")
Back to Journals » Clinical Ophthalmology » Volume 18
Surgical Outcomes of Children with Unilateral Congenital Cataract and Persistent Fetal Vasculature
Authors Loukovaara S
Received 5 June 2024
Accepted for publication 15 August 2024
Published 24 August 2024 Volume 2024:18 Pages 2387—2396
DOI https://doi.org/10.2147/OPTH.S472028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sirpa Loukovaara1,2
1Unit of Vitreoretinal Surgery, Department of Ophthalmology, Helsinki University Hospital, Helsinki, Finland; 2Individualized Drug Therapy Research Program, University of Helsinki, Helsinki, Finland
Correspondence: Sirpa Loukovaara, Unit of Vitreoretinal Surgery, Department of Ophthalmology, University of Helsinki and Helsinki University Hospital, Haartmaninkatu 4C, Helsinki, 00290, Finland, Tel +358-50-4271566, Email [email protected]
Purpose: To delineate the characteristics, surgical interventions, and visual outcomes among children diagnosed with congenital cataract and persistent fetal vasculature (PFV).
Patients and Methods: Retrospective observational single-center study was conducted between January 1, 2009, and December 31, 2019, at Helsinki University Hospital. The national cohort encompassed 82 children aged from birth to 15 years who underwent lensectomy, 3-port vitrectomy, or a combined procedure, with the objective of achieving visual rehabilitation. Among the surgical cohort, paediatric cases with International Classification of Disease (ICD-10) codes Q14.0 for PFV and Q12.0 for congenital cataract were identified and analyzed. Data were collected through a comprehensive review of medical records, encompassing clinical history (birth weight), gender distribution, ocular parameters (laterality, intraocular pressure [IOP], visual acuity [VA]), details of cataract and vitreoretinal surgical interventions, indications for surgery, postoperative ophthalmic complications, as well as evaluations of functional and anatomical outcomes.
Results: The cohort consisted of 11 children, ranging in age from 6 months to 12 years. Surgical intervention resulted in the attainment of at least light perception vision in nine of the operated eyes, representing 81.8% of cases. Among these, two eyes (18.2%) achieved hand motion vision, while 5 eyes (55.6%) achieved vision of finger counting or better. Additionally, two eyes (18.2%) achieved visual acuity measurable on the Snellen chart. However, one eye (9.1%) experienced complete vision loss, while the contralateral eye developed sympathetic ophthalmia.
Conclusions: Congenital cataract with PHV without anterior segment pathology associated with best postoperative VA, while eyes with anterior segment pathology or a complex posterior segment pathology had poor visual prognosis. Case selection for surgery is considered of great importance, since sympathetic ophthalmia may occur postoperatively. Understanding more deeply pathogenesis of PFV is warranted.
Keywords: tractional retinal detachment, pediatric ophthalmology, congenital eye disorders, ocular abnormalities, visual impairment, retinal surgery
Introduction
Congenital cataract with persistent fetal vasculature (PFV) represents a complex and challenging condition in paediatric ophthalmology. PFV, formerly known as persistent hyperplastic primary vitreous, is a rare developmental anomaly characterized by incomplete regression of the primary vitreous and embryonal hyaloid vasculature, leading to a spectrum of ocular abnormalities, including cataract and retinal detachment.1,2 In the worst case, the persistent hyaloidal stalk is integrated anteriorly into the posterior lens capsule and posteriorly to the vascular bundle of the optic nerve head (ONH) and exerts tractional forces radially in all directions.3 Ultimately, tractional retinal detachment (TRD) may occur due to retrolental fibrovascular tissue proliferation and contraction.4 In PFV eyes, concomitant retrolental stalk, avascular peripheral retina, and regional capillary dropout have been observed with fluorescein angiography examination.5
The management of unilateral congenital cataract with PFV poses unique therapeutic challenges. Surgical intervention is often required to address the congenital cataract and associated PFV-related anterior and/or posterior segment complications, with techniques such as lensectomy, vitrectomy, membranectomy, and retinal detachment repair.6,7 And in many cases multiple surgical interventions are needed. However, in cases with advanced pathology, including ONH hypoplasia, severe tractional retinal detachment, or microphthalmia, surgery is generally not a preferred choice since post-operative vision is often modest.8 Postoperatively, achieving optimal visual outcomes in the PFV cases can be hindered by factors including amblyopia, nystagmus, glaucoma, proliferative vitreoretinopathy (PVR), and refractive errors. Case selection for surgical treatment is of great importance, since long-standing complications such as sympathetic ophthalmia, ie, bilateral granulomatous panuveitis, may occur postoperatively and need to be considered.9,10
In this real-world single-centre study, the aim was to provide a comprehensive overview of the clinical features, management strategies and final visual outcomes for eyes with unilateral congenital cataract and PFV. By elucidating the complexity of this rare paediatric condition, clinicians could enhance their understanding and improve the individually tailored management of affected children, ultimately optimizing visual outcomes and quality of life.
Material and Methods
Study Design and Cohort
Among the cohort of 82 paediatric patients, 11 paediatric cases (11 eyes) aged from birth to 15 years were diagnosed with International Classification of Disease (ICD-10) codes Q14.0 for PFV and Q12.0 for congenital cataract during an eleven-year study period, covering years from January 1st, 2009, to December 31st, 2019.
Register Data Sources and Data Collection
Case identification was through data collection via a tertiary eye clinic archive. Cases were reviewed for demographic and ophthalmic data, including ages at diagnosis and at the time of vitreoretinal surgical intervention, gender, eye involved (laterality), location of PFV, associated ocular abnormalities (microphthalmos, hypoplastic ONH, hypoplastic fovea, macular detachment, traction retinal detachment), postoperative visual acuity (VA), intraocular pressure (IOP), performed surgical procedures (combined vitrectomy and retinal procedure (CKD92); and combined phacoemulsification with or without intraocular lens (IOL) implantation together with PPV (CKD94) including reoperations), location of vitrectomy incisions (pars plicata or pars plana), late onset complications related to surgery (loss of the eye ball, secondary glaucoma, sympathetic ophthalmia), and length of post vitrectomy follow-up (in months).
Deeper demographic characteristics of the study children (eg consanguinity of parents, parents age at conception), or other antenatal history could not be checked from archives.
Diagnosis of congenital cataract and PFV was made based on a combination of clinical examination by biomicroscopy and/or indirect ophthalmoscopy as well as clinical examination performed under general anaesthesia documented with RetCam pediatric ocular imaging and ultrasound findings. In all PFV eyes, there was an elevated fibrovascular membrane or stalk from the ONH to the posterior lens capsule. A non-surgical follow-up was used in cases with non-central lens opacity and surgery was performed first when there was increasing development of cataract. Preoperatively, all children were evaluated by an experienced pediatric ophthalmologist, cataract surgeon and/or vitreoretinal surgeon to determine the timing of surgical intervention.
Children underwent lensectomy, 3-port vitrectomy, or combined lensectomy-vitrectomy procedure through a limbal or pars plicata/plana approach aimed at visual rehabilitation. Vitrectomies were performed through the immature pars plicata or, in older children, through the pars plana approach. The postoperative IOL power was targeted for hyperopia.
Post vitrectomy, all operated eyes were followed by Optos ultra-widefield (UWF™, Nikon Co. Ltd, Japan) retinal imaging and by table mounted Optical Coherence Tomography imaging (Heidelberg Engineering, Heidelberg Engineering GmbH).
In infants, the fixation patterns were recorded, but in older children VA was assessed with age-appropriate Snellen test, hand movement (HM), finger counting (FC), or light perception (LP).
Ethics
The study was approved by the HUH (HUS/58/2020) and central hospital’s Institutional Review Boards and adhered to the tenets of the Declaration of Helsinki. Informed consent was waived due to retrospective register-based design of the study. Register-based patient data was handled with confidentiality.
Statistical Analysis
All data analysis was performed with Excel. Since the study children received individually tailored management, no statistics could be performed.
Results
The present study comprised eleven children, each representing a single eye with unilateral congenital cataract and PFV, as described in Table 1. The mean birth weight of the cohort was 3589 grams, with a range spanning from 3230 to 4000 grams. Regarding ethnicity, all participants were of Finnish descent, except for one individual. Notably, all births occurred as full-term single pregnancies, with the sole exception being a full-term twin pregnancy. This case 11 (the A-twin) was diagnosed with pneumothorax, microphthalmos, and PFV immediately following birth (Table 2).
 |
Table 1 Characteristics of Children with Unilateral Congenital Cataract and Persistent Fetal Vasculature: Patient Data at Baseline Including Details of Anterior Segment Surgery |
 |
Table 2 Characteristics of Eyes with Unilateral Congenital Cataract and Persistent Fetal Vasculature: Type of Posterior Segment Vitreoretinal Surgeries |
Six children were born in Helsinki and Uusimaa hospital district, five cases elsewhere in Finland (Satakunta, Varsinais-Suomi, Kymenlaakso, Pohjois-Savo). Four out of eleven children (36.3%) exhibited microphthalmos, while one child (9.1%) presented with hypoplastic ONH, and another child (9.1%) displayed hypoplastic fovea. It is noteworthy that none of the children enrolled in the study exhibited documented systemic abnormalities (Table 1). PFV was identified in ten infants (91%) within the first 3 months of life, primarily manifesting through clinical indicators such as leukocoria, microphthalmos, and/or strabismus. In one instance, however, leukocoria was observed later, at the age of 8 months (Case 9).
One eye (Case 7) was diagnosed with secondary glaucoma and received intraocular pressure lowering medication prior to vitrectomy surgery. In addition, two eyes developed secondary glaucoma post vitrectomy.
Anterior Segment Surgery
Most children in the cohort were male (Table 1). Initially, four children underwent anterior segment phacoaspiration procedures, encompassing either lens suction or lensectomy. Among these four cases, two eyes underwent primary posterior capsulotomy. However, the primary posterior capsulotomy was not performed in Cases 6 and 11. Following anterior segment interventions, three eyes remained aphakic, while one eye received an intraocular lens (IOL) placed in the capsular bag (Case 5, Table 1). Notably, this case underwent anterior segment surgery twice, with the second procedure necessitated by the dislocation of the previously inserted IOL.
Combined Anterior and Posterior Segment Surgery
A combined anterior segment procedure involving phacoaspiration with or without IOL implantation, alongside posterior segment 3-port pars plicata/plana vitrectomy was undertaken in six children, as detailed in Table 2.
In total, among the eleven operated children included in the study, a foldable IOL was implanted in six cases, constituting 54.5% of the cohort. Specifically, five out of these six eyes received the three-piece ZA9003 IOL, while one eye was implanted with the single-piece ZCB00 hydrophobic acrylic IOL.
Out of eleven study eyes, one eye with TRD and subretinal fibrosis underwent vitrectomy with the adjunctive placement of an encircling band and silicone oil (SO) endotamponade (Case 1). Subsequently, the SO endotamponade was successfully removed after a period of 4 months, and the retina remained attached.
Surgery of PFV Stalk
Two out of the eleven eyes with persistent retrolental fibrovascular tissue connecting the ONH to the posterior lens capsule underwent endodiathermy (ED) as a preliminary measure to control intraocular bleeding before proceeding with stalk division (Case 6 and 11, Table 2). In the remaining nine eyes, the PFV stalk was severed using a vitrectomy probe without endodiathermy.
Child with Sympathetic Ophthalmia
One child presented with microphthalmos, PFV, and dense cataract from birth (Case 8). Due to the estimated unfavorable visual prognosis, this child underwent only monitoring until six months of age. Subsequently, vitrectomy surgery was pursued, albeit the eye had progressed to total TRD with tent-shaped funnel formation, resulting in complete loss of visual acuity (VA). At six months post vitrectomy, at the age of one year and two months, the contralateral healthy eye of this child developed sympathetic ophthalmia. Initially, treatment for sympathetic ophthalmia comprised systemic corticosteroids, followed by the administration of the biologic agent Humira® (adalimumab) at a dosage of 20 mg every second week subcutaneously, alongside Trexan® (methotrexate) at 5 mg systematically once a week. Finally, the microphtalmic vitrectomized SO filled blind eye was enucleated one year and 10 months post primary vitrectomy causing poor cosmesis and the contralateral eye with sympathetic ophthalmia encountered secondary glaucoma necessitating a glaucoma drainage implant (Molteno).
Reoperations
In addition to the case requiring enucleation, three other children necessitated reoperation in the vitreoretinal unit (Table 2). Among these three eyes, two eyes underwent reoperation due to complicated TRD (Case 1 and 7), while one required intervention for secondary cataract (Case 9). Out of these two eyes, Case 1 had undergone posterior capsulotomy at the time of cataract surgery (Table 1), but case 7 had undergone primary combined anterior and posterior segment surgery. Post vitrectomy, one eye underwent strabismus surgery as part of the comprehensive management approach (Case 10).
Postoperative Follow-Up and Visual Outcomes
The median length of postoperative follow-up after vitreoretinal surgery varied among the operated cases. Notably, two children (Cases 2 and 4, as detailed in Table 2) were lost to follow-up postoperatively, with their subsequent care managed elsewhere in another hospital district.
Postoperatively, the spherical equivalent was very differing among the operated cases (Table 2).
Surgical intervention provided at least light perception vision in nine (81.8%) of the operated eyes, out of which two eyes (18.2%) obtained HM, 5 eyes (55.6%) FC (Figure 1) or better vision and two eyes (18.2%) visual acuity on Snellen (Figures 2 and 3).
 |
Figure 1 A retinal image captured by Optos ultra-widefield ® presents a 7-year-old female patient with stalk PFV fibrous membrane over disc three years after vitrectomy in left eye (Case 5). No peripheral vascular abnormalities. The final visual acuity was finger counting. |
 |
Figure 2 A retinal image captured by Optos ultra-widefield ® presents a 9-year-old male patient with remnants of PFV over disc five years after vitrectomy in left eye (Case 10). Optic nerve head hypoplasia with peripapillary RPE mottling. No peripheral vascular abnormalities. The final visual acuity was 0.05 on Snellen testing. |
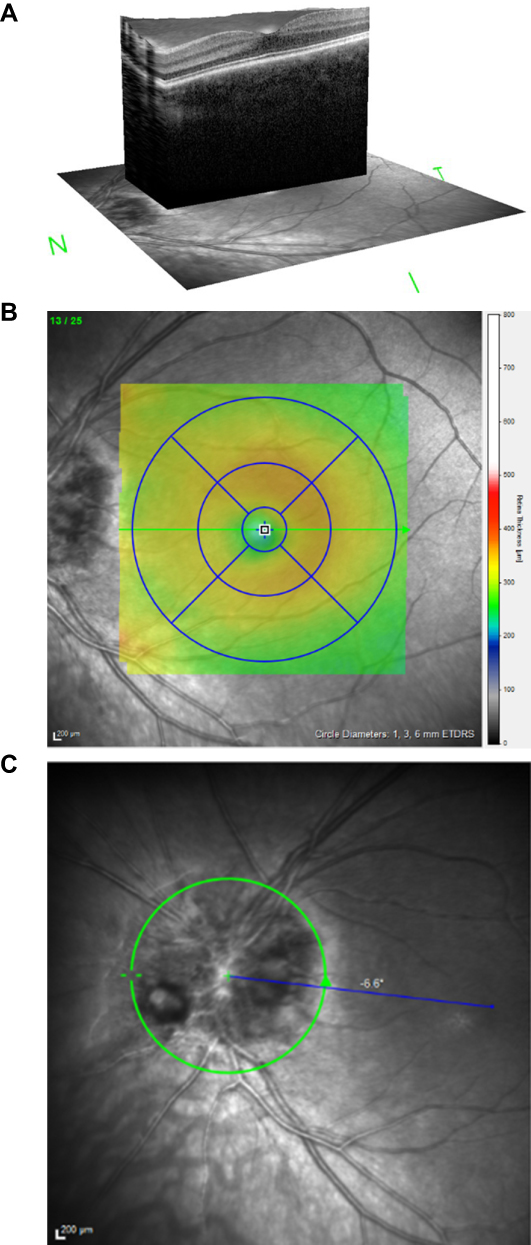 |
Figure 3 Retinal images captured by Optical Coherence Tomography (OCT) imaging (Heidelberg Engineering, Heidelberg Engineering GmbH) present a 4-year-old female patient with PFV remnants over disc three years after vitrectomy in left eye (Case 9). The final visual acuity was 0.5–0.63 on Snellen testing (with spectacle correction −7.0). (A). 3 D macular OCT image of the left macula shows normal foveal structure. (B). In the tomography central retinal thickness was normal 266 µm. (C) Papilla HRT image shows PFV stalk remnants inferonasally at 8 o’clock. |
The most favorable visual outcome, achieving 0.5 on the Snellen chart, was noted in a child diagnosed with congenital cataract and PFV, alongside subtle macular abnormalities, ie, retinal pigment epithelial mottling in the macula (Case 9, Figure 3). This child underwent combined surgical intervention at the age of 1 year, followed by secondary cataract removal at 1 year and 7 months of age.
As anticipated, children presenting with complex PFV with macular TRD exhibited poor visual outcomes following surgery. Among the PFV eyes with associated optic nerve head hypoplasia or macular TRD, the most favorable postoperative visual acuity achieved was finger counting.
Prior to and following surgery, amblyopia therapy, combined with aphakic refraction correction utilizing contact lenses on spectacle lenses, was administered to six out of eleven children, constituting 54.5% of the cohort. Despite diligent implementation of amblyopia treatment, the final visual acuity outcomes remained suboptimal, with successful amblyopia treatment observed only in one case (Case 9).
Discussion
Congenital cataract stands as a notable contributor to childhood visual impairment on a global scale, impacting an estimated 1 to 6 per 10,000 live births. The etiology of congenital cataract is multifactorial, involving genetic predispositions, maternal infections during gestation, metabolic dysregulations, and exposure to certain pharmacological agents or environmental toxins.11,12 Furthermore, congenital cataract may manifest in isolation or as a component within syndromic contexts marked by systemic aberrations. However, in comparison to simple congenital cataract, the underlying causes of unilateral congenital cataract with PFV remain relatively obscure. Notably, children presenting with congenital (infantile) cataract alongside PFV exhibit a spectrum of clinical manifestations.13
Surgical management of congenital cataract complicated by PFV is advocated prior to the onset of associated complications, such as angle-closure glaucoma, intraocular hemorrhage, and TRD. Recent findings from a meta-analysis incorporating randomized controlled trials have demonstrated that anterior vitrectomy significantly diminishes the incidence of posterior capsular opacification, secondary glaucoma, and uveitis.14 Notably, surgical outcomes exhibit variability contingent upon the anterior, posterior, or combined phenotypic presentations of PFV.15,16 Generally, posterior, or combined forms of PFV tend to mean a poorer visual prognosis compared to anterior PFV.16,17
It is noteworthy that premature infants with a history of PFV undergoing cataract surgery without IOL implantation face an elevated risk of retinal detachment.18,19 In this investigation, one eye subjected to primary lens suction due to lens coloboma and subluxation, along with stalk transection, developed TRD with subsequent subretinal fibrosis. Of note, in this small cohort, the proportion of PFV eyes undergoing primary IOL implantation was 54.5%, which surpassed the previously reported rate of 35% by Solebo et al.20
Despite advancements in surgical techniques and instrumentation, achieving optimal visual acuity remains a considerable clinical challenge in eyes with congenital cataract and PFV. Factors influencing surgical outcomes cover the age at the time of intervention, extent of ocular involvement, presence of associated ocular abnormalities such as microphthalmia, and adherence to rigorous postoperative amblyopia management protocols. In the future, long-term multicenter follow-up studies are imperative to comprehensively assess the efficacy and sustainability of surgical outcomes in the PFV cases. Continual monitoring for potential late onset complications and the implementation of appropriate interventions including vigorous amblyopia treatment and strabismus surgery are essential components of good postoperative care aimed at optimizing visual outcomes and enhancing the quality of life for affected children.
While this real-world study presents the most extensive cohort of vitrectomized pediatric eyes with congenital cataract and PFV to date in Finland, caution is warranted in extrapolating conclusions regarding optimal management due to the relatively limited number of pediatric cases. Within this study, certain eyes were monitored, and surgical intervention was deferred until occlusion of the visual axis, progression of anatomical anomalies, and/or compromise of the anterior chamber angle were observed.
Given the generally suboptimal visual outcomes observed in our surgical cohort, with one case resulting in devastating sympathetic ophthalmia, caution should be exercised in advocating surgical intervention for pediatric eyes with light perception vision, PFV, and a tent-shaped funnel configuration of TRD.8 In contrast to adults, pediatric patients often exhibit a heightened ocular immune response following cataract surgery.21 Furthermore, there is evidence suggesting that vitreoretinal surgery may serve as a precipitating factor for sympathetic ophthalmia, thus warranting careful consideration prior to ocular procedures in children with a dismal visual prognosis.22
In recent years, particularly with pars plana vitrectomy, there has been an escalating recognition of sympathetic ophthalmia as a rare yet noteworthy complication, occurring in approximately 0.038% of all cases.23 In a juvenile rabbit model undergoing lensectomy with IOL insertion, it was demonstrated that agitation of the lens, rather than a mere corneal incision, can trigger a robust postoperative immune response.21
In Finland, a comprehensive screening protocol is in place for early detection of congenital cataract and other ocular anomalies in newborns. Within 72 hours of birth, all neonates undergo a red reflex test, followed by a secondary examination conducted by a general practitioner as part of routine infant physical examination screening. Unlike some other regions, genetic testing for unilateral congenital cataract with PFV is not routinely employed for diagnostic confirmation within the Finnish healthcare system.
Conclusion
Congenital cataract with PFV devoid of anterior segment pathology tends to correlate with the most favorable postoperative visual outcomes.16,17 Conversely, eyes presenting with anterior segment pathology, such as microphthalmia, or exhibiting complex posterior segment pathologies like macular TRD, optic nerve hypoplasia, or foveal hypoplasia, are associated with a less promising visual prognosis. Most children undergoing surgical intervention achieve only modest improvements in vision. Given the potential occurrence of sympathetic ophthalmia following surgery, meticulous case selection for surgical management is paramount. Furthermore, delving deeper into the pathogenesis of PFV is imperative to enhance our understanding of this condition.
Acknowledgments
The author gratefully acknowledges Dr. Sonja Kiehelä for data acquisition and Mrs. Sanna Piiponniemi for technical help. This study was supported by Helsinki Eye Clinic grant Y1014SI004 and Eye Foundation.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Goldberg MF. Persistent fetal vasculature (PFV): an integrated interpretation of signs and symptoms associated with persistent hyperplastic primary vitreous (PHPV). LIV Edward Jackson Memorial Lecture. Am J Ophthalmol. 1997;124(5):587–626. doi:10.1016/S0002-9394(14)70899-2
2. Zahavi A, Weinberger D, Snir M, Ron Y. Management of severe persistent fetal vasculature: case series and review of the literature. Int Ophthalmol. 2019;39(3):579–587. doi:10.1007/s10792-018-0855-9
3. Pollard ZF. Persistent hyperplastic primary vitreous: diagnosis, treatment, and results. Trans Am Ophthalmol Soc. 1997;95:487–549.
4. Khurana S, Gupta PC, Vaiphei K, Singh R, Ram J. A clinicopathological study of persistent fetal vasculature. Indian J Ophthalmol. 2019;67(6):785–787. doi:10.4103/ijo.IJO_1375_18
5. Shen JH, Liu L, Wang NK, et al. FLUORESCEIN ANGIOGRAPHY FINDINGS IN UNILATERAL PERSISTENT FETAL VASCULATURE. Retina. 2020;40(3):572–580. doi:10.1097/IAE.0000000000002398
6. Shastry BS. Persistent hyperplastic primary vitreous: congenital malformation of the eye. Clin Exp Ophthalmol. 2009;37(9):884–890. doi:10.1111/j.1442-9071.2009.02150.x
7. Walsh MK, Drenser KA, Capone A, Trese MT. Early vitrectomy effective for bilateral combined anterior and posterior persistent fetal vasculature syndrome. Retina. 2010;30(4 Suppl):S2–S8. doi:10.1097/IAE.0b013e3181d34a9e
8. Dass AB, Trese MT. Surgical results of persistent hyperplastic primary vitreous. Ophthalmology. 1999;106(2):280–284. doi:10.1016/S0161-6420(99)90066-0
9. Dutta Majumder P, Mistry S, Sridharan S, et al. J. Pediatric Sympathetic Ophthalmia: 20 Years of Data From a Tertiary Eye Center in India. J Pediatr Ophthalmol Strabismus. 2020;57(3):154–158. doi:10.3928/01913913-20200219-01
10. Agarwal M, Radosavljevic A, Tyagi M, et al. Sympathetic Ophthalmia - An Overview. Ocul Immunol Inflamm. 2023;31(4):793–809. doi:10.1080/09273948.2022.2058554
11. Haargaard B, Wohlfahrt J, Fledelius HC, Rosenberg T, Melbye M. A nationwide Danish study of 1027 cases of congenital/infantile cataracts: etiological and clinical classifications. Ophthalmology. 2004;111(12):2292–2298. doi:10.1016/j.ophtha.2004.06.024
12. Li J, Chen X, Yan Y, Yao K. Molecular genetics of congenital cataracts. Exp Eye Res. 2020;191:107872. doi:10.1016/j.exer.2019.107872
13. Santorini M, Chesneau B, Koskas-Boublil P, et al. First implication of MIP in bilateral microphthalmia with persistent fetal vasculature. Am J Med Genet A. 2023;191(5):1373–1377. doi:10.1002/ajmg.a.63133
14. Cao K, Wang J, Zhang J, et al. Efficacy and safety of vitrectomy for congenital cataract surgery: a systematic review and meta-analysis based on randomized and controlled trials. Acta Ophthalmol. 2019;97(3):233–239. doi:10.1111/aos.13974
15. Hunt A, Rowe N, Lam A, Martin F. Outcomes in persistent hyperplastic primary vitreous. Br J Ophthalmol. 2005;89(7):859–863. doi:10.1136/bjo.2004.053595
16. Sisk RA, Berrocal AM, Feuer WJ, Murray TG. Visual and anatomic outcomes with or without surgery in persistent fetal vasculature. Ophthalmology. 2010;117(11):2178–83.e1–2. doi:10.1016/j.ophtha.2010.03.062
17. Cheng LS, Kuo HK, Lin SA, Kuo ML. Surgical results of persistent fetal vasculature. Chang Gung Med J. 2004;27(8):602–608.
18. Oke I, Hwang B, Heo H, Nguyen A, Lambert SR. Risk Factors for Retinal Detachment Repair After Pediatric Cataract Surgery in the United States. Ophthalmol Sci. 2022;2(4):100203. doi:10.1016/j.xops.2022.100203
19. Ozdemir Zeydanli E, Ozdek S, Acar B, et al. Surgical outcomes of posterior persistent fetal vasculature syndrome: cases with tent-shaped and closed funnel-shaped retinal detachment. Eye. 2022;37(7):1371–1376. doi:10.1038/s41433-022-02140-0
20. Solebo AL, Russell-Eggitt I, Cumberland P, Rahi JS. Congenital cataract associated with persistent fetal vasculature: findings from IoLunder2. Eye. 2016;30(9):1204–1209. doi:10.1038/eye.2016.159
21. Young JB, Keppel TR, Waas M, et al. Quantitative proteomic analysis of aqueous humor after rabbit lensectomy reveals differences in coagulation and immunomodulatory proteins. Mol Omics. 2020;16(2):126–137. doi:10.1039/C9MO00169G
22. Ripa M, Panos GD, Rejdak R, et al. Sympathetic Ophthalmia after Vitreoretinal Surgery without Antecedent History of Trauma: a Systematic Review and Meta-Analysis. J Clin Med. 2023;12(6):2316. doi:10.3390/jcm12062316
23. Tyagi M, Agarwal K, Reddy Pappuru RR, et al. Sympathetic Ophthalmia after Vitreoretinal Surgeries: incidence, Clinical Presentations and Outcomes of a Rare Disease. Semin Ophthalmol. 2019;34(3):157–162. doi:10.1080/08820538.2019.1610464
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.