")
Back to Journals » Journal of Inflammation Research » Volume 17
Systemic Inflammation Predict Neurological Functional Outcome in Patients with Tuberculous Meningitis: A Multicenter Retrospective Cohort Study in China
Authors Guo Y , Zhang R, Gan X, Wang E, Lu S, Jiang H, Duan H, Yuan Z, Li W, Liu Y
Received 31 July 2024
Accepted for publication 15 October 2024
Published 22 October 2024 Volume 2024:17 Pages 7561—7571
DOI https://doi.org/10.2147/JIR.S489495
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yijia Guo,1– 3,* Ruyun Zhang,4,* Xinling Gan,5 Erli Wang,6 Shuihua Lu,7 Hui Jiang,3 Hongfei Duan,8 Zhengzhou Yuan,9 Weimin Li,2,3,10 Yong Liu1
1Department of Neurology, Chengdu Medical College, The First Affiliated Hospital, Chengdu, People’s Republic of China; 2Beijing Municipal Key Laboratory of Clinical Epidemiology, School of Public Health, Capital Medical University, Beijing, People’s Republic of China; 3Beijing Chest Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Department of Emergency, Beijing Chest Hospital, Capital Medical University, Beijing, People’s Republic of China; 5Key Laboratory of Rehabilitation Medicine in Sichuan Province, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 6Department of Radiology, The First People’s Hospital of Longquanyi District, Chengdu, People’s Republic of China; 7National Clinical Research Center for Infectious Diseases, Guangdong Provincial Clinical Research Center for Tuberculosis, Shenzhen Third People’s Hospital, Southern University of Science and Technology, Shenzhen, People’s Republic of China; 8Department of Tuberculosis, Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis and Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 9Department of Neurology, The Affiliated Hospital of Southwest Medical University, Luzhou, People’s Republic of China; 10National Tuberculosis Clinical Laboratory of China, Beijing Key Laboratory in Drug Resistance Tuberculosis Research, Beijing Tuberculosis and Thoracic Tumor Research Institute, Beijing, People’s Republic of China
*These authors contributed equally to this work as first authors
Correspondence: Yong Liu, Chengdu Medical College, The First Affiliated Hospital, No. 278, Middle Section, Baoguang Avenue, Xindu District, Chengdu, 610500, People’s Republic of China, Email [email protected]
Background: The predictors associated with clinical outcomes in patients with tuberculous meningitis (TBM) remain unclear. We aimed to analyse the relationship between systemic inflammation and clinical outcomes, as well as to explore whether systemic inflammation level influences the effectiveness of dexamethasone on treatment.
Methods: Between January 2011 and December 2021, TBM patients admitted to five hospitals were observed consecutively. Baseline and post-treatment systemic inflammation levels were calculated using the neutrophil-lymphocyte-ratio (NLR). Generalized linear mixed models were employed to identify predictors of clinical outcomes. Propensity score matching and subgroup analyses were conducted to evaluate the effect of dexamethasone on treatment outcomes across different NLR levels.
Results: A total of 1203 TBM patients were included in the study. During the follow-up, 144 (13.6%) participants experienced early neurological deterioration within 7 days after admission, and 345 (28.67%) exhibited poor functional outcome at the 12-month follow-up. Multivariate analysis revealed that post-treatment NLR was significantly associated with early neurological deterioration (OR=1.25; 95% CI, 1.14– 1.33; P< 0.001), and poor outcome (OR=1.34; 95% CI, 1.26– 1.45; P< 0.001). After propensity score matching, dexamethasone treatment was not associated with early neurological deterioration (OR=0.83; 95% CI, 0.42– 1.66; P=0.610) or poor outcome (OR=1.22; 95% CI, 0.49– 2.11; P=0.490) in the highest quartile of post-treatment NLR. The effect of dexamethasone on treatment outcomes did not significantly vary with disease severity stratification.
Conclusion: Elevated systemic inflammation is an independent risk factor for neurological outcome in TBM patients. Further studies are required to investigate systemic inflammation in more severely affected population to better predict the outcomes following anti-inflammatory therapies.
Keywords: tuberculous meningitis, systemic inflammation, neurological outcome
Introduction
Tuberculosis (TB) is a major global health issue, affecting approximately 10 million individuals annually and serving as the leading cause of death from a single infectious disease.1 Tuberculous meningitis (TBM) is acknowledged as the most severe form of TB infection,2,3 accounting for nearly 40% of TB-related mortality4 and substantially increasing the likelihood of neurological disability.5 Therefore, it is of great importance to identify individuals at high risk of neurological disability in TBM patients, as they may require more intensive therapeutic interventions to improve clinical outcomes.
Recent studies have challenged the traditional view of the brain as an immune-privileged organ due to the presence of the blood-brain barrier.6–8 These studies demonstrate that peripheral immune cells can penetrate the blood-brain barrier during neurological disorders.9,10 Previous research has suggested that dead neuronal cells release inflammatory mediators within brain tissue,11 triggering the infiltration of peripheral immune cells into local tissue and leading to neurological deterioration.12 To mitigate the overactive immune response, national guidelines recommend early glucocorticoid (GC) treatment in patients with TBM.13,14 GCs have been shown to be effective anti-inflammatory agents, significantly reducing TBM-related mortality rates.15 However, concerns have been raised regarding the clinical efficacy of GCs in TBM patients co-infected with HIV. A recent clinical trial indicated that dexamethasone did not provide substantial benefits in terms of survival or functional improvement for individuals with HIV.16 It is speculated that the effectiveness of GCs may vary among specific subgroups of TBM patients; however, identifying those who may benefit from GC treatment remains unclear.16 A retrospective cohort study of COVID-19 patients revealed a significant association between elevated levels of systemic inflammation on admission and an increased risk of mortality, with GC therapy demonstrating a reduction in mortality specifically among high-risk individuals identified by systemic inflammation level.17 Furthermore, another study focused on patients with acute respiratory distress syndrome also found a positive correlation between elevated systemic inflammation and a favorable response to GC treatment.18 This finding suggests that systemic inflammation levels may serve as a novel marker for predicting treatment outcomes.18 Nevertheless, no prior studies have investigated whether systemic inflammation can predict clinical outcomes and the efficacy of GC therapy in TBM patients.
In this multi-center, retrospective cohort study of TBM from China, we hypothesized that elevated levels of systemic inflammation are associated with early neurological deterioration and subsequent disability, and may also influence the outcomes of GC treatment.
Materials and Methods
Study Population
We conducted a retrospective cohort study across five hospitals in China from January 2011 to December 2021. We investigated patients who received a laboratory-confirmed or clinical diagnosis of TBM according to established guidelines.19 The diagnostic criteria for TBM were categorized into definite, probable, and possible TBM.
Definite TBM was confirmed by the presence of acid-fast bacilli in cerebrospinal fluid (CSF), a positive culture for mycobacterium, or detection of mycobacterial nucleic acids via polymerase chain reaction in CSF. Probable TBM was defined as patients who fulfilled clinical criteria with a total diagnostic score of 10 or more points (when brain imaging was not available) or 12 or more points (when brain imaging was available). For possible TBM, patients needed to meet clinical criteria with a total diagnostic score ranging from 6 to 9 points without brain imaging or 6 to 11 points with brain imaging.19 This study was approved by the ethics committee at Beijing Chest Hospital (Approval number: YJS-2022-07). Informed consent was waived due to the retrospective nature of the study, all patient data was anonymized or maintained with confidentiality. The study protocol was reported in accordance with the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) guideline.20
Data Collection
Demographic information, clinical manifestations, vital signs (temperature, heart rate, and respiratory rate), laboratory results, radiological findings, and treatment were collected. The clinical severity at admission was staged according to the British Medical Research Council (BMRC) grade.21 The BMRC grade criteria included two main dimensions: impaired consciousness status and neurological deficits. A clinical stage between grade I and III was assigned for diagnosis. To assess neurological deficit, we utilized the Expanded Disability Severity Score (EDSS) at baseline and 7 days after therapy. The EDSS score, ranging from 0 (no disability) to 10 (death),22,23 was used to identify early neurological deterioration, defined as an increased score≥1. Baseline peripheral blood cell parameters, including white blood cell count, neutrophils, monocytes, lymphocytes, and platelets, were collected within 24 hours after admission before treatment initiation. Follow-up parameters were obtained at 3 days post-treatment. Additionally, cerebrospinal fluid (CSF) findings, such as white blood cell count, mononuclear cells, multinuclear cells, glucose and chloride concentration, and protein levels, were collected based on the first examination after admission.
Definition of Systemic Inflammation and Follow-Up Outcome
Systemic inflammation was assessed using the neutrophil-to-lymphocyte ratio (NLR), with NLRbaseline and NLRafter representing the baseline and post-treatment systemic inflammation, respectively. The NLRchange was computed by subtracting NLRbaseline from NLRafter, while the NLRratio was determined by dividing NLRafter by NLRbaseline. The baseline NLR values were classified into four categories: Q1 (NLR≤2.8), Q2 (2.8< NLR≤4.5), Q3 (4.5<NLR≤8.0), and Q4 (NLR>8.0).
We also evaluated the criteria of the systemic inflammatory response syndrome (SIRS) within 24 hours after admission to define systemic inflammation. SIRS were diagnosed if at least two of the following criteria were met: temperature over 38°C, respiratory rate over 20 cycles per minute, heart rate over 90 bpm, and leukocytosis/leukopenia/bandemia (leukocytes >12×109/L, <4×109/L, or bandemia ≥10%).24
Following discharge, patients underwent follow-up assessments at 3, 6, and 12 months at local centers to evaluate their clinical status. The outcome measure was determined using the modified Rankin Scale (mRS), with a poor functional outcome (mRS score of 3–6 at 12 months) serving as the primary endpoint. Information on mRS scores was collected through telephone interviews or face-to-face follow-up sessions with patients or their family members.
Statistical Analyses
The sample size was calculated based on the number of outcome events. We estimated that 10–15 potential variables are significantly associated with poor outcome in TBM. The minimum sample size required approximately 100–150 events of poor outcome to avoid violating the principle of approximately ten outcome events per variable in generalized linear mixed models.25 Descriptive characteristics were reported as percentages for categorical variables or mean with standard deviation for continuous variables. Chi-square or Fisher exact test, Student t-test, or the Mann–Whitney U-test were performed for statistical analysis when appropriate. To account for the expected correlation in outcomes within different centers, a two-level generalized linear mixed model was fitted using a logit link. This model was utilized to analyze potential predictors associated with clinical outcomes, with patients at the first level and hospitals at the second level. Additionally, the net reclassification index (NRI) and integrated discrimination index (IDI) were employed to quantify the improvement in correct reclassification and sensitivity by adding different NLR parameters to outcome models.
To mitigate the influence of confounding factors, propensity score matching (PSM) was conducted. Subgroup analysis was performed to identify factors associated with dexamethasone treatment. All tests were two-tailed, with a significance level set at P<0.05. All analyses were conducted using R version 4.2.0.
Results
Baseline Characteristics
A total of 1203 patients were included in the analysis, as depicted in the study flowchart (Figure S1). The baseline characteristics of the participants are detailed in Table 1, revealing that 636 (52.8%) were male, with a mean age of 38.6 (18.2) years. Based on the diagnostic criteria, 1024 (85.1%) patients had a clinical diagnosis of TBM, while 179 (14.9%) were laboratory-confirmed TBM. At admission, 603 (50.1%) patients were classified as BMRC grade I, 444 (36.9%) as grade II, and 156 (12.9%) as grade III.
 |
Table 1 Baseline Characteristics of Study Participants |
Analysis of the Association Between NLR and Early Neurological Deterioration
Following a 7-day follow-up after admission, a total of 144 (13.6%) participants experienced early neurological deterioration. Univariate analysis indicated that several factors such as age, diabetes, BMRC Grade, other coexisting infections, SIRS, meningeal enhancement, hydrocephalus and NLR, were associated with an increased risk of early neurological deterioration (Table S1). To analyze the association between NLR and early neurological deterioration, we employed various adjusted models (Table 2). After adjusting for demographic, clinical and treatment variables, NLRafter (OR=1.25; 95% CI, 1.14–1.33; P<0.001), NLRchange (OR=1.08; 95% CI, 1.03–1.12; P<0.001) and NLRratio (OR=1.32; 95% CI, 1.16–1.41; P<0.001) emerged as independent risk factors for early neurological deterioration.
 |
Table 2 Association of Baseline, Follow-Up and Dynamic Change of NLR with Clinical Outcomes |
Analysis of the Association Between NLR and Poor Functional Outcome
With a follow-up of 12 months, 345 (28.7%) participants exhibited poor functional outcome. Univariate analysis showed that several factors were associated with an elevated risk of poor functional outcomes, including age, diabetes, drug-resistant tuberculosis, BMRC grade, other coexisting infections, SIRS, cerebral infarction, hydrocephalus, and NLR (Table S2). To further investigate the relationship between NLR levels and poor functional outcome, we utilized various adjusted models (Table 2). After adjusting for confounding factors, NLRbaseline (OR=1.16; 95% CI, 1.08–1.20; P<0.001), NLRafter (OR=1.34; 95% CI, 1.26–1.45; P<0.001), NLRchange (OR=1.09; 95% CI, 1.03–1.11; P<0.001) and NLRratio (OR=1.16; 95% CI, 1.05–1.27; P=0.006) were identified as independent risk factors significantly predicting poor functional outcome. Sensitive analysis was performed in patients with different BMRC grades and those who received dexamethasone treatment (Table S3).
Discrimination and Calibration Analysis of NLR to Predictive Models
The inclusion of NLRafter to the basic model significantly improved the accuracy in predicting early neurological deterioration and poor functional outcome compared to other parameters. Specifically, the addition of the NLRafter did resulted a significant increase in NRI (12.26%, P=0.003) and IDI (3.52%, P<0.001) for early neurological deterioration, as well as NRI (14.83%, P<0.001) and IDI (7.99%, P<0.001) for poor functional outcome, respectively. Detailed results of NRI and IDI can be found in Table 3.
 |
Table 3 Performance of Predictive Models with NLR for Clinical Outcomes |
Propensity Score Matching to Explore Whether NLR Stratification Influences the Treatment Effect of Dexamethasone
After employing PSM to mitigate the impact of confounding factors, the patient groups were found to be well-balanced (Table S4). The findings indicate that dexamethasone treatment did not demonstrate an advantage in reducing the risk of early neurological deterioration (OR=0.83; 95% CI, 0.42–1.66; P=0.610; Figure 1) and poor functional outcome (OR=1.22; 95% CI, 0.49–2.11; P=0.490; Figure 2) in the highest NLRafter quartile. The treatment effect of dexamethasone on clinical outcomes did not differ across varying disease severity (Tables 4 and S5–S7) and other subgroups (Figures S2 and S3).
 |
Table 4 Effect of Dexamethasone on Clinical Outcomes in Post-Treatment NLR Category According to Severity Stratification |
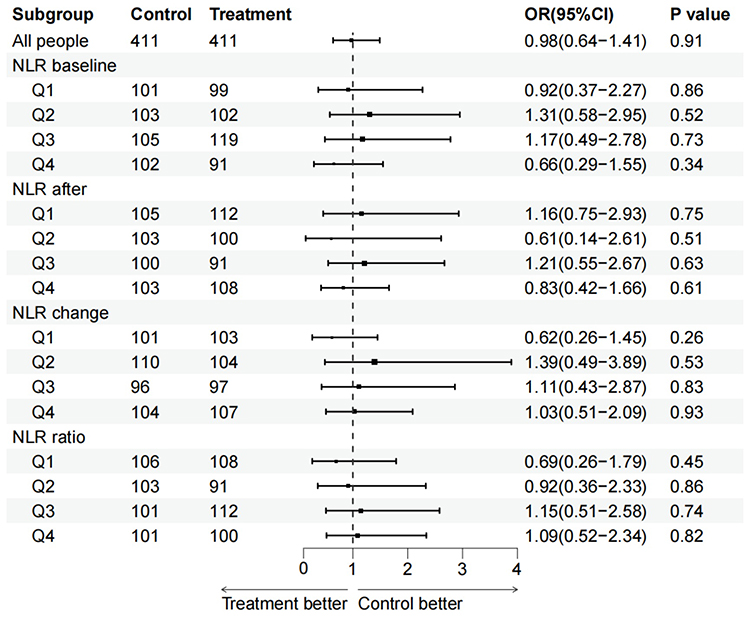 |
Figure 1 Forestplot for NLR subgroup difference in dexamethasone treatment for early neurological deterioration. NLR baseline: Q1 (NLR≤2.8), Q2 (2.8< NLR≤4.5), Q3 (4.5<NLR≤8.0), and Q4 (NLR>8.0); NLR after: Q1 (NLR≤3.4), Q2 (3.4< NLR≤6.4), Q3 (6.4<NLR≤8.4), and Q4 (NLR>8.4); NLR change: Q1 (change≤-1.9), Q2 (−1.9< change≤0.8), Q3 (0.8<change≤3.6), and Q4 (change>3.6); NLR ratio: Q1 (ratio≤0.7), Q2 (0.7< ratio≤1.2), Q3 (1.2<ratio≤2.2), and Q4 (ratio>2.2). Abbreviation: NLR, neutrophil-lymphocyte-ratio. |
 |
Figure 2 Forestplot for NLR subgroup difference in dexamethasone treatment for poor functional outcome. NLR baseline: Q1 (NLR≤2.8), Q2 (2.8< NLR≤4.5), Q3 (4.5<NLR≤8.0), and Q4 (NLR>8.0); NLR after: Q1 (NLR≤3.4), Q2 (3.4< NLR≤6.4), Q3 (6.4<NLR≤8.4), and Q4 (NLR>8.4); NLR change: Q1 (change≤-1.9), Q2 (−1.9< change≤0.8), Q3 (0.8<change≤3.6), and Q4 (change>3.6); NLR ratio: Q1 (ratio≤0.7), Q2 (0.7< ratio≤1.2), Q3 (1.2<ratio≤2.2), and Q4 (ratio>2.2). Abbreviation: NLR, neutrophil-lymphocyte-ratio. |
Discussion
The present multi-center study investigated the associations between system inflammation levels and clinical outcomes in patients with TBM. Our results indicate that the elevated levels of systemic inflammation serve as predictor of early neurological deterioration and subsequent poor outcome. However, we found that dexamethasone treatment was not associated with improvements in neurological disability, and its treatment effect did not vary significantly among patients with different levels of system inflammation.
The burden of neurological disability in TBM is substantial.5 Previous studies have shown that TBM patients often presented with multiple brain lesions, including tuberculoma, cerebral infarction, and hydrocephalus.26–28 These lesions, which involve the brain parenchyma, lead to various clinical symptoms; thus, it is crucial to assess early neurological deficits in patients with TBM.21 Prior research has emphasized that functional assessment are vital in neurological disorders, and should be more closely monitored during treatment.29,30 However, no previous studies have reported early neurological deterioration in TBM patients. Our study suggests a significant association between elevated NLR levels and early neurological deterioration as well as functional disability at follow-up. A previous study reported an increased NLR in pulmonary TB patients but did not examine its association with treatment outcomes.31 In our TBM cohort, we observed a higher proportion of pulmonary TB patients exhibited elevated NLR at baseline, this may be attributed to the combined effect of chronic lung infection and the activation of inflammatory mediators released by the brain on the peripheral immune system during acute meningitis onset.11,12 Recent studies have shown conflicting results regarding the role of NLR as a prognostic biomarker in neurological disorders.32–34 In a cohort study of multiple sclerosis, the author did not identify NLR as a marker of disease activity and disability;33 however, this conclusion was drawn without considering different follow-up time points. A recent study on ischemic stroke patients found that the NLR after reperfusion therapy was associated with the severity of cerebral edema and long-term functional outcome.34 In this study, our results also indicate that NLR post-treatment can serve as a significant marker for early warning signals of neurological deterioration and poor outcome in TBM patients. These findings stress the importance of monitoring NLR during treatment.
Dexamethasone has been used as an anti-inflammatory agent to reduce early mortality rates in TBM,15 however, limited evidence supports that dexamethasone treatment is associated with long-term neurological disability in TBM or bacterial meningitis.35,36 Systemic inflammation markers are low-cost and readily available parameters that could to be useful in identifying patients who may benefit from GC,17,18 especially when compared to the application of genotype to guide GC treatment.37 In our cohort, we found that dexamethasone did not improve poor outcomes across different NLR stratifications among TBM patients, suggesting that system inflammation may be not sufficient to evaluate the efficacy of anti-inflammatory treatment. In HIV-negative TBM adults treated with dexamethasone, elevated levels of inflammatory cytokines in the CSF can predict survival response to dexamethasone. This suggests that local inflammation may play a crucial role in clinical settings.38 Meningeal enhancement is frequently observed on brain MRI in patients with TBM, indicating a more severe inflammatory process in certain individuals. Meningeal enhancement is frequently observed on brain MRI in TBM patients, indicating a more severe inflammatory process in certain individuals. In our study, we examined the treatment effect of dexamethasone on subgroups classified by brain imaging (Figures S2 and S3). However, the results did not demonstrate any benefit to support dexamethasone treatment in patients with meningeal enhancement. Future studies should investigate more inflammation stratification makers and verify the effect of adjunctive dexamethasone in patients with TBM.
Strengths and Limitations
The strengths of this study include a large sample of participants recruited from multiple centers and a robust analytical approach that selects optimal models based on objective statistical assessments. However, we acknowledged several limitations. First, as an observational study, there is a potential for residual confounding of unmeasured variables. Second, we recognized the low rate of laboratory-confirmed TBM in our cohort (14.9%), consistent with a previous study (13.2%).39 This highlights the insufficient diagnosis of definite TBM in the real world when compared to clinical trials.1 Third, paradoxical reaction is a frequent phenomenon during treatment in TBM patients,40,41 we did not design this outcome because the retrospective nature of our study and we were unable to collect repeated brain imaging and CSF data from all patients after discharge. Fourth, our dataset does not include patients co-infected with HIV, so caution should be exercised when generalizing the results to broader populations. Fifth, half of the TBM patients included in our study were classified as BMRC Grade I. Future studies with large sample sizes are needed to explore the effect of dexamethasone on neurological outcomes in a more severely affected population to confirm these findings.
Conclusion
Our study demonstrated that NLR is associated with early neurological deterioration and poor outcome in TBM patients. Further research should investigate NLR in more severely affected population to predict the clinical outcomes following anti-inflammatory therapies.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to local policy but are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank the study participants, the study group members in each of the five regional centers, and management teams in Biobank of Beijing Chest Hospital.
Yijia Guo and Ruyun Zhang contributed equally to this work as first authors.
Funding
This work was funded by the Natural Science Foundation Youth Project of Sichuan Province (2022NSFSC1596); the Youth Innovation Project of Medical Research in Sichuan Province (Q20047); the Medical Research Fund of Chengdu City (2022160); and National Natural Science Foundation of China (82102657).
Disclosure
All the authors declare that they have no conflict of interest relevant to the manuscript.
References
1. Huynh J, Donovan J, Phu NH, et al. Tuberculous meningitis: progress and remaining questions. Lancet Neurol. 2022;21(5):450–464. doi:10.1016/S1474-4422(21)00435-X
2. Davis AG, Donovan J, Bremer M, et al. Host directed therapies for tuberculous meningitis. Wellcome Open Res. 2020;5:292. doi:10.12688/wellcomeopenres.16474.1
3. Donovan J, Figaji A, Imran D, Phu NH, Rohlwink U, Thwaites GE, et al. The neurocritical care of tuberculous meningitis. Lancet Neurol. 2019;18(8):771–783. doi:10.1016/S1474-4422(19)30154-1
4. Wasay M, Farooq S, Khowaja ZA, et al. Cerebral infarction and tuberculoma in central nervous system tuberculosis: frequency and prognostic implications. J Neurol Neurosurg Psychiatry. 2014;85:1260–1264. doi:10.1136/jnnp-2013-307178
5. Wen L, Li M, Xu T, Yu X, Wang L, Li K, et al. Clinical features, outcomes and prognostic factors of tuberculous meningitis in adults worldwide: systematic review and meta-analysis. J Neurol. 2019;266(12):3009–3021. doi:10.1007/s00415-019-09523-6
6. Ballabh P, Braun A, Nedergaard M. The blood-brain barrier: an overview: structure, regulation, and clinical implications. NeurobiolDis. 2004;16:1–13.
7. Ma W, Oliveira-Nunes MC, Xu K, et al. Type I interferon response in astrocytes promotes brain metastasis by enhancing monocytic myeloid cell recruitment. Nat Commun. 2023;14(1):2632. doi:10.1038/s41467-023-38252-8
8. Engelhardt B, Vajkoczy P, Weller RO. The movers and shapers in immune privilege of the CNS. Nat Immunol. 2017;18(2):123–131. doi:10.1038/ni.3666
9. Chandra S, Sisodia SS, Vassar RJ. The gut microbiome in Alzheimer’s disease: what we know and what remains to be explored. Mol Neurodegener. 2023;18(1):9. doi:10.1186/s13024-023-00595-7
10. Tejera D, Mercan D, Sanchez-Caro JM, et al. Systemic inflammation impairs microglial Aβ clearance through NLRP3 inflammasome. EMBO J. 2019;38(17):e101064. doi:10.15252/embj.2018101064
11. Klein RS, Garber C, Howard N. Infectious immunity in the central nervous system and brain function. Nat Immunol. 2017;18(2):132–141. doi:10.1038/ni.3656
12. Shi K, TianDC L, Li Z-G, Ducruet AF, Lawton MT, Shi F-D, et al. Global brain inflammation in stroke. Lancet Neurol. 2019;18(11):1058–1066. doi:10.1016/S1474-4422(19)30078-X
13. Thwaites G, Fisher M, Hemingway C, Scott G, Solomon T, Innes J, et al. British Infection Society guidelines for the diagnosis and treatment of tuberculosis of the central nervous system in adults and children. J Infect. 2009;59(3):167–187. doi:10.1016/j.jinf.2009.06.011
14. Nahid P, Dorman SE, Alipanah N, et al. Official American thoracic society/centers for disease control and prevention/infectious diseases society of America Clinical Practice Guidelines: treatment of drug-susceptible tuberculosis. Clin Infect Dis. 2016;63:e147–95. doi:10.1093/cid/ciw376
15. Prasad K, Mamta Singh B, Ryan H, et al. Corticosteroids for managing tuberculous meningitis. Cochrane Database Syst Rev. 2016;4(4):CD002244. doi:10.1002/14651858.CD002244.pub4
16. Donovan J, Bang ND, Imran D, et al. Adjunctive dexamethasone for tuberculous meningitis in HIV-Positive Adults. N Engl J Med. 2023;389(15):1357–1367. doi:10.1056/NEJMoa2216218
17. Cai J, Li H, Zhang C, et al. The neutrophil-to-lymphocyte ratio determines clinical efficacy of corticosteroid therapy in patients with COVID-19. Cell Metab. 2021;33(2):258–269.e3. doi:10.1016/j.cmet.2021.01.002
18. Wang Q, Xie T, Gao R, et al. Neutrophil-to-lymphocyte ratio is a powerful predictor of adult patients with acute respiratory distress syndrome who might benefit from corticosteroid therapy. Am J Transl Res. 2021;13(10):11556–11570.
19. Marais S, Thwaites G, Schoeman JF, et al. Tuberculous meningitis: a uniform case definition for use in clinical research. Lancet Infect Dis. 2010;10(11):803–812. doi:10.1016/S1473-3099(10)70138-9
20. von Elm E, Altman DG, Egger M, et al. Strengthening the reporting of observational studies in epidemiology(STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335:806–808.
21. Sher K, Abbasi A, Abbasi A, et al. Stages of tuberculous meningitis: a clinicoradiologic analysis. J Coll Physicians Surg Pak. 2013;23(6):405–408.
22. Kassi E, Semaniakou A, Sertedaki A, et al. Sequencing analysis of the human glucocorticoid receptor (NR3C1) gene in multiple sclerosis patients. J Neurol Sci. 2016;363:165–169. doi:10.1016/j.jns.2016.02.054
23. Song T, Chang H, Du L, et al. Glucocorticoid receptor mutations and clinical sensitivity to glucocorticoid in Chinese multiple sclerosis patients. Neurol Sci. 2020;41(10):2767–2771. doi:10.1007/s10072-020-04376-8
24. Marik PE, Taeb AM. SIRS, qSOFA and new sepsis definition. J Thorac Dis. 2017;9(4):943–945. doi:10.21037/jtd.2017.03.125
25. African COVID-19 Critical Care Outcomes Study (ACCCOS) Investigators. Patient care and clinical outcomes for patients with COVID-19 infection admitted to African high-care or intensive care units (ACCCOS): a multicentre, prospective, observational cohort study. Lancet. 2021;397(10288):1885–1894. doi:10.1016/S0140-6736(21)00441-4
26. Abdulaziz ATA, Ren YM, Li W, et al. Comparison of Standard and Intensified Regimens for HIV-Negative Adults With Tuberculous Meningitis in West China: a retrospective observational study. Front Neurol. 2019;10:626. doi:10.3389/fneur.2019.00626
27. Li K, Tang H, Yang Y, et al. Clinical features, long-term clinical outcomes, and prognostic factors of tuberculous meningitis in West China: a multivariate analysis of 154 adults. Expert Rev Anti Infect Ther. 2017;15:629–635. doi:10.1080/14787210.2017.1309974
28. Modi M, Sharma K, Prabhakar S, et al. Clinical and radiological predictors of outcome in tubercular meningitis: a prospective study of 209 patients. Clin Neurol Neurosurg. 2017;161:29–34. doi:10.1016/j.clineuro.2017.08.006
29. National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333(24):1581–1587. doi:10.1056/NEJM199512143332401
30. Dávalos A, Cendra E, Teruel J, et al. Deteriorating ischemic stroke: risk factors and prognosis. Neurology. 1990;40(12):1865–1869. doi:10.1212/WNL.40.12.1865
31. Cursi L, Lancella L, Mariani F, et al. Monocyte-to-lymphocyte, neutrophil-to-lymphocyte and neutrophil-to-monocyte plus lymphocyte ratios in children with active tuberculosis: a multicentre study. Acta Paediatr. 2023;112(11):2418–2425. doi:10.1111/apa.16932
32. Muñoz-Delgado L, Macías-García D, Jesús S, et al. Peripheral immune profile and neutrophil-to-lymphocyte ratio in parkinson’s disease. Mov Disord. 2021;36(10):2426–2430. doi:10.1002/mds.28685
33. Gelibter S, Pisa M, Croese T, et al. Neutrophil-to-lymphocyte ratio: a marker of neuro-inflammation in multiple sclerosis? J Neurol. 2021;268(2):717–723. doi:10.1007/s00415-020-10322-7
34. Ferro D, Matias M, Neto J, et al. Neutrophil-to-lymphocyte ratio predicts cerebral edema and clinical worsening early after reperfusion therapy in stroke. Stroke. 2021;52(3):859–867. doi:10.1161/STROKEAHA.120.032130
35. Thwaites GE, Nguyen DB, Nguyen HD, et al. Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults. N Engl J Med. 2004;351(17):1741–1751. doi:10.1056/NEJMoa040573
36. van de Beek D, Farrar JJ, de Gans J, et al. Adjunctive dexamethasone in bacterial meningitis: a meta-analysis of individual patient data. Lancet Neurol. 2010;9(3):254–263. doi:10.1016/S1474-4422(10)70023-5
37. Tobin DM, Roca FJ, Oh SF, et al. Host genotype-specific therapies can optimize the inflammatory response to mycobacterial infections. Cell. 2012;148(3):434–446. doi:10.1016/j.cell.2011.12.023
38. Whitworth LJ, Troll R, Pagán AJ, et al. Elevated cerebrospinal fluid cytokine levels in tuberculous meningitis predict survival in response to dexamethasone. Proc Natl Acad Sci USA. 2021;118(10):e2024852118. doi:10.1073/pnas.2024852118
39. Feng GD, Shi M, Ma L, et al. Diagnostic accuracy of intracellular mycobacterium tuberculosis detection for tuberculous meningitis. Am J Respir Crit Care Med. 2014;189(4):475–481. doi:10.1164/rccm.201309-1686OC
40. Garg RK, Malhotra HS, Kumar N. Paradoxical reaction in HIV negative tuberculous meningitis. J Neurol Sci. 2014;340(1–2):26–36. doi:10.1016/j.jns.2014.03.025
41. Singh AK, Malhotra HS, Garg RK, et al. Paradoxical reaction in tuberculous meningitis: presentation, predictors and impact on prognosis. BMC Infect Dis. 2016;16:306. doi:10.1186/s12879-016-1625-9
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.