis, pediatrics, spesolimab, IL-36R
Introduction
Generalized pustular psoriasis (GPP) is a rare chronic, relapsing, and severe inflammatory cutaneous disease characterized by generalized pustular edematous erythema, and usually associated with fever, headaches, asthenia, myalgia, and raised C-reactive protein (CRP) level and white blood cell count (WBC).1 Most GPP patients who present with an earlier onset of disease and no history of psoriasis vulgaris have a homozygous or compound heterozygous mutation of the IL36RN gene.2,3 Moreover, patients with alternative genetic mutation of IL-36 associated inflammatory cascade, such as CARD14, AP1S3, and MPO, could have similar phenotypes.4
The IL-36 pathway plays a central role in the pathogenesis of GPP.5 IL-36 is a pro-inflammatory cytokine, with subunits IL-36α, IL-36β, and IL-36γ, belonging to the IL-1 cytokines family. Upon binding to its receptor, IL-36 activates nuclear factor-κB (NF-κB) and mitogen-activated protein kinase (MAPK) signal pathways resulting in the secretion of extensive pro-inflammatory cytokines and chemokines, such as IL-36 precursors, IL-1β, TNF-α, IL-6, IL-23, CXCL8, CXCL1, and CXCL2.6 Those chemokines and cytokines recruit and activate immune cells, hence forming an inflammatory loop.6 Dysfunction in the IL-36 receptor (IL-36R) results in an overactivity of the inflammatory cascade.
GPP always requires systemic drugs, as topical drugs alone are insufficient.7 Biologic agents targeting TNF-α, IL-23, IL-17, and IL-36, or their receptors might be good candidates.8 Considering the key role of IL-36 in GPP,5 inhibitors of IL-36 or IL-36R could be effective. Spesolimab is a humanized monoclonal antibody of the IL-36R, which could inhibit the over-activation of the IL-36/IL-36R signal. Moreover, spesolimab has been approved by the US Food and Drug Administration, European Medicines Agency, and China Food and Drug Administration to treat GPP in adults. In china, all treatments for GPP are off-label except spesolimab, which was approved in 2022. However, data on its use in children under 12 years with GPP is scarce. We present five children with GPP treated with a single dose of spesolimab and followed up for its efficacy on disease symptoms and its impact on circulating IL36 levels.
Methods
Participants
Five patients aged 4–12 with GPP were enrolled at the Beijing Children’s Hospital from November 2023 to March 2024. We included patients who met the GPP criteria of the Japanese Dermatological Association (JDA);7 with a Generalized Pustular Psoriasis Physician Global Assessment (GPPGA) score ≥3, GPPGA pustulation subscore ≥2, body surface area (BSA) ≥10%, and Generalized Pustular Psoriasis Area and Severity Index (GPPASI) score ≥10; and with progressing disease severity. The five patients included did not achieve long-term remission on previous treatment, including adalimumab, secukinumab, acitretin and topical drugs.
Intervention
A single intravenous dose of spesolimab was given on day 0. This dose depended on the patient’s body weight (450mg for 20–50kg and 900mg for ≥50kg). Although spesolimab is off-label in children with GPP, previous data showed its efficacy and safety. Before starting spesolimab, we excluded current or latent infections of viral B and C hepatitis, tuberculosis, and HIV.
Outcome Measure
GPP severity was assessed by BSA, GPPGA total score, GPPGA pustulation sub-score, GPPASI, and JDA severity index for GPP.7 Drug-related adverse events were assessed from day 0. Cytokines and chemokines were measured in EDTA plasma before treatment and 1 week after spesolimab administration. The concentrations of IL-36α, IL-36β, and IL-36γ were assessed by magnetic bead-based immunoassays (magEasyQPlex). The levels of IL-17A, IL-17C, IFN-γ, TNF, IL-6, and IL-8 in the plasma were quantified by the Olink inflammation panel based on the proximity extension assay technology in the plasma, and the amount of protein was evaluated by Normalized Protein Expression (NPX).
Statistical Analysis
Data analysis was performed via the statistical SPSS26.0 software. Median and range were used for descriptive statistics. A paired-samples t-test was carried out for normally distributed data. Otherwise, the Wilcoxon-signed ranks test was used. A P <0.05 was considered statistically significant.
Result
We included four boys and one girl with GPP (Table 1). The median age was 6.9 years (range: 4.8−10.6 years), and the median age of onset was 1.7 years old (range: 3 months−10 years and 5 months). The median disease course was 48 months (range: 2−64 months). No participant had psoriasis vulgaris in the course of the disease. One patient had a family history of psoriasis, whose grandfather suffered from psoriasis plaque. Three patients presented with a map tongue. One patient was obese, and the BMI of other patients was within normal range.
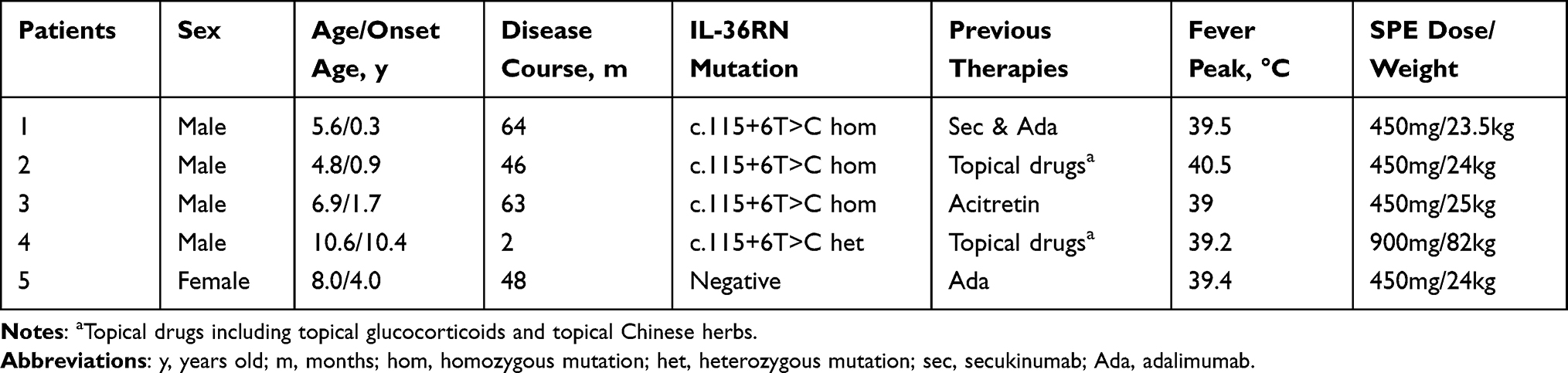 |
Table 1 Clinical Characteristics and Spesolimab Treatment Protocols in Five Juveniles with GPP |
Four patients had the IL-36RN c.115+6T>C variants, including three homozygous mutations and one heterozygous. No patient carried the CARD14, AP1S3, or MPO variant. Three patients had received systemic treatment for previous eruptions (adamulimab and secukinumab in patient 1, acitretin in patient 3, and adamulimab in patient 5).
Before treatment, all patients presented with high fever and an increased number of pustules. At baseline, the median BSA was 65% (range: 61–97%), median GPPASI was 38.5 (range: 29.6–63.5), and median JDA scores were 13 points (range: 10–17 points). The GPPGA total score was 3 (moderate) in four patients, and 4 (severe) in one patient. The GPPGA pustulation subscore was 3 in three patients, and 4 in two patient.
No new skin lesion developed at the median of 3 days (range: 1–5) after treatment. Overall, the body temperature decreased to ≤38°C after a median of 2 days (range: 0–4) and returned to normal after a median of 4 days (range: 0–6). Moreover, one patient had no fever within 2 hours. At the end of 1 week with spesolimab-treatment, BSA, GPPGA, GPPGA pustulation subscores, and JDA scores decreased significantly (P = 0.008, P = 0.003, P = 0.034, P = 0.038, and P = 0.001 respectively), and all patients had a GPPGA total score of 0/1, with a median of 3 days (range: 2–6), all patients had a GPPGA pustulation subscore of 0, with a median of 4 days (range: 1–6), all patients had a GPPASI of 50, with a median of 3 days (range: 2–4), and four patients had a GPPASI of 75. The median time achieving GPPASI of 75 in five patients was 6 days (range: 5–8). After spesolimab treatment, the median JDA scores decreased to 7 points (range: 5–9) on day 3, and 3 points (range: 2–4) on day 7 (Figure 1).
 |
Figure 1 Cutaneous presentation before treatment (a) and after one-week treatment with spesolimab (b); (c and d) showed GPPASI scores and JDA scores at baseline and after treatment with spesolimab; e-g showed number of patients whose body temperature decreased to ≤ 38°C or ≤ 37.2°C (e), GPPGA0/1 or GPPGA pustulation subscore of 0 (g), and number of patients achieved GPPASI of 50 or GPPASI of 75 (f) after treatment with spesolimab. |
The WBC and CRP levels significantly decreased (P = 0.029, and P = 0.001) and the albumin level significantly increased (P = 0.018) 7 days after spesolimab administration.
The median level of IL-36α was 63.44 pg/mL (range: 27.25–137.66) and 9.73 pg/mL (range: 0–17.25) before treatment and 1 week after treatment (P = 0.023), respectively. The median level of IL-36β was 4.00 pg/mL (range: 2.74–27.38) and 0 pg/mL before treatment and 1 week after treatment (P = 0.043), respectively. The median level of IL-36γ was 26.82 pg/mL (range: 1.63–92.32) and 5.98 pg/mL (range: 0–15.20) before treatment 1 week after treatment (P = 0.097), respectively (Figure 2). Meanwhile, IL-17A, IL-17C, IFN-γ, TNF, IL-6, and IL-8 levels decreased 1 week after treatment. Among them, IL-17A, IL-17C, and IL-6 levels decreased significantly (P = 0.004, P = 0.001, and P = 0.001, respectively) (Figure 3).
 |
Figure 2 The concentrations of IL-36α, IL-36β, and IL-36γ before treatment and after one-week treatment with spesolimab. GPP_pre, means before treatment; GPP_post, means after one week with a single dose of spesolimab administration; * means P≤0.05. |
 |
Figure 3 The levels of IL-17A, IL-17C, IFN-gamma, TNF, IL-6, and IL-8 before treatment and after one-week treatment with spesolimab. GPP_pre, means before treatment; GPP_post, means after one week with a single dose of spesolimab administration; * *means P≤0.01; *** means P≤0.001. |
No relapse occurred 2 to 8 months after treatment. One patient experienced an upper respiratory infection in the first week following spesolimab administration and improved rapidly on regular antibiotics. No other adverse event was recorded.
Discussion
GPP treatment is a challenge, especially in children. Concerning the efficacy and safety, biologics are a favorable option compared with conventional oral treatment in adults.9–11 However, data on the use of biologics in children is scarce, especially those under 12 years.
Spesolimab could ameliorate GPP lesions rapidly. A multicenter, double-blinded, placebo-controlled trial (Effisayil 1) showed that 54% and 43% spesolimab-treated adults with GPP achieved GPPGA pustulation subscore 0 and GPPGA0/1, respectively, at week 1.12 After subgroup analysis considering Chinese patients in Effisayil 1, the percentages rose to 60% and 60% for GPPGA pustulation subscore 0 and GPPGA0/1, respectively.13 The finding of real-world studies were consistent with those of randomized controlled trials (RCTs) (Table 2).14–20 Our study is the first spesolimab-treatment report involving GPP patients under 12 years. All our five participants had a GPPGA pustulation subscore of 0 and GPPGA0/1 at week 1. In contrast to findings from the RCTs and real-world studies, spesolimab might result in better clearance of lesions in children. Few studies evaluated its effect on body temperature. Ran et al17 found that the body temperature normalized 2 and 5 days after spesolimab administration in two patients presenting with fever. In our five participants, the body temperature reduced to ≤38°C after the median of 2 days, and normalized after the median of 4 days, while one patient experienced rapid relief. After 1 week, WBC and CRP levels significantly reduced in all patients. Those proposed systemic inflammation may rapidly improve in patients with GPP after spesolimab administration. As shown by other reports, spesolimab was effective in our five patients irrespective of the presence of IL-36RN mutations.12,21
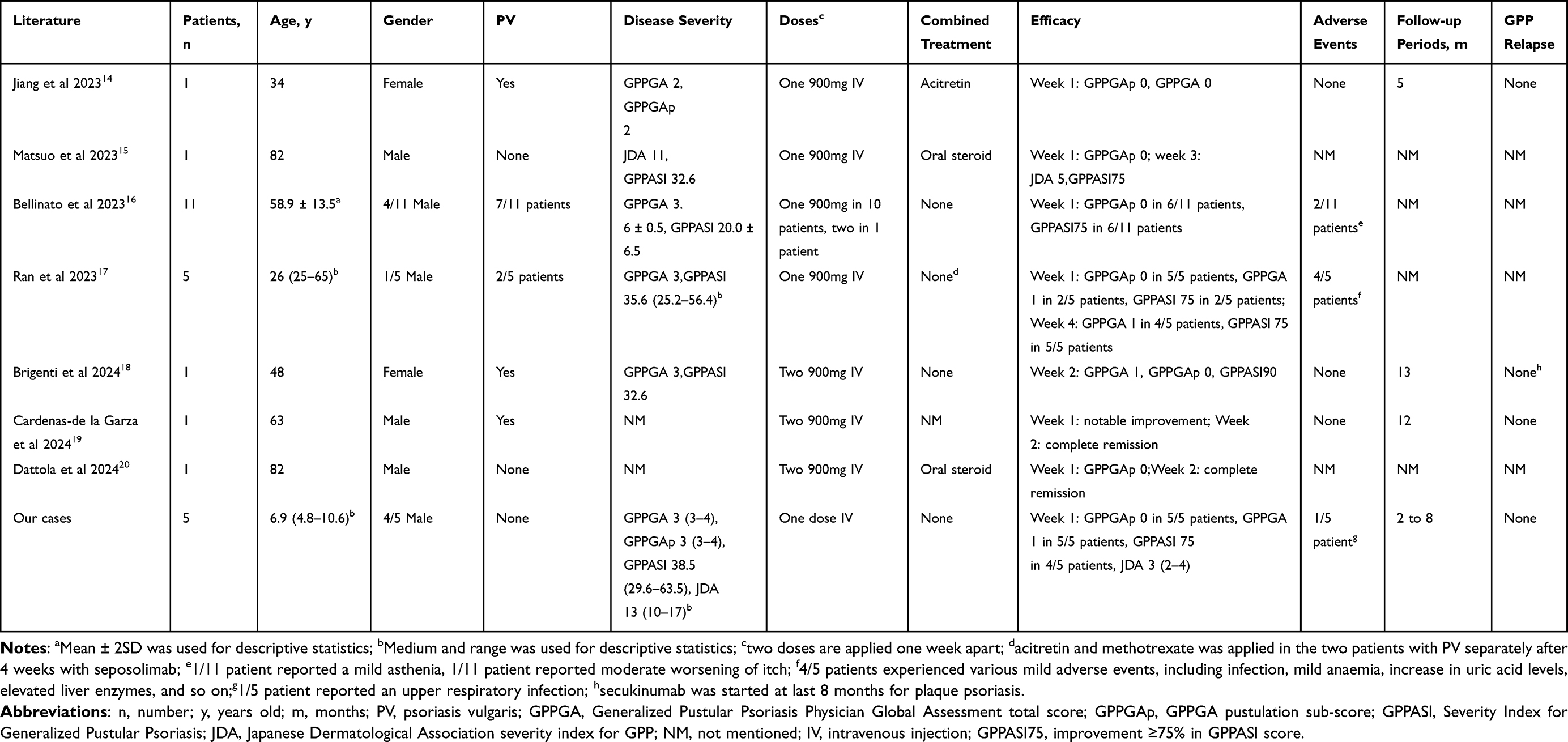 |
Table 2 Real-World Studies of the Effectiveness and Safety of Spesolimab in Patients with GPP Flare |
A single dose of spesolimab could control the flare of GPP in our five children. However, this regimen could not be generalized to all participants. In the Effisayil 1 clinical trials, 12 of 32 patients who had persistent symptoms and 4 of 32 patients who had a recurrence of a flare received a second dose of spesolimab on day 8, and 4 of 32 patients received a standard-of-care escape treatment.12 In a real-world study including 11 patients, 1 patient received two doses of spesolimab.16 Mostly, GPP has a relapse-remission course or its persistent. Thus, long-term treatment might be required to control or prevent flares. Effisayil 2 clinical trials assessed different models of spesolimab administration to prevent GPP flare after 48 weeks of observation and found that high-dose spesolimab (600 mg loading dose followed by 300 mg every 4 weeks) might be a promising option to prevent GPP flares.21
Our study showed that IL-36α, IL-36β, and IL-36γ levels were all decreased after spesolimab administration, with a significant decrease in IL-36α and IL-36β. Moreover, downstream cytokines and chemokines levels, including IL-17A, IL-17C, and IL-6 also decreased. IL-36 cytokines, including IL-36α, IL-36β, and IL-36γ, could cause a positive feedback loop in an autocrine or paracrine manner.22 Spesolimab is an IL-36R inhibitor that decreases IL-36 cytokines levels by suppressing IL-36 signaling pathway. Those elucidated IL-36 and related inflammatory storm could decrease through inhibiting IL-36Rs.
Spesolimab was well tolerated by our five participants. Patients presented mild adverse effects without death or hypersensitivity events. The tolerance of sepesolimab was also shown in other trials in adult or children above 12 years old. According to a Phase 2 RCT, the rates of adverse events were similar in spesolimab and placebo groups during the one-week and 48-week observation periods.12,21 However, the incidence of infections was indeed higher in the spesolimab group (17% vs 6%) during the one-week trial,12 and the proportion of serious adverse events was greater during the 48-week trial (10% vs 3%).21 The adverse events in real-life studies were mainly mild infection, anemia, asthenia, and raised uric acid levels and liver enzymes.16,23 However, data on real-life experiences and long-term research assessing its safety profile are limited.24 Thus, further studies in diverse populations, using different research methods, and with long-term spesolimab administration are required.
Above all, our five pediatric GPP patients showed a good response to a single dose of spesolimab. However, due to the small sample size, absence of control groups, and short follow-up period, high evidence-level trials are required to confirm our findings.
Abbreviation
GPP, Generalized pustular psoriasis; CRP, C-reactive protein; NF-κB, nuclear factor-κB; MAPK, mitogen-activated protein kinase; FDA, US food and drug administration; EMA, European medicines agency; CFDA, China food and drug administration (CFDA); BSA, Body surface area; GPPGA, Generalized pustular psoriasis physician global assessment; GPPASI, Severity Index for Generalized pustular psoriasis; JDA, Japanese dermatological association severity index for GPP; PEA, proximity extension assay; NPX, Normalized protein expression; WBC, White blood count; SAEs, Serious Adverse Events.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
Informed consent was obtained from all participants’ parents. The study complies with the Declaration of Helsinki.
Ethical Approval
Reviewed and approved by Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health ([2024]-E-102-R).
Funding
The study was funded by the National Key R&D Program of China (2023YFC2508101) and the Beijing Hospitals Authority’s Ascent Plan (DFL20241201).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Navarini AA, Burden AD, Capon F, et al. European consensus statement on phenotypes of pustular psoriasis. J Eur Acad Dermatol Venereol. 2017;31(11):1792–1799. doi:10.1111/jdv.14386
2. Wang Y, Cheng R, Lu Z, et al. Clinical profiles of pediatric patients with GPP alone and with different IL36RN genotypes. J Dermatological Sci. 2017;85(3):235–240. doi:10.1016/j.jdermsci.2016.11.008
3. Wang Z, Xiang X, Chen Y, et al. Different clinical features of pediatric generalized pustular psoriasis in patients with or without IL36RN variants. Dermatology. 2022. doi:10.1159/000528753
4. Yang SF, Lin MH, Chou PC, et al. Genetics of Generalized Pustular Psoriasis: current Understanding and Implications for Future Therapeutics. Genes. 2023;14(6). doi:10.3390/genes14061297
5. Bernardo D, Thaci D, Torres T. Spesolimab for the treatment of generalized pustular psoriasis. Drugs. 2024;84(1):45–58. doi:10.1007/s40265-023-01988-0
6. Iznardo H, Puig L. Exploring the role of IL-36 cytokines as a new target in psoriatic disease. Int J Mol Sci. 2021;22(9). doi:10.3390/ijms22094344
7. Fujita H, Terui T, Hayama K, et al. Japanese guidelines for the management and treatment of generalized pustular psoriasis: the new pathogenesis and treatment of GPP. J Dermatol. 2018;45(11):1235–1270. doi:10.1111/1346-8138.14523
8. Okorie CL, Nayudu K, Nambudiri VE. Cutaneous findings and treatments in deficiency of interleukin-36 receptor antagonist (DITRA): a review of the literature. Exp Dermatol. 2024;33(1):e14934. doi:10.1111/exd.14934
9. Miyachi H, Konishi T, Kumazawa R, et al. Treatments and outcomes of generalized pustular psoriasis: a cohort of 1516 patients in a nationwide inpatient database in Japan. J Am Acad Dermatol. 2022;86(6):1266–1274. doi:10.1016/j.jaad.2021.06.008
10. Takeichi T, Akiyama M. Generalized pustular psoriasis: clinical management and update on autoinflammatory aspects. Am J Clin Dermatol. 2020;21(2):227–236. doi:10.1007/s40257-019-00492-0
11. Chen Y, Xiang X, Wang Z, Miao C, Xu Z. The update of treatment strategies in pediatrics with generalized pustular psoriasis in China. Pediatr Investig. 2023;7(3):191–198. doi:10.1002/ped4.12395
12. Bachelez H, Choon SE, Marrakchi S, et al. Trial of spesolimab for generalized pustular psoriasis. N Engl J Med. 2021;385(26):2431–2440. doi:10.1056/NEJMoa2111563
13. Tsai TF, Zheng M, Ding Y, et al. Efficacy and safety of spesolimab in patients with generalized pustular psoriasis: a subgroup analysis of Chinese patients in the Effisayil 1 trial. Dermatol Ther. 2023;13(12):3097–3110. doi:10.1007/s13555-023-01037-4
14. Jiang M, Li Y, Guan X, Li L, Xu W. Rapid response of spesolimab in biologics - failure patient with generalized pustular psoriasis flare. Postepy Dermatol Alergol. 2023;40(4):584–586. doi:10.5114/ada.2023.129514
15. Matsuo M, Niwa H, Onishi H, Iwata H. A case of generalized pustular psoriasis with discrepant resolution time between pustules and erythema after treatment with spesolimab. J Dermatol. 2023. doi:10.1111/1346-8138.17032
16. Bellinato F, Gisondi P, Dattola A, et al. Spesolimab in patients with flare of generalized pustular psoriasis: a multicentre case-series. J Eur Acad Dermatol Venereol. 2023. doi:10.1111/jdv.19678
17. Ran D, Yang B, Sun L, et al. Rapid and sustained response to spesolimab in five Chinese patients with generalized pustular psoriasis. Clin Exp Dermatol. 2023;48(7):803–805. doi:10.1093/ced/llad108
18. Brigenti N, Gisondi P, Bellinato F, Girolomoni G. Generalized pustular psoriasis successfully treated with spesolimab: a case report. SAGE Open Med Case Rep. 2024;122050313X241235451. doi:10.1177/2050313X241235451
19. la Garza JA C-D, Zazueta-Lopez RM, Garza-Elizondo AK, Flores-Gutierrez DP, Welsh E. Spesolimab treatment in a patient with generalized pustular psoriasis: a case report with 12-month follow-up and literature review. Clin Exp Dermatol. 2024;49(3):286–288. doi:10.1093/ced/llad389
20. Dattola A, Taliano A, Rallo A, Pellacani G, Richetta AG. Spesolimab for the treatment of generalized pustular psoriasis: real life experience. Ital J Dermatol Venerol. 2024;159(1):61–62. doi:10.23736/S2784-8671.23.07628-4
21. Morita A, Strober B, Burden AD, et al. Efficacy and safety of subcutaneous spesolimab for the prevention of generalised pustular psoriasis flares (Effisayil 2): an international, multicentre, randomised, placebo-controlled trial. Lancet. 2023;402(10412):1541–1551. doi:10.1016/S0140-6736(23)01378-8
22. Marrakchi S, Puig L. Pathophysiology of generalized pustular psoriasis. American Clinical Dermato. 2022;23(Suppl 1):13–19. doi:10.1007/s40257-021-00655-y
23. Elewski BE, Lebwohl MG, Anadkat MJ, et al. Rapid and sustained improvements in generalized pustular psoriasis physician global assessment scores with spesolimab for treatment of generalized pustular psoriasis flares in the randomized, placebo-controlled Effisayil 1 study. J Am Acad Dermatol. 2023;89(1):36–44. doi:10.1016/j.jaad.2023.02.040
24. Potestio L, Camela E, Cacciapuoti S, et al. Efficacy and safety of spesolimab for the management of generalized pustular psoriasis: a drug safety evaluation. Expert Opin Drug Saf. 2023;22(11):1003–1010. doi:10.1080/14740338.2023.2265295
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Generalized Pustular Psoriasis with Cushing’s Syndrome: A Case of Effective Spesolimab Treatment
Peng G, Zhang Y, Zhang S, Li Y, Luo L, Luo J, Nie X, Zhang H, Liao C
Biologics: Targets and Therapy 2025, 19:321-329
Published Date: 10 May 2025
Achieving Therapeutic Success with Spesolimab: Two Cases of Drug-Induced Generalized Pustular Psoriasis Initially Mimicking Acute Generalized Exanthematous Pustulosis
Chen J, Xia Y, Zhou F, Tao J, Zhou N
Journal of Inflammation Research 2025, 18:9581-9585
Published Date: 19 July 2025