")
Back to Journals » Clinical Ophthalmology » Volume 19
Systemic Predictors of Diabetic Retinopathy and Diabetic Macular Edema in an Adult Veteran Population
Authors Tran EM, Gregori NZ, Rachitskaya A, Nandan A, Pershing S, Goldberg JL
Received 26 August 2024
Accepted for publication 16 December 2024
Published 8 January 2025 Volume 2025:19 Pages 101—110
DOI https://doi.org/10.2147/OPTH.S487047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Elaine M Tran,1 Ninel Z Gregori,2 Aleksandra Rachitskaya,2 Abhishek Nandan,2 Suzann Pershing,1,3 Jeffrey L Goldberg1– 3
1Byers Eye Institute at Stanford, Palo Alto, CA; 2Bascom Palmer Eye Institute/Miami VA Health Care System, Miami, FL, USA; 3VA Palo Alto Health Care System, Palo Alto, CA, USA
Correspondence: Jeffrey L Goldberg, Byers Eye Institute, Department of Ophthalmology, Stanford University School of Medicine, Palo Alto, CA, USA, Email [email protected]
Purpose: To investigate the influence of systemic and serum measures and hypoglycemic medications on the initial presentation and ongoing development of diabetic retinopathy (DR) and diabetic macular edema (DME).
Design: Using Veterans Affairs electronic health records, we identified patients with a diabetes mellitus diagnosis and at least one eye examination between 1997 and 2010. After adjusting for sociodemographic factors, we used multivariable Cox regression models to evaluate the association of hemoglobin A1c (HbA1c) levels, blood pressure, albuminuria, blood urea nitrogen (BUN), and prescribed medications with the subsequent diagnosis of 1) any diabetic eye disease (defined for this analysis as DR and/or DME, 2) diabetic retinopathy, and 3) diabetic macular edema.
Results: Of 4089 diabetic Veteran patients, 821 (20%) were subsequently diagnosed with diabetic retinopathy and 88 (2%) had macular edema. Patients were more likely to receive a diabetic retinopathy diagnosis if they presented with HbA1c > 8.5 (HR=2.66, 95% CI 1.88– 3.77, p< 0.01), systolic blood pressure > 140 mmHg (HR=1.45, 95% CI 1.26– 1.66, p< 0.01), blood urea nitrogen (BUN) > 35 mg/dL (HR=2.17, 95% CI 1.60– 2.93, p< 0.01), and/or used insulin (HR=2.04, 95% CI 1.74– 2.40, p< 0.01). Patients were more likely to be diagnosed with diabetic macular edema if they had systolic blood pressure > 140 mmHg (HR=2.00, CI 1.29– 3.08, p< 0.01) and/or used insulin (HR=2.48, CI 1.53– 4.03, p< 0.01).
Conclusion: Markers of systemic health may be useful predictors for incident diabetic retinopathy or diabetic macular edema, evaluated collectively in Veteran patients. Higher HbA1c levels, systolic blood pressure, BUN levels, and insulin use (suggestive of more severe and/or long-standing diabetes) appear to be highly associated with the development of diabetic eye disease, and, in particular, diabetic retinopathy.
Keywords: diabetes, diabetic retinopathy, HbA1c, blood pressure, albuminuria
Introduction
Diabetic retinopathy (DR) is a leading cause of acquired vision loss in working age adults in the US, and is one of the most devastating systemic complications of diabetes. DR affects between 29% and 40% of diabetic patients and is responsible for 10–12% of new cases of legal blindness each year in the US.1–3 Currently, estimated to affect over four million US adults, DR prevalence is increasing, driven by the aging US population and growing incidence of diabetes mellitus.4 Even more striking, diabetes is estimated to affect approximately 20–25% of US Veterans, and approximately 10% of US Veterans have diabetic retinopathy (representing almost 5 million patients with diabetes and approximately 1.5 million patients with diabetic retinopathy, out of a total population of over 19 million patients).5–7
Intensive glycemic control8,9 and blood pressure control10–13 have been shown to reduce the risk of retinopathy and the need for surgical or laser interventions. However, the combined effects of other clinical markers, including hyperlipidemia,14–18 blood urea nitrogen, and albuminuria,19–22 remain controversial. Furthermore, some data suggest that specific diabetes medications with potential anti-angiogenic activities may be associated with better diabetic retinopathy outcomes. For example, rosiglitazone, a thiazolidinedione insulin sensitizer that has been linked to delayed onset of proliferative diabetic retinopathy (PDR), remains on the market in the United States but may be utilized less than metformin and other hypoglycemic medications. Metformin has also been associated with lower odds of severe non-proliferative diabetic retinopathy (NPDR).23,24 To date, most analyses have considered each of these factors independently or in subsets, using different thresholds for elevated values, and there are limited data on their impact considered in aggregate, adjusting for other variables.25,26
Using electronic health record data from a Veteran Affairs (VA) healthcare system comprising over 4000 diabetic patients with up to 14 years of eye examination data, we evaluated the adjusted associations of demographics, clinical measurements, and medications with the subsequent development of diabetic eye disease, including diabetic retinopathy and clinically significant diabetic macular edema (DME).
Methods
Data Source and Study Design
We performed a retrospective cohort analysis of patients diagnosed with diabetes mellitus who visited the eye clinic at Miami VA Medical Center. Data were collected between January 1997 and December 2010. Using data from the Computerized Patient Record System (CPRS) electronic health record (EHR), we identified patients with a diabetes diagnosis and at least one recorded eye examination, and clinical variables were extracted into a secure database. Descriptive and multivariate Cox regression analyses were performed for three ocular health outcomes: any diabetic eye disease, diabetic retinopathy, and diabetic macular edema. Miami VA Healthcare System Institutional Review Board (IRB) and Stanford University IRB approval was obtained for the study, including data analysis, with approval for a waiver of consent based on considerations including minimal risk to patients, confidentiality protections, retrospective nature of the research, and infeasibility of contacting patients. The study was performed in compliance with the Declaration of Helsinki.
Predictor Variables
Patient age, ethnicity, sex, HbA1c level, systolic blood pressure, cholesterol level, blood urea nitrogen (BUN) level, urine albumin level, and use of diabetes medications were identified directly from the EHR. For each variable, we used the closest data recorded at or after each patient’s initial eye clinic visit to the Miami VA Medical Center. We also calculated the duration of diabetes, measured as the time from the diabetes diagnosis. The systemic predictors were evaluated as categorical variables. HbA1c levels were categorized into four groups: less than 6.0, between 6.0 and less than 7.0, between 7.0 and 8.5, and greater than 8.5. BUN levels were classified as 20 mg/dL, 20–35 mg/dL, and greater than 35 mg/dL. High blood pressure was defined as a systolic blood pressure measurement of 140 mmHg or greater, albuminuria as urinary albumin ≥ 5.0 g or greater, and high cholesterol as total cholesterol ≥ 240 mg/dL. The medications included in the analyses were insulin, metformin, glipizide, glyburide, and rosiglitazone based on their availability during the study period. Medications were identified from VA pharmacy records.
Outcome Variables
We identified diabetic eye disease using International Classification of Diseases, 9th edition, Clinical Modification (ICD-9-CM) codes. Three primary outcomes were evaluated: (1) incident diabetic retinopathy, (2) incident diabetic macular edema, and (3) incident diabetic eye disease. Diabetic eye disease was defined as diabetic retinopathy and/or diabetic macular edema. Specific ICD-9-CM codes are listed in Supplemental Table 1.
Statistical Analysis
All statistical analyses were performed using Stata version 15 (StataCorp, College Station, TX, USA) and SAS (version 9.4, SAS Institute, Cary, NC, USA) software. Descriptive statistics were summarized for categorical variables as percentages and for continuous variables as means and standard deviations. We excluded patients with missing values for any predictor variables. Using multivariable Cox proportional hazards regression with a statistical significance threshold of less than 0.05, we evaluated the association of systemic factors with diagnoses of any diabetic eye disease, diabetic retinopathy, and DME, respectively. Time from diabetes diagnosis was analyzed as a time-dependent variable, and the analysis index was defined as the date of the first observed eye clinic visit. Variables that did not reach significance in the univariate Cox analysis were excluded from the multivariate models (with the exception of cholesterol levels, which were included in the final models for clinical validity). We additionally performed sensitivity analyses, excluding patients diagnosed with diabetic eye disease at their initial eye clinic visit.
Results
Study Sample and Baseline Characteristics
A total of 4089 diabetic Veteran patients met study inclusion criteria. Of these, 821 were diagnosed with diabetic retinopathy and 88 with DME during the analysis period (Table 1). Consistent with the Veteran population, the vast majority of patients were male (97%) (Table 2). Caucasian patients comprised the largest ethnic group (41%). Patient ages ranged from 20 to 98 years, with a mean age of 64 years. The sample trended toward slightly elevated HbA1c levels (mean 7.4), prehypertension (mean systolic blood pressure of 135 mmHg), and high cholesterol levels (mean 184 mg/dL). Most patients were on oral diabetes medication (78%) and a substantial proportion were on insulin (22%). Patients were followed for up to 11.4 years (mean 2.9 years) from their first eye clinic visit to last observed visit.
 |
Table 1 Diagnoses of Eye Disease |
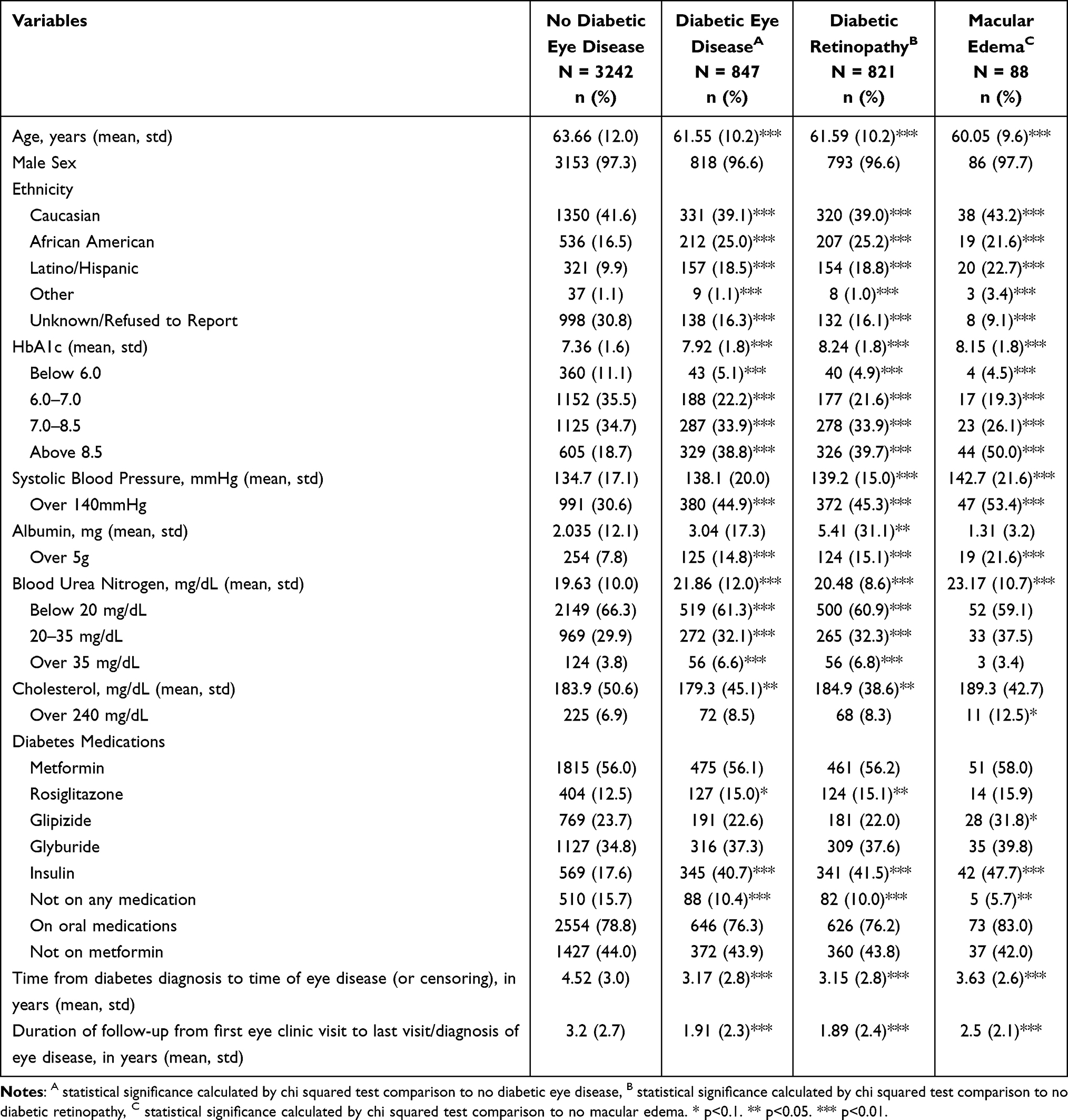 |
Table 2 Baseline Characteristics Measured at First Eye Clinic Visit |
Systemic Factors and Likelihood of Incident Diabetic Eye Disease
All systemic factors except cholesterol levels were significantly associated with the development of any diabetic eye disease (Table 3). Elevated HbA1c levels had the strongest association; patients with presenting HbA1c over 8.5 were more than twice as likely to be diagnosed with diabetic eye disease during the study period (HR=2.49, 95% CI 1.78–3.49, p<0.01). High systolic blood pressure >140 mmHg, albuminuria >5 g, and BUN >20 mg/dL were also significantly associated with 36–48% greater likelihood of developing diabetic eye disease. The only diabetes medication that was significantly associated with likelihood of diabetic eye disease was insulin use (HR=2.03, 95% CI 1.73–2.37, p<0.01). In addition to systemic factors, African American and Latino/Hispanic patients also had a higher likelihood of developing diabetic eye disease (African American: HR=1.29, 95% CI 1.07–1.55, p<0.01; Latino/Hispanic: HR=1.75, 95% CI 1.44–2.13, p<0.01). Interestingly, time since diabetes diagnosis was not significantly predictive of the likelihood of diabetic eye disease after adjusting for other patient factors.
 |
Table 3 Multivariate Cox Regression of Baseline Predictors for Diagnosis of Diabetic Eye Disease |
Systemic Factors and Likelihood of Incident Diabetic Retinopathy or Diabetic Macular Edema
We observed similar patterns when we specifically evaluated likelihood of developing diabetic retinopathy. Patients with HbA1c levels over 8.5 were over two times more likely to develop diabetic retinopathy (HR=2.66, 95% CI 1.88–3.77, p<0.01), patients with elevated systolic blood pressure were over 40% more likely (HR=1.45, 95% CI 1.26–1.66, p<0.01), and those with high BUN >35mg/dL (HR=2.17, 95% CI 1.60–2.93, p<0.01) or taking insulin (HR=2.04, 95% CI 1.74–2.40, p<0.01) were approximately twice as likely to develop diabetic retinopathy. (Table 4).
 |
Table 4 Multivariate Cox Regression of Baseline Predictors for Diagnosis of Diabetic Retinopathy |
High systolic blood pressure (HR=2.00, 95% CI 1.29–3.08, p<0.01) and insulin use (HR=2.48, 95% CI 1.53–4.03, p<0.01) remained significantly associated with the development of DME. The other variables were not statistically significant; however, results were limited by a small sample size. (Supplemental Table 2).
Sensitivity analyses excluding patients diagnosed with diabetic eye disease at their initial eye clinic visit yielded comparable results for all outcomes (Supplemental Tables 3-5).
Discussion
We assessed 4089 diabetic Veteran patients who were followed with eye clinic visits for a mean of 2.9 years. We found a greater likelihood of developing diabetic eye disease among patients who were older, of African American race or Latino/Hispanic ethnicity, treated with insulin, and/or presented with high HbA1c, high systolic blood pressure, and/or high BUN.
Patients who presented with HbA1c greater than 8.5 at their first VA eye clinic visit were more than twice as likely to develop diabetic eye disease compared to those with lower HbA1c measurements, after adjusting for other patient demographic and systemic factors. This is consistent with previous studies,8,9,25 supported here in a large-scale analysis of Veteran patients, including follow-up data to identify incident diabetic retinopathy and diabetic macular edema, as well as adjustment for other clinical variables. Patients who present with high HbA1c levels may have more difficulty in controlling their diabetes, whether through medication resistance, brittle diabetes, and/or obstacles to obtaining or adhering to care.
High systolic blood pressure at the initial eye clinic visit was also strongly associated with subsequent development of diabetic eye disease, diabetic retinopathy, and clinically significant DME. Although the effect size for high systolic blood pressure was lower than that for elevated HbA1c, it remained consistently significant across all the models. These findings support previous guidelines for tight blood pressure control to reduce the risk of complications from diabetic eye disease,13,27 as well as to prevent diabetic retinopathy progression.28,29 We did not observe a significant difference in the odds of diabetic eye disease based on cholesterol levels.
Previous analyses of the possible association between albuminuria and diabetic retinopathy have presented mixed findings. Although many studies have reported a positive association,30–32 others have reported little or no association.20 However, most studies have been cross-sectional and evaluated relatively small samples. Similarly, a positive association has been reported between BUN and diabetic retinopathy progression,33 but based on limited longitudinal data. The findings in the analysis presented here demonstrate a strong relationship between albuminuria and BUN with diabetic eye disease, even after adjusting for other systemic factors such as blood glucose control and blood pressure, suggesting the potential of these systemic markers as additional predictors of diabetic eye disease on first presentation with diabetes. This finding makes sense, given that retinopathy and nephropathy each reflect microvascular disease and may develop concomitantly.34–37
We did not identify a statistically significant relationship between specific oral diabetic medications, including metformin and rosiglitazone, and the likelihood of developing diabetic eye disease. This may reflect our limited sample size, however, interestingly, neither metformin nor thiazolinediones trended to a protective effect in our analysis. Use of insulin, however, was associated with approximately two-fold higher odds of developing diabetic eye disease, even after adjusting for blood glucose control and other systemic factors. This likely reflects the cumulative effect of many years with diabetes, disease that is poorly-controlled, and/or more brittle, treatment-resistant disease, since most patients are not started on insulin as a first-line therapy, and longer diabetes duration is recognized as a risk factor for diabetic eye disease. Interestingly, after adjusting for medications and other factors, diabetes duration (time since diagnosis) was not associated with a significant difference in odds of diabetic eye disease. This suggests that a longer duration of diabetes does not confer additional risk directly; instead, it does so via the cumulative effect of suboptimal control of blood glucose and other biomarkers.
Our study has several limitations. Our data did not differentiate between type 1, type 2, drug- or chemically induced diabetes, or diabetes due to other underlying conditions, and was notable for a smaller sample size of diabetic macular edema patients for analysis. Furthermore, although albumin is usually measured with creatinine to calculate a ratio in the diagnosis of clinical albuminuria, we did not have complete data on creatinine values to calculate a ratio. However, high albumin itself is a sign of kidney dysfunction, thus we used a threshold of 5 g for albuminuria since high albumin in urine (especially at 5 g) is highly suggestive of some kidney dysfunction. Even a very high creatinine level (eg, 100) would result in a ratio of 50, which is well above a normal urine albumin-to-creatinine ratio (≤30 mg/g). We also did not include newer diabetes medications that were not available for the duration of our analysis period (eg, Sodium-Glucose CoTransporter-2 [SGLT2] Inhibitors and most Glucagon-Like Peptide-1 [GLP-1] receptor agonists), which are an important topic for future study.38 Given the retrospective nature of our study, it is also possible that there were other confounding variables (such as smoking) that may have influenced the primary outcome. At least one study, however, has suggested against the implication of smoking as a significant risk factor for diabetic retinopathy, which is a stark variance from its implications in diabetic macrovascular disease.39 Moreover, the inclusion of many traditional and non-traditional variables of risk for diabetic eye disease is a strength of our study.
We identified diabetic eye disease based on documented retinopathy and DME diagnoses at eye clinic visits; however, patients may not have been seen in the VA or VA eye clinic with regular frequency. It is possible that diabetic eye disease may develop earlier in some patients but not be documented in the EHR if no eye clinic visits occurred. Patients may also have been lost to follow-up before detection and documentation of diabetic eye disease, particularly given a shorter-than-optimal mean duration of follow-up data (2.9 years after diagnosis). Confounding factors, including socioeconomic determinants of health, may influence how soon patients are seen during the course of their disease, the regularity of their general medical or eye care, and their adherence to prevention and treatment guidelines. Patients may wait to seek eye care or may have delayed referral to an ophthalmologist, such that diabetic eye disease is first diagnosed later in the course of their disease or not at all during our observed study period. However, this was mitigated by the fact that our analysis was based on VA health plan data. All diabetic patients in the VA are required to receive an annual eye examination either in person or via telemedicine. VA achieves an approximately 90% success rate in annual screening, compared to approximately 58% in the community.40 Furthermore, we would expect infrequent eye examinations and unobserved diabetic eye disease to bias our analysis away from finding a significant effect; the fact that we still observe a difference suggests that the findings are valid.
Our findings are based on data from a single VA healthcare system, and as such are also specific to the Veteran population. The generalizability of findings outside this population may also be notably limited, particularly for women and ethnic minorities, because our sample consisted mostly of male patients who visited the Miami VA healthcare system. Similarly, patients residing in other geographic regions may have had different findings. Future research should benefit from a larger and more diverse population. Additionally, visual acuity is not currently captured in VA electronic health records in a structured format but work is actively in progress using natural language processing approaches to capture this data broadly within VA unstructured text records; vision compromise/severity (BCVA) is another important outcome measure for future research, as well as analysis of diabetic retinopathy and diabetic macular edema that requires treatment (as another measure of treatment-indicated sight-threatening disease). However, aside from these limitations, this analysis captures a large proportion of Veteran patients with diabetes in a real-world setting and yields important insights into the adjusted impact of systemic factors on structured measure of diabetic eye disease, specifically diabetic retinopathy and diabetic macular edema.
Conclusions
Diabetic retinopathy remains one of the most prevalent preventable causes of vision loss in adult populations. Regular evaluation and intense control of systemic factors have been proven to be effective at delaying the advancement of this disease. This study presents an important multivariable analysis of a unique array of systemic factors evaluated in concert in a Veteran patient population. Findings suggest that ideal ophthalmic care should include a thorough assessment of systemic biomarkers, as well as particular consideration for Veteran minority groups at increased risk of developing diabetic eye disease (diabetic retinopathy and/or diabetic macular edema). Multi-targeted risk factor control is important to reduce the incidence of diabetic eye disease, regardless of the medication selected. Ophthalmologists can play a key role in ensuring that systemic predictors are regularly evaluated and optimized to reduce the burden of diabetic eye disease.
Acknowledgments
Presented in part at the Association for Research in Vision and Ophthalmology, May 2017.
Funding
Stanford University School of Medicine MedScholars Fund (ET); departmental support from Research to Prevent Blindness and National Eye Institute (P30-EY026877) (ET, SP, JLG). The funding organizations had no role in the design or conduct of this research.
Disclosure
Dr Aleksandra Rachitskaya reports Consulting: AbbVie/Allergan, Alcon, Apellis Pharmaceuticals, Regeneron, Iveric Bio, Roche/Genentech, Ocular Therapeutix, Samsara, EyePoint, Boehringer Ingelheim, 4D Molecular Therapeutics; Scientific Advisory Board: Samsara; Speakers’ Bureau: Apellis Pharmaceuticals, Iveric Bio, Genentech, RegeneronResearch Grants: Beacon Therapeutics, Apellis Pharmaceuticals, DRCR Retina Network, and Roche/Genentech, Regeneron. Dr Suzann Pershing reports grants from NIH, Research to Prevent Blindness, during the conduct of the study; personal fees from Acumen, LLC and Verana Health, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. National diabetes statistics report. 2022. Available from: https://www.cdc.gov/diabetes/data/statistics-report/index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fdiabetes%2Fdata%2Fstatistics%2Fstatistics-report.html.
2. Cheng YJ, Gregg EW, Geiss LS, et al. Association of A1C and fasting plasma glucose levels with diabetic retinopathy prevalence in the U.S. population: implications for diabetes diagnostic thresholds. Diabetes Care. 2009;32(11):2027–2032. doi:10.2337/dc09-0440
3. Varma R, Torres M, Peña F, Klein R, Azen SP. Prevalence of diabetic retinopathy in adult Latinos: the Los Angeles Latino eye study. Ophthalmology. 2004. doi:10.1016/j.ophtha.2004.03.002
4. Kempen JH, O’Colmain BJ, Leske MC, et al. The Prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol. 2004. doi:10.1001/archopht.122.4.552
5. Diabetes Mellitus. In Federal healthcare data trends 2017. Federal Practitioner, 2017. S20–S21. Available from: https://www.fedprac-digital.com/federalpractitioner/data_trends_2017?pg=20#pg20.
6. Orcutt J, Avakian A, Koepsell TD, Maynard C. Eye disease in veterans with diabetes. Diabetes Care. 2004;27(Suppl 2):B50–3. PMID: 15113783.doi:10.2337/diacare.27.suppl_2.b50
7. Miller DR, Safford MM, Pogach LM. Who has diabetes? Best estimates of diabetes prevalence in the department of veterans affairs based on computerized patient data. Diabetes Care. 2004;27(Suppl 2):B10–21. PMID: 15113777.doi:10.2337/diacare.27.suppl_2.b10
8. Nathan DM, Genuth S; Diabetes Control and Complications Trial Research Group, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993. doi:10.1056/NEJM199309303291401
9. Turner R, Dahl MG, Shuster S, Rees JL. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9132). doi:10.1016/S0140-6736(98)07019-6
10. Kohner EM, Aldington SJ, Stratton IM, et al. United Kingdom prospective diabetes study, 30: diabetic retinopathy at diagnosis of non-insulin-dependent diabetes mellitus and associated risk factors. Arch Ophthalmol. 1998;116(3):297. doi:10.1001/archopht.116.3.297
11. Chase P, Garg S, Jackson W, et al. Blood pressure and retinopathy in type I diabetes. Ophthalmology. 1990;97(2):155–159. doi:10.1016/S0161-6420(90)32611-8
12. Gillow JT, Gibson JM, Dodson PM. Hypertension and diabetic retinopathy - What’s the story? Br J Ophthalmol. 1999;83(9):1083–1087. doi:10.1136/bjo.83.9.1083
13. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ. 2011. doi:10.1136/bmj.317.7160.703
14. Gall M-A, Hougaard P, Borch-Johnsen K, Parving -H-H. Risk factors for development of incipient and overt diabetic nephropathy in patients with non-insulin dependent diabetes mellitus: prospective, observational study. BMJ. 2011. doi:10.1136/bmj.314.7083.783
15. Ravid M, Brosh D, Ravid-Safran D, Levy Z, Rachmani R. Main risk factors for nephropathy in type 2 diabetes mellitus are plasma cholesterol levels, mean blood pressure, and hyperglycemia. Arch Intern Med. 1998;158(9):998. doi:10.1001/archinte.158.9.998
16. Verrotti A, Lobefalo L, Chiarelli F, et al. Lipids and lipoproteins in diabetic adolescents and young adults with retinopathy. Eye. 1997;11(6):876–881. doi:10.1038/eye.1997.225
17. Kordonouri O, Danne T, Hopfenmüller W, Enders I, Hövener G, Weber B. Lipid profiles and blood pressure: are they risk factors for the development of early background retinopathy and incipient nephropathy in children with insulin-dependent diabetes mellitus? Acta Paediatr Int J Paediatr. 1996;85(1):43–48. doi:10.1111/j.1651-2227.1996.tb13888.x
18. Larsson LI, Alm A, Bergenheim T, Lithner F, Bergström R. Retinopathy in diabetic patients aged 15-50 years in the county of Umea, Sweden. Acta Ophthalmol Scand. 1999. doi:10.1034/j.1600-0420.1999.770415.x
19. Manaviat MR, Afkhami M, Shoja MR. Retinopathy and microalbuminuria in type II diabetic patients. BMC Ophthalmol. 2004;4(1). doi:10.1186/1471-2415-4-9
20. Erasmus RT, Oyeyinka G, Arijel A. Microalbuminuria in non-insulin-dependent (type 2) Nigerian diabetics: relation to glycaemic control, blood pressure and retinopathy. Postgrad Med J. 1992;68(802):638–642. doi:10.1136/pgmj.68.802.638
21. Kim CH, Kim HK, Park JY, et al. Association of microalbuminuria and atherosclerotic risk factors in non- diabetic subjects in Korea. Diabet Res Clin Pract. 1998;40(3):191–199. doi:10.1016/S0168-8227(98)00029-1
22. Shen LQ, Child A, Weber GM, Folkman J, Aiello LP. Rosiglitazone and delayed onset of proliferative diabetic retinopathy. Arch Ophthalmol. 2008;126(6):793. doi:10.1001/archopht.126.6.793
23. Yi QY, Deng G, Chen N, et al. Metformin inhibits development of diabetic retinopathy through inducing alternative splicing of VEGF-A. Am J Transl Res. 2016;8(9):3947–3954.
24. Li Y, Ryu C, Munie M, et al. Association of metformin treatment with reduced severity of diabetic retinopathy in type 2 diabetic patients. J Diabetes Res. 2018;2018:1–8. doi:10.1155/2018/2801450
25. Tarasewicz D, Conell C, Gilliam LK, Melles RB. Quantification of risk factors for diabetic retinopathy progression. Acta Diabetol. 2023;60(3):363–369. PMID: 36527502.doi:10.1007/s00592-022-02007-6
26. Ghamdi AHA. Clinical predictors of diabetic retinopathy progression; a systematic review. Curr Diabetes Rev. 2020;16(3):242–247. PMID: 30767747.doi:10.2174/1573399815666190215120435.
27. Matthews DR, Stratton IM, Aldington SJ, Holman RR, Kohner EM. Risks of progression of retinopathy and vision loss related to tight blood pressure control in type 2 diabetes mellitus: UKPDS 69. Arch Ophthalmol. 2004;122(11):1631–1640. doi:10.1001/archopht.122.11.1631
28. Schrier RW, Estacio RO, Esler A, Mehler P. Effects of aggressive blood pressure control in normotensive type 2 diabetic patients on albuminuria, retinopathy and strokes. Kidney Int. 2002;61(3):1086–1097. doi:10.1046/j.1523-1755.2002.00213.x
29. Klein R. Is blood pressure a predictor of the incidence or progression of diabetic retinopathy? Arch Intern Med. 2011. doi:10.1001/archinte.1989.00390110033008
30. Cruickshanks KJ, Ritter LL, Klein R, Moss SE. The association of microalbuminuria with diabetic retinopathy: the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Ophthalmology. 1993;100(6):862–867. doi:10.1016/S0161-6420(93)31562-9
31. Parving HH, Hommel E, Mathiesen E, et al. Prevalence of microalbuminuria, arterial hypertension retinopathy and neuropathy in patients with insulin dependent diabetes. Br Med J. 1988;296(6616):156–160. doi:10.1136/bmj.296.6616.156
32. Savage S, Estacio RO, Schrier RW, Schrier RW. Urinary albumin excretion as a predictor of diabetic retinopathy, neuropathy, and cardiovascular disease in NIDDM. Diabetes Care. 1996;19(11):1243–1248. doi:10.2337/diacare.19.11.1243
33. Matsuyama K, Ogata N, Matsuoka M, et al. Relationship between pigment epithelium-derived factor (PEDF) and renal function in patients with diabetic retinopathy. Mol Vis. 2008;14:992–996.
34. He F, Xia X, Wu XF, Yu XQ, Huang FX. Diabetic retinopathy in predicting diabetic nephropathy in patients with type 2 diabetes and renal disease: a meta-analysis. Diabetologia. 2013;56(3):457–466. doi:10.1007/s00125-012-2796-6
35. Grunwald JE, Pistilli M, Ying GS, et al. Retinopathy and progression of CKD: the cric study. Clin J Am Soc Nephrol. 2014;9(7):1217–1224. doi:10.2215/CJN.11761113
36. Lee WJ, Sobrin L, Lee MJ, Kang MH, Seong M, Cho H. The relationship between diabetic retinopathy and diabetic nephropathy in a population-based study in Korea (KNHANES V-2, 3). Investig Ophthalmol Vis Sci. 2014;55(10):6547. doi:10.1167/iovs.14-15001
37. Ahmed MH, Elwali ES, Awadalla H, Almobarak AO. The relationship between diabetic retinopathy and nephropathy in Sudanese adult with diabetes: population based study. Diabetes Metab Syndr Clin Res Rev. 2017;11:S333–S336. doi:10.1016/j.dsx.2017.03.011
38. Joo JH, Sharma N, Shaia J, et al. The effect of GLP-1 receptor agonists on diabetic retinopathy at a tertiary care center. Ophthalmology Sci. 2024;4(6):100547. doi:10.1016/j.xops.2024.100547
39. Moss SE, Klein R, Klein BE. Association of cigarette smoking with diabetic retinopathy. Diabetes Care. 1991;14(2):119–126. PMID: 2060413.doi:10.2337/diacare.14.2.119.
40. US Department of Veteran Affairs. Diabetes care eye exams. QUALITY OFCARE. 2017. Available from: https://www.va.gov/QUALITYOFCARE/initiatives/compare/diabetes-care-eye-exams.asp.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Telehealth Encourages Patients with Diabetes in Racial and Ethnic Minority Groups to Return for in-Person Ophthalmic Care During the COVID-19 Pandemic
Ramsey DJ, Lasalle CC, Anjum S, Marx JL, Roh S
Clinical Ophthalmology 2022, 16:2157-2166
Published Date: 4 July 2022
Non-Traditional Blood Lipid Indices for Metabolism Dysfunction-Associated Fatty Liver Disease Prediction in Non-Obese Type 2 Diabetes Mellitus
Gao Q, Feng L, Zhou W, Li X, Yin L, Wang Y
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2345-2354
Published Date: 7 August 2023
Correlation Between Blood Glucose Indexes Generated by the Flash Glucose Monitoring System and Diabetic Vascular Complications
Sheng X, Li T, Hu Y, Xiong CS, Hu L
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2447-2456
Published Date: 16 August 2023
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025
Predictors of Blood Pressure, Cholesterol, and Cardiovascular Screening Among Saudis at Primary Healthcare Settings in Riyadh, Saudi Arabia
Alhawiti NM, Shubair MM, Nasser SM, Alharthy A, Al-Khateeb BF, Othman F, Alshahrani A, Alnaim L, Abukhamis AA, Alwatban N, El-Metwally A
Patient Preference and Adherence 2025, 19:1433-1447
Published Date: 13 May 2025