")
Back to Journals » Research and Reports in Urology » Volume 17
Surgical Management of Anterior Urethral Stricture: A 23-year Single-Center Study
Authors Guo Y, Ma N, Zhang J, Chen S, Liu P, Yang Z, Li Y
Received 18 November 2024
Accepted for publication 4 February 2025
Published 19 February 2025 Volume 2025:17 Pages 31—42
DOI https://doi.org/10.2147/RRU.S507169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Guglielmo Mantica
Yilong Guo,1,* Ning Ma,2,* Jiaxiong Zhang,3 Sen Chen,2 Pingping Liu,1 Zhe Yang,2 Yangqun Li1
1Department of Comprehensive Plastic Surgery, Plastic Surgery Hospital of Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Hypospadias Plastic Surgery, Plastic Surgery Hospital of Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3Department of Geriatric Medicine, Coronary Circulation Center of Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yangqun Li, Department of Comprehensive Plastic Surgery, Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 33 Badachu Road, Beijing, People’s Republic of China, Tel +86 13501210314, Email [email protected]
Purpose: Anterior urethral stricture is a common clinical condition in urology with significant socioeconomic impacts and is associated with high recurrence rates of and postoperative complications. However, the long-term outcome of surgical management of urethra stricture and the associated risk factors of stricture recurrence remain limited. We conducted a 23-year single-center retrospective study to evaluate the long-term surgical outcomes of anterior urethral strictures with different clinical characteristics and to study factors that contribute to stricture recurrence.
Methods: A retrospective study was conducted on 145 male patients diagnosed with anterior urethral stricture, who underwent meatotomy, anastomotic urethroplasty (AU), penile skin flap urethroplasty (PFU), single-stage buccal mucosa grafting (SSU), or multistage buccal mucosa grafting (MSU) between April 2000 and August 2023. We defined 100 months as the cut-off time point to distinguish short-term and long-term follow-up. Early surgical complications were scored using the Clavien-Dindo classification at 3 months. Patient-Reported Outcome Measure (PROM) was applied to evaluate surgical success. Risk factors for wound complications were evaluated using univariable and multivariable analysis.
Results: The overall mean stricture length was 2.3 ± 1.8 cm (a range of 0.3– 7.0). Stricture locations were at the meatus, fossa navicularis, penile, bulbar, and multifocal in 15, 36, 79, 9, and 6. The short-term and long-term success rate for meatotomy, AU, PFU, SSU, and MSU were 70.0%/80%, 70.4%/62.5%, 77.8%/69.2%, 100%/75%, and 81.8%/66.7%, respectively. The early complications classified as Clavien grades I, II, III, IV, and V were 39, 5, 5, 0, and 0. The late complication rate in the short-term and long-term groups were 20.3% and 30.3% (p > 0.05). The satisfaction survey showed that 74.5% (108 of 145) patients were satisfied or very satisfied with the surgical result. There was no statistically significant difference in stricture-free survival among the five surgical groups (Log rank test: χ² = 3.83, p > 0.05). The binary univariate logistic regression analysis showed that stricture symptom duration (p < 0.05) and previous urethroplasty (p < 0.05) were independent predictors of surgery failure.
Conclusion: This long-term retrospective study on male anterior urethral stricture disease demonstrates that surgical management is an effective and functional treatment. However, the success rate of urethroplasty shows a declining trend with longer follow-up. Stricture symptom duration and previous urethroplasty carry a high risk of surgical failure.
Keywords: anterior urethral stricture, complication, reconstructive surgical procedures, urethra, urethroplasty
Introduction
Anterior urethral stricture is a challenging urological condition affecting 296/100,000 men characterized by abnormal fibrosis of the corpus spongiosum.1 The male anterior urethra can be divided into the meatus, fossa navicularis, penile urethra, and bulbous urethra, and anterior urethral stricture can be single, multiple, or even panurethral.2 The narrowing of the urethra lumen can cause dysuria, acute urinary retention, and urinary tract infection (UTI).3 Stricture recurrence often occurs after endoscopic or surgical treatments, which can cause a tremendous financial burden and negative impact on the patient’s quality of life.4
At present, urethroplasty is considered the golden standard management for treating anterior urethral stricture, a large number of studies were conducted to assess the outcomes of urethroplasty techniques in the management of anterior urethral stricture.5–10 However, given the cause, etiology, location, number, and severity of male anterior stricture disease, the surgical option can be varied, and there is no universal agreement upon the reconstructive strategy of anterior urethral stricture.11 Despite numerous studies conducted to describe the techniques we used, there are only a few that have conducted long-term follow-ups for more than 10 years in such a large series.
To provide evidence for selecting urethroplasty techniques based on stricture characteristics and to evaluate long-term surgical outcomes in a large patient cohort, we retrospectively analyzed patients who underwent meatotomy, anastomotic urethroplasty (AU), penile skin flap urethroplasty (PFU), single-stage buccal mucosa urethroplasty (SSU), and multi-stage buccal mucosa urethroplasty (MSU) at our center.
Materials and Methods
Study Design
This retrospective analysis was approved by the institutional ethics review board of Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College. A total of 145 male patients diagnosed with anterior urethral stricture who underwent surgery between April 2000 and August 2023 were retrospectively studied in this study. The medical information was collected including patient demographic information, urethra stricture feature, surgical technique, and postoperative follow-up information. Patients who were lost to follow-up without complete postoperative follow-up information, those with posterior urethral stricture, those who did not undergo a second-stage surgery, and those whose urination could not be reasonably assessed due to other medical conditions were excluded. All the surgeries were led by the chief surgeon (LYQ) of the Hypospadias Center, who has over 40 years of experience in performing complex urological surgeries, particularly in hypospadias repair and anterior urethral strictures. All the surgeries were assisted by Associate Chief Surgeons Dr. YZ and Dr. MN, along with junior resident physicians.
Surgical Approach
Meatotomy
Two types of meatotomy were conducted in 15 patients with short distal meatus stricture. The mean stricture length is 0.5 ± 0.2 cm. A dorsal meatotomy is conducted to open the narrowed meatus by designing a Y-V plasty. A Y-shaped incision on the dorsal urethra meatus was made with the apex of the V inserted into the urethra. Then, mobilize the edges of the Y flap by sharp dissection and insert the glans flap into the opened urethra meatus to increase the width of the external urethral orifice. Then, suture the edges of the glans flap and urethra with a 6/0 absorbable suture.
Anastomotic Urethroplasty
Short fossa navicularis, penile, and bulbar strictures were treated with urethra stricture excision and anastomotic urethroplasty in 51 patients. The mean stricture length is 1.1 ± 0.8. The stricture segment of the urethra is dissected completely. After mobilizing the distal and proximal urethra, a 12F Foley catheter was placed to support the neourethra, and the edge of the urethra mucosa on both sides was continuously sutured with a 5/0 absorbable suture. The dartos fascia on both sides of the urethra was interruptedly sutured to wrap the urethra, and the skin was closed with 4/0 silk sutures. A suprapubic cystostomy was conducted for urinary diversion.12
Penile Skin Flap Urethroplasty
Penile urethral stricture or long penile or bulbar urethral stricture in 22 patients with adequate prepuce skin volume were treated with PFU. The mean stricture length is 2.2 ± 1.1 cm. Mobilize the edge of the lesion and completely dissect the urethra stricture from the surface down to the healthy underlying corpus spongiosum. Penile skin flap size was carefully designed by measuring the urethra defect and carefully mobilized and raised with the pedicle. Then, transpose the flap without tension and fixed with 4–0 absorbable sutures.13,14
Single-Stage Buccal Mucosa Grafting
We conducted the dorsal inlay buccal mucosa grafting technique in 5 patients with long fossa navicularis, penile, or bulbar strictures that cannot be anastomosis without tension. The mean stricture length is 2.1 ± 0.9 cm. A ventral incision was made directly in the midline of the penis at the stricture level and completely resected about 1 to 2 cm to the proximal and distal healthy urethra. The margins of the dorsal urethra were dissected from the tunica albuginea, and the free margins were interrupted and sutured to the tunica albuginea. The mucosa graft was sutured to the underlying tunica albuginea at several points and the margins of the graft were interruptedly sutured to the edges of the incised urethra, and then the urethra was sutured over a 12F Foley catheter.15
Multistage Buccal Mucosa Urethroplasty
Multistage buccal mucosa urethroplasty was conducted in 52 patients with long strictures that lacked an intact corpus spongiosum or urethral plate. The mean stricture length is 4.1 ± 1.5 cm. In the first stage, two pieces of buccal mucosa were harvested from either cheek of the patient. After trimming the redundant subcutaneous tissue, the buccal mucosa was longitudinally and continuously sutured around the gauze roll to form the neourethra. After fully dissecting the fibrotic tissue, the mucosa graft was inserted into the ventral penis and sutured on the vascularized bed with both ends interruptedly sutured on the distal and proximal meatus. All the patients were catheterized with a 12F Foley catheter through the proximal urethral orifice and placed in a compressive dressing surrounding the penis. The compressive dressing and Foley catheter were removed on the seventh postoperative day.
The second stage of surgery is performed at least 6 months after the first stage of surgery. The margin of the buccal mucosa graft is marked and incised, after carefully raising the edges of the mucosa, and we created the neourethra by continuously suturing the mucosa over a 12F Foley catheter. Then, rise and interruptedly suture the dartos fascia and skin to cover the primary suture line. A suprapubic cystostomy was conducted for urinary diversion.16
Follow-up
The duration of clinical symptoms is defined as the time from the onset of urethral stricture symptoms, such as poor stream, spraying, and incontinence, to the time when the patient underwent urethral stricture surgery at our institution. For the evaluation criteria of surgical success, we referred to the assessment of the urinary stream in the Patient-Reported Outcome Measure (PROM) for Urethral Stricture Surgery.17 The patients were asked, “Over the past 4 weeks, would you say that the strength of your urinary stream is…” and provided with five options: A) Normal, B) Occasionally reduced, C) Sometimes reduced, D) Reduced most of the time, and E) Reduced all of the time. Only patients reporting ‘Normal’ were defined as having surgical success, while any other responses aside from ‘Normal’ were classified as surgical failure. The available causes of surgical failure, such as stricture recurrence, fistula formation, ejaculatory pain, and spraying, were also documented in our study. Early postoperative complications were reported using the Clavien–Dindo classification, which has been validated and shown to be reproducible in the field of reconstructive urology.18 Long-term and short-term follow-up are characterized by follow-up of more than and less than 100 months.
Statistical Analysis
Descriptive statistics focused on the frequencies and proportions of categorical variables. Continuous variables are summarized as median (interquartile range). Univariable and multivariable logistic regression models were used to determine independent predictors of failure after urethroplasty. Continuous variables were transformed into categorical variables for analysis. Data were analyzed using the computer program Statistical Package for Social Sciences SPSS version 17.0 (SPSS Inc., Chicago, Ill., USA). The P value is considered significant if <0.05.
Results
A total of 145 male patients were included in our research. The number of patients in the short-term and long-term groups was 69 and 76, respectively. The mean age of the patients was 36.6 ± 14.4 years (a range of 18−71). The mean stricture length was 2.3 ± 1.8 cm (a range of 0.3–7.0). Patient demographic details are summarized in Table 1. The overall success rate in a mean follow-up time of 8.9 ± 5.3 years (a range of 0.1–22.7) was 71.0%. The short-term and long-term success rates were 75.4% and 67.1% (p > 0.05). The overall early complication rate was 32.4% (47 in 145), and the most common early complication is wound pain, wound edema, and wound infection reported in 19 (40.4%), 18 (38.2%), and 5 (10.6%) patients. According to Clavien-Dindo classification of early surgical complications, 83.0% (39 of 47) were classified as Clavien grade I, 10.6% (5 in 47) were classified as Clavien grade II, 10.6% (5 in 47) patients were classified as Clavien grade III, and there were no Clavien grade IV–V complications occurred in our research. The overall late complication was 23.5% (34/145), the most common late complication is spraying in 14 (41.2%), followed by fistula in 8 (23.5%), postvoid residual urine in 8 (23.5%), erectile dysfunction in 6 (17.7), penile lump in 3 (8.8%), and ejaculatory pain in 1 (2.9%).
 |
Table 1 Patient Demographics |
 |
Table 2 Stricture Location-Based Follow-up Data |
The surgical success rates for meatotomy, AU, PFU, SSU, and MSU were 73.3%, 66.7%, 72.7%, 80%, and 73.1% in a mean follow-up of 7.2 ± 5.4, 8.1 ± 5.3, 10.2 ± 6.5, 11.9 ± 4.5, and 9.5 ± 4.7 years. The short-term and long-term success rate for each surgery type: meatotomy (70.0% and 80%), AU (70.4% and 62.5%), PFU (77.8% and 69.2%), SSU (100% and 75%), and MSU (81.8% and 66.7%). The difference in stricture-free survival curves between the five surgical groups was not statistically significant. The Kaplan–Meier curve and the number at risk for each point were conducted (Log rank test: chi-square 3.83; p = 0.43) (Figure 1). The satisfaction score is 4.1 ± 1.5, 3.8 ± 1.6, 4.1 ± 1.4, 4.4 ± 1.3, and 4.1 ± 1.4, respectively. Clavien Grade I early complications were generally resolved without intervention or with simple conservative management such as wound pain, wound edema, wound bleeding, wound break down, cheek pain, and cheek edema. For Clavien Grade II early complications, wound infections were treated with wound dressing and intravenous antibiotics or oral medication, and bladder spasms were managed with anisodamine. Fistulas were graded as Clavien Grade III, four were resolved by wound dressing, and two fistulas required surgical intervention.
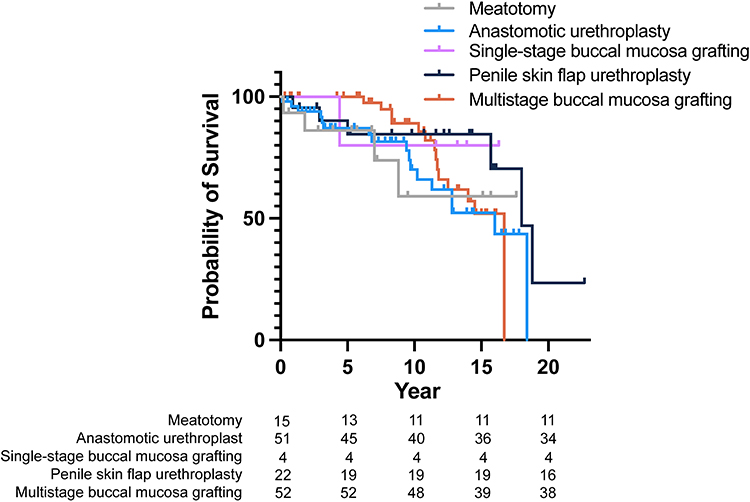 |
Figure 1 Kaplan–Meier curves regarding stricture-free survival by surgery type. |
The late complication rate in the short-term and long-term groups was 20.3% and 30.3% (p > 0.05). Spraying is the most common late complication on short-term and long-term groups occurred in 10.1% and 9.2% patients. In the meatotomy group, two patients reported normal voiding but significant de novo spraying, one reported stricture recurrence, and one reported fistula—all of which was surgically corrected. In the AU group, postvoid residual urine was reported in four patients, requiring manual extrusion. De novo spraying was observed in five patients, erectile dysfunction (ED) in two, and a minor penile lump during urination in one patient. All were well-tolerated, and the patients declined further surgery. Twelve cases of stricture recurrence, four chronic fistulas, and one case of ejaculatory pain were treated with urethroplasty. In the PFU group, two cases of spraying, one case of ED, and two cases of postvoid residual urine were well tolerated. Five cases of stricture recurrence and one case of fistula required surgical intervention. In the SSU group, one patient reported well tolerated spraying and one penile lump. One case of stricture recurrence received surgical correction. In the MSU group, four cases of de novo spraying, two cases of postvoid dribbling, three ED, and one penile lump were well tolerated without causing morbidity. No late oral complications were observed. Twelve stricture recurrences and two fistulas were considered failures and required additional surgery. Detailed surgical information related to stricture locations was summarized in Table 2.
 |
Table 3 Patency Rates According to Urethroplasty Technique, Location, and Failed Hypospadias |
Out of 145 patients, 100 patients with failed hypospadias had undergone previous hypospadias repair, with an average of 2.0 ± 0.9 procedures (range: 1–5), and were screened. The most common location of strictures was penile, followed by fossa navicularis, bulbar, meatus, and multifocal, affecting 65, 21, 7, 5, and 2 patients, respectively. Meatotomy was performed in 5 patients, AU in 40 patients, SSU in 5 patients, PFU in 7 patients, and MSU in 43 patients. The mean stricture length was 2.4 ± 1.8 cm (range of 0.3–7.0 cm). Surgical success was achieved in 69 patients (69%) with a mean follow-up of 9.0 ± 5.4 years (range of 0.1−18.8 years). No statistical differences were found between the surgery failure and the number of failed hypospadias. The patency rates are summarized in Table 3.
Binary univariate logistic regression analysis was conducted to evaluate the potential risk factors associated with surgical failure in anterior urethral stricture. On univariate analysis, stricture symptom duration, stricture in multiple locations, and previous urethroplasty were found significant for predicting stricture recurrence. On multivariate analysis, age at surgery, body mass index, symptom duration, stricture etiology, failed hypospadias, stricture number, stricture length, the presence of early complication, the use of graft, graft type, and graft size showed no association with surgery failure (p>0.05). Only stricture symptom duration (Hazard Ratio: 1.10 (1.05–1.16); p<0.05) and previous urethroplasty (Hazard Ratio: 6.81 (1.69–27.51); p<0.05) were found significant to predict recurrence. This result was confirmed with multivariable analysis after adjusting for stricture length, etiology, failed hypospadias, stricture symptom duration, and previous urethroplasty (Table 4).
 |
Table 4 Binary Logistic Regression Analysis to Identify Potential Risk Factors Associated with Surgery Failure |
Discussion
To our knowledge, this is one of the largest series to analyze the long-term surgical outcome of the anterior urethral stricture. There are limited studies on long-term follow-up for urethral stricture surgery, most of which are retrospective, with follow-up intervals chosen based on the characteristics of specific patient cohorts. Currently, there is no established optimal follow-up window for postoperative monitoring of urethral stricture. Our study found a trend toward a decrease in success rates for urethral stricture surgery over long-term follow-up compared to short-term follow-up. This finding provides a theoretical basis for refining follow-up intervals to more accurately assess stricture success rates. With larger patient datasets in the future, establishing a more precise follow-up timeframe could better support the choice of surgical techniques, assess the surgical outcomes, and risk factors related to recurrence.
The surgical management of anterior urethral strictures aims to improve symptoms, reduce the risk of recurrence, and enhance quality of life. At present, there is still no consensus on the best objective or functional metrics to determine the success after urethroplasty.19 Various objective and subjective criteria are available for evaluating surgical success, but they vary across studies and journals. Anderson et al reported that the estimated 1- and 5-year success rates of urethroplasty varied significantly depending on the definition of surgical success, ranging from highest to lowest: retreatment, cystoscopy, uroflow, questionnaire, and any failure.20 For a traditional questionnaire survey, Tam et al reported that the International Prostate Symptom Score (IPSS), a stand-alone tool to detect urethral stricture recurrence following urethroplasty, is neither adequately sensitive nor specific enough to detect stricture recurrence.21 However, with the development of relevant qualitative metrics, patient-reported quantifiable changes have shown promising results in assessing surgical success, due to the advantages of clinical reliability, practicality, and cost-effectiveness. Jackson et al developed a valid PROM from expert opinion, literature review, and patient feedback, and an excellent correlation was shown between the voiding symptom scores and maximum flow rate.17 It is also reported that the urinary stream is a key parameter that is more sensitive to evaluating patients with cystoscope-confirmed stricture recurrence.21 Due to the absence of objective evaluation data in the early stages of our long-term study, and the lack of postoperative urodynamics data for comparison in some patients, we utilized urinary stream-based PROM alone to evaluate surgical success after urethroplasty. While PROM provides valuable insights, there are certain limitations to using it alone for evaluating surgical outcomes. PROM is particularly limited when patients sustain other obstructive conditions, such as benign prostatic enlargement (BPE). A variety of factors differ across patients and can potentially influence the validity and reliability of the research outcome. Additionally, discrepancies have been observed between patient-reported and physician-reported outcomes regarding the results of surgery for urethral stricture.
Localized meatal strictures can be initially treated by less invasive meatotomy, and the aesthetic outcome may be insufficient, but meatotomy can achieve single straight urinary stream with good meatus caliber in 97% patients apart from temporary dysuria in 38% patients.22 Malone et al reported that the construction of a slit-like urethra meatus with good cosmetic outcome and only occasional spraying. Therefore, completely excise the fibrosis structure and deepening the glans incision to create a slit-like urethra meatus to minimize the two long-term spraying in our meatotomy group is feasible.
Excision and primary anastomosis are widely regarded as the gold-standard reconstructive technique for patients, with short bulbar urethral strictures measuring less than 2 cm.23 Previous studies have reported success rates for anastomotic urethroplasty (AU) ranging from 91% to 98%.12,24 However, in our study, the success rate of AU was notably lower, achieving only 66.7%. Morey et al reported no statistically significant difference in success rates, stricture recurrence, or erectile complaints between proximal bulbar urethral strictures treated with AU for strictures measuring 3.78 cm in length (range 2.6–5.0 cm) and those measuring 1.5 cm in length (range 1.0–2.3 cm).25 While stricture length may not significantly impact outcomes in our research, by contrast, the history of dilation, prior surgery, or stricture-associated urethroplasty carries a high risk of spongiofibrosis. Among the 17 failed AU cases in our study, 16 patients had undergone a mean of 2.4 failed hypospadias (range 1–5), and 6 had previously received dilation or urethroplasty.26,27 Two patients who underwent AU reported erectile dysfunction (ED) with a mean recovery time of 4 months without additional intervention. Mundy et al primarily observed that ED following AU and graft urethroplasty is negligible. In a long-term follow-up of 260 patients who underwent AU for bulbar urethral strictures, newly developed ED occurred in only 6 patients (2.3%).28 Postoperative ED is thought to result from aggressive urethral dissection, which can damage the cavernous nerve.29
The controversy between using penile skin flap or buccal mucosa grafting has been debated for a long time. The reported patency rates between grafts and flaps were similar.30,31 Lumen et al reported a failure rate of PFU and MSU for 40.0 and 30.3% in a follow-up of 64.1 and 42.1 months.32 A higher success rate of 79.1% was achieved in a large cohort of 105 patients who underwent MSU, with a mean follow-up of 34.7 months (range: 10–58 months).33 The PFU carries its blood supply and requires only one stage to repair large defects, especially for recipient site with poor blood supply. Whitson et al also reported a decreasing tendency of the success rate of PFU at 1, 3, 5 and 10 years were 95%, 89%, 84% and 79%, respectively.34 In addition, PFU is associated with more postoperative complications such as skin necrosis, skin loss, and penile torsion.30 However, the total surgery time of MSU (209.0 ± 43.2) is significantly longer than PFU (114.2 ± 54.5) (P<0.05). MSU is associated with early oral complications in 15.4% (8/52) of patients in our research. We close the oral incision by interrupted closure, rinse the mouth with chlorhexidine acetate, and apply the liquid dressing daily. No long-term donor site complication was observed in all the patients. It was hypothesized that the distal meatus stricture could be attributed to a narrow distal tunnel design, inadequate tie-over dressing, and wound breakdown.
There are certain limitations to our research. First, retrospective research lacks a control group for comparing the outcomes of different reconstructive procedures and is subject to potential confounding variables, including demographic, clinical, and admission-related factors. Additionally, surgical success is assessed through a patient self-reported questionnaire following surgery, which may introduce recall bias. Furthermore, the inconsistent and incomplete data in the available medical records, written by various junior residents, raise concerns about potential data incompleteness. Second, the time span of our series is large, the surgical decision was made with the evolution of reconstructive theory, and might reflect minimal learning curve effects. The surgical outcome might be varied and require a more detailed analysis, but a larger patient number was required. Third, our study can only acquire observational outcomes and make descriptive analysis, and the identification of clinical indicators for improving the surgical outcome requires additional prospective and multi-institutional with larger patient samples and standardized outcome measurement. Fourth, the exclusion of patients lost to follow-up and those who did not undergo second-stage surgery is prone to introduce selection bias and overestimation of the success rates. Statistical adjustments for missing data or the standardized exclusion criteria may help mitigate this bias.
Conclusion
Our retrospective research shared our experience in the treatment of a large number of patients of anterior urethral stricture with different types of clinical characteristics. Our research adds to the body of literature supporting the effectiveness of surgical management of anterior urethral stricture and may provide a solid foundation and provoke the optimizing of patients’ surgical outcomes in the future. Identifying the risk factors associated with surgical failure can be highly valuable in preoperative surgery planning and improve overall outcomes.
Data Sharing Statement
The data are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was conducted in compliance with the principles outlined in the Declaration of Helsinki. Ethical approval was obtained from Plastic Surgery Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College. All participants provided written informed consent before their inclusion in the study.
Consent for Publication
Any images, videos, recordings, etc., in our manuscript can be published.
Collaborating Authors or Study Group Members
No collaborating authors or Study Group in the production of this work.
Acknowledgments
The authors thank Ken Hou for the professional comments on grammar usage and narration. Hao Yu, Dongliu Xiang, and Liwei Wang for the help in writing assistance. Zetian Li, Zhen Liu, Zhenpeng Zhu, Shiyuan Lu, and Hao Chen for the constructive advice on manuscript structure organization. Yaman Niu, Yuzhi Wu, Jiaqi Xu, Yangyang Ding, Yao Xiao, and Zikun Wan for their help in table design.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was conducted independently and did not receive any external funding.
Disclosure
All authors declare no competing interests.
References
1. Figler BD, Gore JL, Holt SK. et al. High regional variation in urethroplasty in the United States. J Urol. 2015;193(1):179–183. doi:10.1016/j.juro.2014.07.100
2. Lumen N, Campos-Juanatey F, Greenwell T, et al. European Association of Urology guidelines on urethral stricture disease (part 1): management of male urethral stricture disease. Eur Urol. 2021;80(2):190–200. doi:10.1016/j.eururo.2021.05.022
3. Tritschler S, Roosen A, Füllhase C, et al. Urethral stricture: etiology, investigation and treatments. Dtsch Arztebl Int. 2013;110(13):220–226. doi:10.3238/arztebl.2013.0220
4. Jackson MJ, Ivaz SL. Quality and length of life, money and urethral stricture disease. Curr Opin Urol. 2015;25(4):346–351. doi:10.1097/MOU.0000000000000179
5. Santiago JE, Gross MD, Accioly JP, et al. Decision regret and long-term success rates after ventral buccal mucosa graft urethroplasty. BJU Int. 2024;135(2):303–309. doi:10.1111/bju.16566
6. Oszczudlowski M, Yepes C, Dobruch J, et al. Outcomes of transecting versus non-transecting urethroplasty for bulbar urethral stricture: a meta-analysis. BJU Int. 2023;132(3):252–261. doi:10.1111/bju.16108
7. Hmida W, Othmen MB, Bako A, et al. Penile skin flap: a versatile substitute for anterior urethral stricture. Int Braz J Urol. 2019;45(5):1057–1063. doi:10.1590/s1677-5538.ibju.2018.0652
8. Steffens JA, Anheuser P, Treiyer AE, et al. Plastic meatotomy for pure meatal stenosis in patients with lichen sclerosus. BJU Int. 2010;105(4):568–572. doi:10.1111/j.1464-410X.2009.09172.x
9. Palminteri E, Gobbo A, Preto M, et al. The role of multi-staged urethroplasty in lichen sclerosus penile urethral strictures. J Clin Med. 2022;11(23):6961. doi:10.3390/jcm11236961
10. Lumen N, Monstrey S, Goessaert A-S, et al. Urethroplasty for strictures after phallic reconstruction: a single-institution experience. Eur Urol. 2011;60(1):150–158. doi:10.1016/j.eururo.2010.11.015
11. Zhang K, Wang T, Cao S, et al. Multi-factorial analysis of recurrence and complications of lingual mucosa graft urethroplasty for anterior urethral stricture: experience from a Chinese referral center. Urology. 2021;152:96–101. doi:10.1016/j.urology.2021.03.017
12. Santucci RA, Mario LA, McAninch JW. Anastomotic urethroplast y for bulbar urethral stricture: analysis of 168 patients. J Urol. 2002;167(4):1715–1719. doi:10.1016/S0022-5347(05)65184-1
13. Boccon-Gibod L, Le Portz B. One-stage urethroplasty for urethral stricture. Free full thickness skin graft versus cutaneous island flap urethroplasty. Eur Urol. 1984;10(1):32–35. doi:10.1159/000463507
14. Quartey JK. One-stage penile/preputial cutaneous island flap urethroplasty for urethral stricture: a preliminary report. J Urol. 1983;129(2):284–287. doi:10.1016/S0022-5347(17)52051-0
15. Asopa HS, Garg M, Singhal GG, et al. Dorsal free graft urethroplasty for urethral stricture by ventral sagittal urethrotomy approach. Urology. 2001;58(5):657–659. doi:10.1016/S0090-4295(01)01377-2
16. Kozinn SI, Harty NJ, Zinman L, et al. Management of complex anterior urethral strictures with multistage buccal mucosa graft reconstruction. Urology. 2013;82(3):718–722. doi:10.1016/j.urology.2013.03.081
17. Jackson MJ, Sciberras J, Mangera A, et al. Defining a patient-reported outcome measure for urethral stricture surgery. Europ urol. 2011;60(1):60–68. doi:10.1016/j.eururo.2011.03.003
18. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
19. Campos-Juanatey F, Osman NI, Greenwell T, et al. European Association of Urology guidelines on urethral stricture disease (part 2): diagnosis, perioperative management, and follow-up in males. Eur Urol. 2021;80(2):201–212. doi:10.1016/j.eururo.2021.05.032
20. Anderson KT, Vanni AJ, Erickson BA, et al. Defining success after anterior urethroplasty: an argument for a universal definition and surveillance protocol. J Urol. 2022;208(1):135–143. doi:10.1097/JU.0000000000002501
21. Tam CA, Elliott SP, Voelzke BB, et al. The International Prostate Symptom Score (IPSS) is an inadequate tool to screen for urethral stricture recurrence after anterior urethroplasty. Urology. 2016;95:197–201. doi:10.1016/j.urology.2016.04.006
22. Edan OA. Wedge urethral meatotomy in meatal stenosis secondary to web formation. J Pediatr Urol. 2022;18(3):334.e1–334.e6. doi:10.1016/j.jpurol.2022.02.022
23. Siegel JA, Panda A, Tausch TJ, et al. Repeat excision and primary anastomotic urethroplasty for salvage of recurrent bulbar urethral stricture. J Urol. 2015;194(5):1316–1322. doi:10.1016/j.juro.2015.05.079
24. Barbagli G, Guazzoni G, Lazzeri M. One-stage bulbar urethroplasty: retrospective analysis of the results in 375 patients. Eur Urol. 2008;53(4):828–833. doi:10.1016/j.eururo.2008.01.041
25. Morey AF, Kizer WS. Proximal bulbar urethroplasty via extended anastomotic approach--what are the limits? J Urol. 2006;175(6):2145–2149. [discussion 2149]. doi:10.1016/S0022-5347(06)00259-X
26. Roehrborn CG, McConnell JD. Analysis of factors contributing to success or failure of 1-stage urethroplasty for urethral stricture disease. J Urol. 1994;151(4):869–874. doi:10.1016/S0022-5347(17)35109-1
27. Verla W, Van Nieuwenhuyse F, Hoebeke P, et al. Urethroplasty for failed hypospadias repair related strictures in adults: a retrospective analysis with long-term follow-up. Urology. 2020;143:248–254. doi:10.1016/j.urology.2020.05.070
28. Eltahawy EA, Virasoro R, Schlossberg SM, et al. Long-term followup for excision and primary anastomosis for anterior urethral strictures. J Urol. 2007;177(5):1803–1806. doi:10.1016/j.juro.2007.01.033
29. Dogra PN, Singh P, Nayyar R, et al. Sexual dysfunction after urethroplasty. Urol Clin North Am. 2017;44(1):49–56. doi:10.1016/j.ucl.2016.08.013
30. Dubey D, Vijjan V, Kapoor R, et al. Dorsal onlay buccal mucosa versus penile skin flap urethroplasty for anterior urethral strictures: results from a randomized prospective trial. J Urol. 2007;178(6):2466–2469. doi:10.1016/j.juro.2007.08.010
31. Wessells H, McAninch JW. Current controversies in anterior urethral stricture repair: free-graft versus pedicled skin-flap reconstruction. World J Urol. 1998;16(3):175–180. doi:10.1007/s003450050048
32. Lumen N, Oosterlinck W, Hoebeke P. Urethral reconstruction using buccal mucosa or penile skin grafts: systematic review and meta-analysis. Urol Int. 2012;89(4):387–394. doi:10.1159/000341138
33. Selim M, Salem S, Elsherif E, et al. Outcome of staged buccal mucosal graft for repair of long segment anterior urethral stricture. BMC Urol. 2019;19(1):38. doi:10.1186/s12894-019-0466-4
34. Whitson JM, McAninch JW, Elliott SP, et al. Long-term efficacy of distal penile circular fasciocutaneous flaps for single stage reconstruction of complex anterior urethral stricture disease. J Urol. 2008;179(6):2259–2264. doi:10.1016/j.juro.2008.01.087
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.