")
Back to Journals » OncoTargets and Therapy » Volume 18
Survival Outcomes in Lung Cancer Patients Newly Diagnosed Through Brain Metastasis Surgery: Impact of Druggable Mutations and Radiotherapy
Authors Chuang TI , Hsu KH , Lee PH, Tseng JS , Hsu YW , Liao CH, Huang YH, Yang TY
Received 4 February 2025
Accepted for publication 19 June 2025
Published 25 June 2025 Volume 2025:18 Pages 751—761
DOI https://doi.org/10.2147/OTT.S520700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Gaetano Romano
Tzu-I Chuang,1 Kuo-Hsuan Hsu,1,2 Po-Hsin Lee,1,3– 5 Jeng-Sen Tseng,1– 3,6,7 Yu-Wei Hsu,8 Chih-Hsiang Liao,6,9– 11,* Yen-Hsiang Huang,1– 3,* Tsung-Ying Yang1,2,4,5
1Department of Chest Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 2Lung Cancer Comprehensive Care and Research Center, Taichung Veterans General Hospital, Taichung, Taiwan; 3School of Medicine, College of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan; 4Doctoral Program in Translational Medicine, National Chung Hsing University, Taichung, Taiwan; 5Rong Hsing Translational Medicine Research Center, National Chung Hsing University, Taichung, Taiwan; 6Department of Post-Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, Taiwan; 7Institute of Biomedical Sciences, National Chung Hsing University, Taichung, Taiwan; 8Department of Oncology, Taichung Veterans General Hospital, Taichung, Taiwan; 9Departments of Neurosurgery, Neurological Institute, Taichung Veterans General Hospital, Taichung, Taiwan; 10Institute of Medicine, Chung Shan Medical University, Taichung, Taiwan; 11School of Medicine, Taipei Medical University, Taipei, Taiwan
*These authors contributed equally to this work
Correspondence: Yen-Hsiang Huang, Department of Chest Medicine, Taichung Veterans General Hospital, No. 1650, Sect. 4, Taiwan Boulevard, Taichung, 407, Taiwan, Tel +886-4-2359-2525 ext. 3201, Fax +886-4-2374-1320, Email [email protected] Chih-Hsiang Liao, Departments of Neurosurgery, Neurological Institute, Taichung Veterans General Hospital, No. 1650, Sect. 4, Taiwan Boulevard, Taichung, 407, Taiwan, Tel +886-4-2359-2525 ext. 5082, Fax +886-4-2374-1218, Email [email protected]
Background: Precocious brain metastasis in lung cancer, diagnosed through surgical resection before primary lung cancer detection, represents a unique clinical scenario with limited research. This study aims to investigate the clinical characteristics, prognosis, and the impact of different treatments on survival outcomes in this distinct population.
Materials and Methods: We retrospectively analyzed clinical outcomes of lung cancer patients newly diagnosed following brain metastasis decompression surgery in our institute, over a period from July 2012 to May 2023. Patient demographics including gender, age, surgical approach, pathological findings, receipt of radiotherapy, systemic treatment modalities, and presence of druggable mutations were documented. Druggable mutations were defined as actionable genetic alterations (AGAs) detected in patients for which corresponding targeted therapeutic agents were available.
Results: Among 64 patients analyzed, 53 (82.8%) were diagnosed with adenocarcinoma; 38 (59.4%) harbored druggable mutations. There was only one patient with small cell carcinoma in this series. Types of druggable mutations were discussed in the study. The clinical stage was IVB among 38 (59.4%) patients. Forty-nine (76.6%) patients had metastatic brain lesions with number ≦3. Thirty-five (54.7%) patients received post-operative radiotherapy. The cohort’s median overall survival (OS) was 19.6 months. Patients with druggable mutations had an OS longer than patients without druggable mutation (46.0 vs 14.5 months, Log rank test p = 0.004). Among patients with druggable mutations, we found no difference in characteristics between patients with and without post-operative cranial radiotherapy. Patients receiving post-operative cranial radiotherapy did not show significantly better clinical efficacy than patients without radiotherapy (adjusted hazard ratio: 0.68, 95% confidence interval 0.16 to 2.91).
Conclusion: In patients with precocious brain metastases from lung cancer, the presence of druggable mutations and subsequent targeted therapy significantly extended survival, whereas post-operative brain radiotherapy may not confer additional survival benefits. These findings highlight the importance of molecular profiling and targeted therapy in this unique patient population.
Keywords: brain metastasis, craniotomy, lung cancer, molecular profile, post-operative radiotherapy, target therapy
Introduction
Lung cancer is one of the leading causes of mortality worldwide. About 40–50% of patients develop distant metastasis when first diagnosed with lung cancer, and their 5-year survival rate is <10%.1–3 The Surveillance, Epidemiology, and End Results (SEER) program reported incidence shows that patients with brain metastasis suffer from significant morbidity with a poor survival outcome of 2 to 14 months for various primary cancers.4
Previous studies had demonstrated that lung cancer patients harboring driver mutation had higher incidence of brain metastasis compared to those without driver mutation.5,6 For example, among Epidermal Growth Factor Receptor (EGFR)-mutant Non-small Cell Lung Cancer (NSCLC) patients, brain metastasis presented in 24.4% of patients at the time of diagnosis of advanced disease, and 52.9% of living patients suffered from brain metastasis at 5 years follow-up.5 Fortunately, numerous therapeutic agents including tyrosine kinase inhibitors (TKIs), immune checkpoint inhibitors (ICIs) and bispecific antibodies were developed, offering favorable clinical efficacies in overcoming poor prognosis for lung cancer patients with brain metastasis,7–11 particularly those with druggable mutations – defined as actionable genetic alterations (AGAs) for which corresponding targeted therapeutic agents are available in the relevant clinical context. Additionally, whole brain radiotherapy (WBRT) and stereotactic radiosurgery (SRS) play crucial roles in enhancing local control for brain metastasis patients.12,13 However, the reproducibility of these findings in the precocious brain metastases population remains unclear. Our research specifically addresses this clinical question.
Clinical guidelines for brain metastasis treatment established by American Society of Clinical Oncology (ASCO), the Society for Neuro-Oncology (SNO), and the American Society for Radiation Oncology (ASTRO), had recommended that surgery should be considered if patients with suspected brain metastasis without a primary cancer diagnosis, patients with large tumors with mass effect, or patients with symptomatic brain metastases.14 Previous clinical trial had also highlighted the clinical benefit of surgery in patient with single brain metastasis.15,16 There are some real-world studies to discuss the prognosis of patients who underwent surgical resection for brain metastasis. Hsu et al presented patients with preserved Eastern Cooperative Oncology Group Performance Status (ECOG PS), with histology of adenocarcinoma, and without liver metastasis experienced significant longer post-resection survival.17 Huang et al showed that EGFR– mutated NSCLC patients undergoing surgical resection for brain metastasis had an associated improved survival compared with those without EGFR mutation.18 Perng et al also demonstrated EGFR mutations, especially exon 19 deletion, are correlated with better survival outcomes in patients with NSCLC brain metastasis after surgical treatment.19 In contrast, our study specifically focuses on patients with precocious brain metastases – those diagnosed with brain metastases prior to the detection of primary lung cancer. According to Shibahara et al (2018), these patients typically present with more pronounced neurological symptoms, lower performance status, and poorer post-operative survival. Research addressing this specific population remains limited.
Materials and Methods
Study Design
This was a single-center, observational, retrospective study conducted, performed in line with the principles of the Declaration of Helsinki, approved by the Institutional Review Board (IRB) of our institute (IRB No. CE24418B). Informed consent was waived due to its retrospective design. Patient confidentiality was maintained through data anonymization and de-identification procedures in accordance with institutional privacy protection protocols.
Patients
We collected and analyzed data of patients who first underwent intracranial tumor resection for decompression purposes and were later diagnosed with lung cancer based on pathological evidence from metastatic brain tissue samples. The study period was between Jul. 2012 and May 2023.
Enrolled patients had fulfilled the following inclusion criteria: (a) had received surgical resection for brain tumor before lung cancer was diagnosed; (b) received brain tumor resection for the purpose of decompression; (c) diagnosis of lung cancer was confirmed by histology from the specimen of brain tumor resection; (d) received no prior local therapy including radiotherapy for brain tumor nor systemic therapy for tumor control; and (e) stage IVA or IVB disease with M1b and M1c according to the 8th edition of the American Joint Committee for Cancer (AJCC) staging system. Patients excluded had any condition as described below: (a) underwent surgical resection for brain tumor after lung cancer had been diagnosed; (b) pathology confirmed malignancy other than lung cancer; (c) received prior local therapy including radiotherapy for brain tumor and systemic therapy for tumor control; (d) lost in follow-up and the survival status was unclear; and (e) diagnosed with another active malignancy.
We obtained from medical chart records demographic and clinical data of patients including their age, gender, smoking status, ECOG PS, clinical stage, histological subtype, baseline druggable mutation status, the number of brain metastases, and receiving post-resection radiotherapy or not. All patients were followed up with chest computed tomography (CT) scans at 3-month intervals. Brain magnetic resonance imaging (MRI) was performed every 3 to 6 months at the attending physician’s discretion.
Detection of Druggable Mutation
Druggable mutations were defined as AGAs detected in patients, referring to driver mutations for which corresponding targeted therapeutic agents were available in the relevant clinical context. Among patients with druggable mutations, Epidermal Growth Factor Receptor (EGFR) mutations were identified using either the Cobas EGFR Mutation Test v2 (Roche Molecular Systems, Inc., USA) or matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). Anaplastic Lymphoma Kinase (ALK) fusions were tested using immunohistochemical (IHC) staining with the VENTANA anti-ALK (D5F3) antibody (Roche Diagnostics/Ventana Medical Systems, Inc., USA). To screen for Proto-oncogene tyrosine-protein kinase ROS1 (ROS1) fusions, we used the VENTANA ROS1 (SP384) assay (Ventana Medical Systems, Inc., USA), and positive results were confirmed by fluorescence in situ hybridization (FISH). Additionally, BRAF gene mutations were detected using MALDI-TOF MS.
Neurosurgical Procedures
All patients underwent surgery under general anesthesia. The head was stabilized using a three-point cranial fixation device (headpins), and neuronavigation was employed intraoperatively to precisely localize the tumor. The size of the craniotomy was tailored according to the dimensions of the tumor and the extent of perifocal cerebral edema, ensuring sufficient exposure of the affected region to achieve optimal decompression.
Tumor resection was conducted microscopically using either an en bloc or piecemeal technique, employing tumor forceps and ultrasonic surgical aspirators as needed. Following tumor excision, an intracranial pressure (ICP) monitoring probe was inserted into the subdural space to allow continuous postoperative ICP monitoring in the neurosurgical intensive care unit.
After tumor removal, the brain was carefully evaluated for signs of significant swelling. In cases where substantial cerebral edema precluded safe repositioning of the bone flap, a duroplasty was performed, followed by direct closure of the scalp. Conversely, if minimal or no swelling was evident, the bone flap was secured back into position.
The primary objectives of the surgery were definitive pathological diagnosis, adequate cerebral decompression, and maintenance of ICP below 20 mmHg.
Statistical Analyses
The primary endpoint of our study was overall survival (OS). OS was determined as the period from the date of the resection of brain metastasis to death. We conducted Fisher’s exact test to assess differences in patient characteristics between those with and without post-resection cranial radiotherapy. We performed subgroup analysis on patients with druggable mutations. OS in terms of survival curves was analyzed using the Kaplan-Meier method. The Log rank test was used to assess differences in survival time. To identify prognostic factors of OS, we used the Cox proportional hazards model. All statistical tests were performed using the software SPSS 23.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set with two-tailed tests at p <0.05.
Results
Patient Characteristics and Demographic Data in the Overall Population
A total of 64 patients were recruited and analyzed. The patient’s characteristics and demographic data at the baseline are summarized in Table 1. The median age of the cohort was 61 (range 22–84) years. Thirty-five patients (54.7%) were male, and 29 patients (45.3%) were female. Thirty-three patients (51.6%) were former or current smokers, and 28 patients (43.8%) had poor performance status with ECOG PS 2 to 4. Twenty-six patients (40.6%) were in stage IVA disease, and 38 patients (59.4%) were in stage IVB disease. Regarding histology of lung cancer, most patients (82.8%) were diagnosed with lung adenocarcinoma, and NSCLC accounted for 90.6%. Also, 38 patients (59.4%) had druggable mutations at baseline (including 34 with EGFR mutation; 2 with ALK fusion, 1 with ROS-1 rearrangement; and 1 with BRAF V600E mutation). All patients with known druggable mutations received target therapy. Forty-nine patients (76.6%) had ≤3 brain metastases, and the largest brain tumor for individual patients measured at a median of 3.96 cm. Furthermore, 35 patients (54.7%) received post-resection cranial radiotherapy (WBRT or SRS).
 |
Table 1 Patient Characteristics and Demographic Data |
Survival Outcomes of the Overall Population
The median OS in the overall population was 19.6 months [95% confidence interval (95% CI), 13.7 to 25.5], and the Kaplan-Meier curve is shown in Figure 1A. The median OS in patients <65 years was 28.3 months, and in patients ≥65 years was 10.1 months. The log-rank analysis of OS showed a significant difference between patients <65 years and ≥65 years (p <0.001). Regarding performance status, the median OS in patients with ECOG PS 0 to 1 was 46.0 months, and in patients with ECOG PS 2 to 4 was 12.5 months. Patients with ECOG PS 0 to 1 had better OS than those with ECOG PS 2 to 4 was a finding also shown by the Log rank test (p <0.001). Kaplan-Meier curves revealed a 46.0 months median OS in patients with druggable mutations, compared with 14.5 months in patients without druggable mutation. Patients with a druggable mutation had a longer OS than those without druggable mutation (Log rank test, p =0.004) (Figure 1B).
 |
Figure 1 Kaplan-Meier analysis of overall survival (OS) in lung cancer patients diagnosed through surgical resection of brain metastases. (A) OS curve for the entire study cohort (n=64). The median OS was 19.6 months (95% CI: 13.7–25.5 months). (B) OS stratified by druggable mutation status. Patients with druggable mutations (blue line, n=38) demonstrated significantly longer survival compared to those without druggable mutations (Orange line, n=26), with median OS of 46.0 months (95% CI: 2.3–89.7 months) versus 14.5 months (95% CI: 1.8–27.2 months), respectively (Log rank test, p=0.004). Vertical tick marks represent censored observations. Abbreviations: Cum Survival, cumulative survival probability; CI, confidence interval. |
Univariate and Multivariate Analyses of OS in the Overall Population
The Cox proportional hazard model was used to identify clinical factors impacting OS (Table 2). The univariate analysis showed a longer OS in patients aged <65 years [Hazard Ratio (HR) 0.30 (95% CI 0.15 to 0.60), p <0.001] and in patients with ECOG PS 0 to 1 [HR 0.28 (95% CI 0.14 to 0.56), p <0.001]. Male patients had a shorter OS with a HR of 3.51 (95% CI 1.65 to 7.49, p =0.001); patients without druggable mutations with a HR of 2.60 (95% CI 1.34 to 5.08, p =0.005). The multivariable analysis showed better prognosis in patients aged <65 years with an adjusted HR of 0.24 (95% CI 0.10 to 0.58, p =0.002) and in patients with ECOG PS 0 to 1 with an adjusted HR of 0.38 (95% CI 0.18 to 0.81, p =0.012), when compared with patients ≧65 years and ECOG PS 2 to 4, respectively. No druggable mutation was a poor prognostic factor with an adjusted HR 7.90 (95% CI 1.85 to 33.70, p =0.005).
 |
Table 2 Univariate and Multivariate Analyses on Overall Survival in the Overall Population |
Survival Outcomes in Patients with or without Post-Resection Radiotherapy for Brain Metastasis
The median OS was not reached for patients without post-resection radiotherapy (ie, less than 50% of the patients in this group died at the time of analysis), while the median OS was 18.7 months for patients who received radiotherapies. The univariate analysis showed a trend that patients without post-resection radiotherapy experienced longer OS than patients with post-resection radiotherapy [HR 0.48 (95% CI 0.23 to 1.01, p =0.052)], which was not confirmed by multivariate analysis, with an adjusted HR of 0.90 (95% CI 0.37 to 2.20, p =0.816). In addition, there were no differences in age, gender, smoking status, ECOG PS, stage, and the number of brain metastases between patients with and without post-resection radiotherapy. However, more patients had a druggable mutation in the group without post-resection radiotherapy than in the group with post-resection radiotherapy (p =0.021). Results are shown in Supplementary Table 1.
Survival Outcomes in Patients with Druggable Mutations
In the subgroup analysis of patients with druggable mutations, the median OS was 50.3 months in patients with ≦3 brain metastatic lesions, and 46.0 months in patients with >3 brain metastatic lesions (Figure 2A). Again, the median OS was not reached in patients without post-resection cranial radiotherapy, and it was 20.7 months in patients with post-resection radiotherapy (Figure 2B). The Cox proportional hazards model showed no influence on the prognosis of OS from age, gender, smoking status, stage, numbers of brain metastasis and post-resection radiotherapy. The multivariate analysis confirmed that patients with ECOG PS 0 to 1 experienced longer OS than those with ECOG 2 to 4, with an adjusted HR of 0.13 (95% CI 0.03 to 0.63, p =0.011). (Table 3) Table 4 shows patient characteristics of those with and without post-operative cranial radiotherapy in the group with druggable mutations. We found no difference in their age, gender, smoking status, ECOG PS, stage, and number of brain metastases.
 |
Table 3 Univariate and Multivariate Analyses on Overall Survival in Patients of Table 3 with Druggable Mutations |
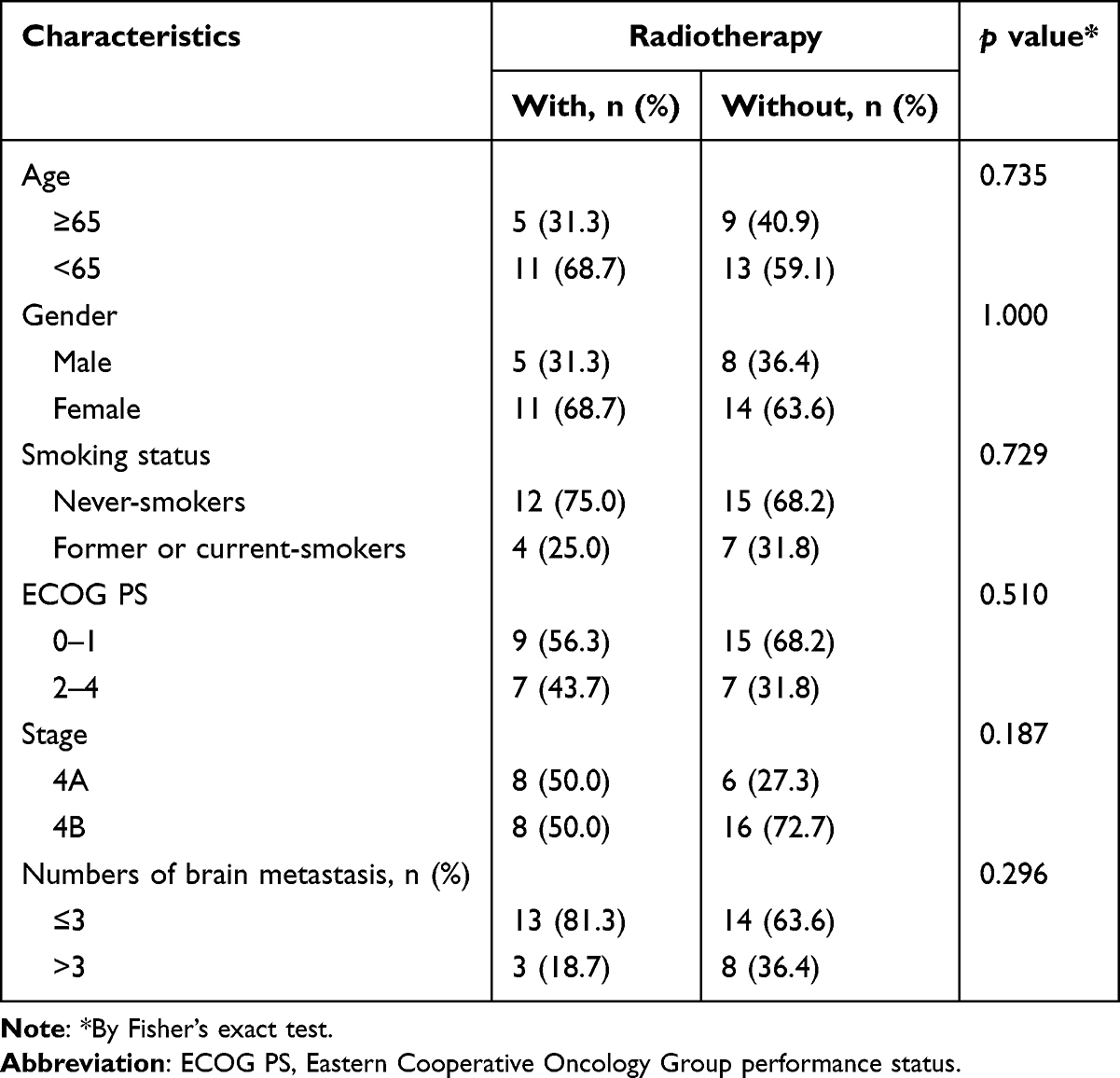 |
Table 4 Patient Characteristics Compared Between Those with and without Radiotherapy in Patients with Druggable Mutations (n=38) |
 |
Figure 2 Kaplan-Meier analysis of overall survival (OS) in lung cancer patients with druggable mutations stratified by clinical characteristics. (A) Comparison of OS based on the number of brain metastatic lesions. Patients with ≤3 brain metastatic lesions (blue line) showed a median OS of 50.2 months, compared to 46.0 months in patients with >3 brain metastatic lesions (Orange line). The difference was not statistically significant (Log rank test, p=0.723). (B) Impact of post-operative radiotherapy on OS. The median OS did not reach in patients who did not receive brain radiotherapy (blue line, “No brain RT”), whereas those who received brain radiotherapy (orange line, “Brain RT”) had a median OS of 11.4 months (95% CI: 0.0–43.0 months). This difference did not reach statistical significance (Log rank test, p=0.265). Abbreviations: RT, radiotherapy; Cum Survival, cumulative survival probability. |
Discussion
About 44% of lung cancer patients develop brain metastases either very early in their disease course (precocious) or simultaneously with their primary lung cancer diagnosis (synchronous).20 These patients experienced a higher chance of having mass effects and neurological symptoms from their brain metastases, and most of them have a poor prognosis. Our study identified three favorable prognostic factors for lung cancer patients newly diagnosed via brain metastasis decompression surgery: age <65 years, ECOG PS 0–1, and presence of druggable mutations. In the subgroup analysis among patients with druggable mutations, post-operative cranial radiotherapy did not demonstrate a statistically significant improvement in overall survival.
Retrospective studies have reported varied outcomes for NSCLC patients undergoing surgical resection of brain metastases. Huang et al showed a 24-month median post-resection survival in a cohort with 59.6% synchronous and 40.4% metachronous brain metastases.18 In contrast, Shah et al reported a short 9.7-month median post-resection survival in a group comprising 35% synchronous and 65% metachronous brain metastasis.21 Perng et al found a middle ground, with a 17-month median post-operative survival in a cohort split nearly evenly between synchronous (47%) and metachronous (53%) brain metastases.19 In our study, we uniquely focused on patients whose lung cancer was initially diagnosed through pathological examination of their brain metastases, all of which were precocious and synchronous. In this specific group, we found a median OS of 19.6 months. These inconsistencies of post-resection outcomes across studies might be attributed to differences in initial disease stage, patient performance status, timing of brain metastasis, and prevalence of known druggable mutations.
Nowadays, the treatment for advanced NSCLC patients is individualized and based on findings of their molecular biology. A previous study reported longer OS in patients with lung adenocarcinoma and a druggable driver mutation after receiving matched targeted therapy.22 In NSCLC patients undergoing surgical resection of brain metastases, Shah et al found similar OS between patients with EGFR mutation and patients with EGFR wild-type [HR 0.89 (95% CI 0.45 to 1.76), p =0.74]. However, the subgroup of patients with EGFR mutation taking EGFR-TKIs experienced a significantly longer OS than those without driver mutation and without EGFR-TKIs treatment [adjusted HR 0.42 (95% CI 0.18 to 0.99), p =0.047)].21 Furthermore, Perng et al found that the EGFR mutation is associated with longer survival with an adjusted HR 0.41 (95% CI 0.20 to 0.85) in patients with NSCLC brain metastases suitable for surgical treatment, especially in patients having exon 19 deletion subtype.19 Hsu et al reported a 34.4-month median post-resection survival in patients with driver mutation.17 In our study, 38 patients (59.4%) had a druggable mutation, and all of them had received matched target therapies. The median OS was 46.0 months in patients with a druggable mutation and 14.5 months in patients without such mutations. From multivariate analysis, we found that patients without druggable mutations had a significantly shorter OS, with an adjusted HR 7.90 (95% CI 1.85 to 33.70, p =0.005). (Table 2) Our findings also highlight the importance of molecular tests in lung cancer patients who were initially diagnosed via brain metastasis surgery.
For patients receiving complete surgical resection of brain oligo-metastases, previous clinical trials showed that cranial radiotherapy, including WBRT and SRS, significantly reduces intracranial local recurrence.22,23 Some retrospective studies suggest that cranial radiotherapy may extend survival in post-craniotomy patients. However, the actual survival benefits of radiotherapy are still unclear.24,25 In our study, for patients with druggable mutation, post-craniotomy radiotherapy did not significantly prolong OS, with an adjusted HR 0.54 (95% CI 0.18 to 1.63, p =0.274). (Table 3) Furthermore, among patients with druggable mutations, we found no significant differences in characteristics (including the number of brain metastases) between those who received post-resection cranial radiotherapy and those who did not. The prolonged OS in our patients was likely related to the revolution of small molecular medication, so-called target therapy. Preclinical studies demonstrated the blood–brain barrier penetration ability of target therapies,26,27 and the clinical efficacies of target therapies were confirmed by clinical trials.7,8 In EGFR-mutant carrying NSCLC patients with brain metastasis, combined therapy of SRS or surgery and EGFR-TKIs could provide extra-survival benefits.28,29 All patients enrolled in our study were symptomatic due to mass effect/brain swelling and underwent brain tumor resection for decompression. Specifically, all these patients underwent neurosurgery for local control before receiving their lung cancer diagnosis. Therefore, the clinical benefits of post-craniotomy radiotherapy might have been attenuated. In current clinical guidelines, focal therapy for symptomatic brain metastasis, including radiosurgery, radiotherapy, and surgery, is recommended; focal therapy for asymptomatic brain metastasis could be deferred if a high potency target therapy is taken.14 In brief, the role of post-craniotomy radiotherapy for this subgroup is inconclusive. Our results indicated that post-craniotomy radiotherapy could be deferred in druggable brain metastasis-diagnosed lung cancer patients. This is the first study to examine the prognosis of lung cancer patients who were newly diagnosed through pathological examination of brain metastases at initial encounter, and more prospective clinical trials are needed to complement the current treatment guidelines.
As a single-center retrospective study, it may have selection bias, particularly regarding patient race and location. The small sample size limits the study’s statistical power and ability to detect some significant clinical factors. Some clinical data containing detailed neurological symptoms and patient-reported questionnaires might not be available. The decision to use cranial radiotherapy was made by the team of our neuro-radiation oncologists, which could introduce treatment selection bias. Finally, our study specifically enrolled patients who underwent surgical decompression as an inclusion criterion, which limits our ability to include a non-surgical cohort as comparison. Despite these limitations, our findings offer valuable insights into this unique patient group. We recommend larger, multi-center prospective trials, which could address our study’s limitations and better explain how different factors affect patient outcomes.
Conclusion
Our study shed light on the favorable survival outcomes in patients with druggable mutations who were diagnosed through surgical resection of brain metastatic lesions for decompression. Additional factors associated with favorable survival outcomes included age < 65 years and ECOG PS 0–1. Notably, post-operative radiotherapy may not significantly prolong OS among patients with druggable mutations. Further prospective clinical trials should be conducted to confirm our findings.
Data Sharing Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
Approval was obtained from the Institutional Review Board (IRB) of Taichung Veterans General Hospital (TCVGH) in Taiwan (IRB No. CE24418B). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was partially supported by grants from Taichung Veterans General Hospital (TCVGH‐1123201B) and Taichung Veterans General Hospital/ National Chung Hsing University Joint Research Program (TCVGH-NCHU1137612).
Disclosure
The authors have no conflicts of interest to disclose for this work.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
2. Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr Oncol Rep. 2012;14(1):48–54. doi:10.1007/s11912-011-0203-y
3. Riihimäki M, Hemminki A, Fallah M, et al. Metastatic sites and survival in lung cancer. Lung Cancer. 2014;86(1):78–84. doi:10.1016/j.lungcan.2014.07.020
4. Cagney DN, Martin AM, Catalano PJ, et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: a population-based study. Neuro Oncol. 2017;19(11):1511–1521. doi:10.1093/neuonc/nox077
5. Rangachari D, Yamaguchi N, VanderLaan PA, et al. Brain metastases in patients with EGFR-mutated or ALK-rearranged non-small-cell lung cancers. Lung Cancer. 2015;88(1):108–111. doi:10.1016/j.lungcan.2015.01.020
6. Wang H, Wang Z, Zhang G, et al. Driver genes as predictive indicators of brain metastasis in patients with advanced NSCLC: EGFR, ALK, and RET gene mutations. Cancer Med. 2020;9(2):487–495. doi:10.1002/cam4.2706
7. Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
8. Solomon BJ, Liu G, Felip E, et al. Lorlatinib versus crizotinib in patients with advanced ALK -positive non–small cell lung cancer: 5-year outcomes from the Phase III CROWN study. J Clin Oncol. 2024;42:3400–3409. doi:10.1200/JCO.24.00581
9. Wakuda K, Yabe M, Kodama H, et al. Efficacy of pembrolizumab in patients with brain metastasis caused by previously untreated non-small cell lung cancer with high tumor PD-L1 expression. Lung Cancer. 2021;151:60–68. doi:10.1016/j.lungcan.2020.11.009
10. Cho BC, Lu S, Felip E, et al. Amivantamab plus lazertinib in previously untreated EGFR -mutated advanced NSCLC. N Engl J Med. 2024;391:1486–1498. doi:10.1056/NEJMoa2403614
11. Subbiah V, Gainor JF, Oxnard GR, et al. Intracranial efficacy of selpercatinib in RET fusion-positive non-small cell lung cancers on the LIBRETTO-001 trial. Clin Cancer Res. 2021;27(15):4160–4167. doi:10.1158/1078-0432.CCR-21-0800
12. Brown PD, Jaeckle K, Ballman KV, et al. Effect of radiosurgery alone vs radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases: a randomized clinical trial. JAMA. 2016;316(4):401–409. doi:10.1001/jama.2016.9839
13. Yamamoto M, Serizawa T, Shuto T, et al. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): a multi-institutional prospective observational study. Lancet Oncol. 2014;15(4):387–395. doi:10.1016/S1470-2045(14)70061-0
14. Vogelbaum MA, Brown PD, Messersmith H, et al. Treatment for brain metastases: ASCO-SNO-ASTRO guideline. J Clin Oncol. 2022;40(5):492–516. doi:10.1200/JCO.21.02314
15. Mintz AH, Kestle J, Rathbone MP, et al. A randomized trial to assess the efficacy of surgery in addition to radiotherapy in patients with a single cerebral metastasis. Cancer. 1996;78(7):1470–1476. doi:10.1002/(SICI)1097-0142(19961001)78:7<1470::AID-CNCR14>3.0.CO;2-X
16. Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med. 1990;322(8):494–500. doi:10.1056/NEJM199002223220802
17. Hsu PC, Chiu LC, Chen KT, et al. Clinical outcome analysis of non-small cell lung cancer patients with brain metastasis receiving metastatic brain tumor resection surgery: a multicenter observational study. Am J Cancer Res. 2023;13(8):3607–3617.
18. Huang Y, Chow KKH, Aredo JV, et al. Epidermal growth factor receptor mutation status confers survival benefit in patients with non-small-cell lung cancer undergoing surgical resection of brain metastases: a retrospective cohort study. World Neurosurg. 2019;125:e487–e496. doi:10.1016/j.wneu.2019.01.112
19. Perng PS, Hsu HP, Lee PH, Huang CC, Lin CC, Lee JS. Correlation of EGFR mutation subtypes and survival in surgically treated brain metastasis from non-small-cell lung cancer. Asian J Surg. 2023;46(1):269–276. doi:10.1016/j.asjsur.2022.03.076
20. Shibahara I, Kanamori M, Watanabe T, et al. Clinical features of precocious, synchronous, and metachronous brain metastases and the role of tumor resection. World Neurosurg. 2018;113:e1–e9. doi:10.1016/j.wneu.2017.10.145
21. Shah PP, Franke JL, Medikonda R, et al. Mutation status and postresection survival of patients with non-small cell lung cancer brain metastasis: implications of biomarker-driven therapy. J Neurosurg. 2021;136(1):56–66. doi:10.3171/2020.10.JNS201787
22. Kris MG, Johnson BE, Berry LD, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014;311(19):1998–2006. doi:10.1001/jama.2014.3741
23. Kocher M, Soffietti R, Abacioglu U, et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952-26001 study. J Clin Oncol. 2011;29(2):134–141. doi:10.1200/JCO.2010.30.1655
24. Sivasanker M, Madhugiri VS, Moiyadi AV, Shetty P, Subi TS. Surgery for brain metastases: an analysis of outcomes and factors affecting survival. Clin Neurol Neurosurg. 2018;168:153–162. doi:10.1016/j.clineuro.2018.03.011
25. Xu M, Song K, Zhou Z, Yu Z, Lv Y, Xu H. Survival and prognostic factors in patients undergoing the resection of solitary brain metastasis from non-small cell lung cancer: a retrospective cohort study. J Thorac Dis. 2022;14(10):4113–4124. doi:10.21037/jtd-22-1279
26. Colclough N, Chen K, Johnström P, et al. Preclinical comparison of the blood-brain barrier permeability of osimertinib with other EGFR TKIs. Clin Cancer Res. 2021;27(1):189–201. doi:10.1158/1078-0432.CCR-19-1871
27. Collier TL, Normandin MD, Stephenson NA, et al. Synthesis and preliminary PET imaging of 11C and 18F isotopologues of the ROS1/ALK inhibitor lorlatinib. Nat Commun. 2017;8:15761. doi:10.1038/ncomms15761
28. Zhao Y, Li S, Yang X, et al. Overall survival benefit of osimertinib and clinical value of upfront cranial local therapy in untreated EGFR-mutant nonsmall cell lung cancer with brain metastasis. Int J Cancer. 2022;150(8):1318–1328. doi:10.1002/ijc.33904
29. Magnuson WJ, Lester-Coll NH, Wu AJ, et al. Management of brain metastases in tyrosine kinase inhibitor-naïve epidermal growth factor receptor-mutant non-small-cell lung cancer: a retrospective multi-institutional analysis. J Clin Oncol. 2017;35(10):1070–1077. doi:10.1200/JCO.2016.69.7144
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.