")
Back to Journals » Clinical Ophthalmology » Volume 18
Tear Film Hyperosmolarity is Associated with Increased Variation of Light Scatter Following Cataract Surgery
Authors Sullivan BD, Palazón de la Torre M, Yago I, Duarte R, Schallhorn JM , Nijm LM, White DE, Berg MS, Artal P
Received 29 June 2024
Accepted for publication 21 August 2024
Published 28 August 2024 Volume 2024:18 Pages 2419—2426
DOI https://doi.org/10.2147/OPTH.S484840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Benjamin D Sullivan,1 Marta Palazón de la Torre,2 Ines Yago,2 Raúl Duarte,3 Julie M Schallhorn,4 Lisa M Nijm,5 Darrell E White,6 Michael S Berg,1 Pablo Artal3
1Trukera Medical, Southlake, TX, USA; 2Oftalmología en Murcia, Hospital Universitario Virgen de la Arrixaca, Murcia, Spain; 3Laboratorio de Optica, Universidad de Murcia, Murcia, Spain; 4Francis I. Proctor Foundation and Department of Ophthalmology, University of California, San Francisco, CA, USA; 5Department of Ophthalmology and Visual Sciences, University of Illinois Eye and Ear Infirmary, Chicago, IL, USA; 6SkyVision Centers, Westlake, OH, USA
Correspondence: Benjamin D Sullivan, Email [email protected]
Purpose: To study the association between tear film hyperosmolarity and ocular light scatter in a cataract surgery population.
Patients and Methods: Contiguous, 20-second objective scatter index (OSI) scans were recorded in hyperosmolar (≥ 320 mOsm/L) and normal subjects (< 308 mOsm/L) with cataract nuclear opacity ≥ 3. OSI was measured at screening, baseline and 90 days following surgery. Along with symptoms of ocular surface disease, slit-lamp examination included corneal staining (0– 3), tear film breakup time (TBUT) and evaluation of meibomian gland disease (MGD). An additional cohort of hyperosmolar subjects were measured for OSI at screening, baseline, and 5, 10, 15 and 30 minutes following instillation of 0.18% sodium hyaluronate (HA).
Results: Thirty-one eyes of 31 patients were included. There was a significant difference in post-operative OSI variation when comparing hyperosmolar (0.65± 0.30, N=11) to normal subjects (0.33± 0.11, N=10, p=0.005). Of note, there were no significant differences in OSI variation when subjects were sorted by staining (p=0.9), TBUT (p=0.7), symptoms (p=0.7), or MGD status (p=0.9). Instillation of 0.18% HA (N=10) did not alter OSI at 5 minutes, but significant reductions in OSI of 28.8%, 38.5% and 36.7% (all p < 0.001) were observed at 10, 15 and 30 minutes.
Conclusion: Hyperosmolar patients exhibited significantly increased variation in light scatter following cataract surgery that was undifferentiated by staining or TBUT. Elevated osmolarity may be indicative of light scatter equivalent to that of a grade 2– 3 cataract.
Keywords: hyperosmolarity, light scatter, tear film, staining, TBUT, cataract
Introduction
Tear film hyperosmolarity acts as a potent cellular stress on the ocular surface that can induce epithelial cell death and compromise the barrier functions of the cornea.1,2 Hyperosmolarity has been shown to be associated with significant (>1.0 diopter (D)) test-to-test variations in the measured corneal astigmatism and >0.5 D variations in IOL power, adding noise that functionally limits the resolution of keratometry and increases the likelihood of unexpected refractive error after cataract surgery.3 A second study found that pre-operative hyperosmolarity was correlated with greater post-operative ametropia and reduced uncorrected distance visual acuity (UDVA) as well as greater post-operative dissatisfaction compared to normal osmolarity controls.4 Neither study demonstrated correlation with clinical parameters such as corneal staining or tear breakup time (TBUT).3,4
Although prior research has shown that tear film hyperosmolarity can compromise pre-surgical measurements and impact post-surgical outcomes, it is not currently known whether hyperosmolarity is directly associated with aberrant visual sequelae. Therefore, our current hypothesis is that hyperosmolarity is associated with increased variation in light scatter between blinks, and specifically, that this effect is not observable under a slit lamp. If this hypothesis is correct, it would likely help to explain a portion of the phenomenon of a post-operative patient that achieves target refraction, has an unremarkable ocular surface, but is dissatisfied with the overall quality of vision – colloquially known as the 20/20 unhappy patient.
Materials and Methods
Study Design and Ethics
This was a prospective comparative study of ocular light scatter in patients with visually significant cataract in patients with and without hyperosmolarity. This study conformed to the tenants of the Declaration of Helsinki and informed consent was obtained from all subjects prior to participation. The study was reviewed and approved by the ethics committee of the Hospital Universitario Virgen de la Arrixaca, Murcia, Spain. It was performed at a single site, Servicio de Oftalmología, Hospital Universitario Virgen de la Arrixaca. Murcia, Spain. There were two arms of the study: 1) a cataract surgery arm, and 2) an artificial tear arm. Subjects in the cataract arm were classified into normal and hyperosmolar in an attempt to understand the impacts of osmolarity on light scatter before and after surgery. Subjects in the artificial tear arm were hyperosmolar dry eye patients and were observed before and after instillation of an artificial tear to understand the relative contribution of osmolarity to light scatter.
Clinical Assessments
For each subject, binary (yes/no) symptoms of ocular surface disease were recorded, including: dry eyes, blurry vision, redness, burning, itching, light sensitivity, tearing, tired eyes, stringy mucus, foreign body sensation, contact lens discomfort, scratchy feeling of sand or grit, fluctuating vision, as well as severity (anchors mild and severe) of disease on a 1–10 integer scale. Slit-lamp examination included Oxford corneal fluorescein staining,5 manual fluorescein tear film breakup time (TBUT) measured in triplicate and averaged for each eye, and evaluation of the existence of meibomian gland disease (MGD) by clinical opinion. Contiguous, 20-second duration double-pass based Objective Scatter Index (OSI) scans were performed using an HD Analyzer with customized software to allow for extended recording (Visiometrics, Spain). Subjects were asked to blink freely during OSI measurement. Bilateral tear film osmolarity was measured using a ScoutPro Osmolarity System (Trukera Medical, USA). Subjects refrained from administering any tear supplements two hours before the osmolarity test, which was performed prior to any other invasive diagnostic test or slit-lamp exam.
Inclusion & Exclusion Criteria
The cataract cohort included subjects 18 years of age or older that were scheduled for surgery utilizing a one-piece aspheric monofocal intraocular lens (IOL) with nuclear opacity (NO) ≥3 and an Objective Scattering Index (OSI) ≥4.0 using the HD Analyzer (Visiometrics, Spain).6 Subjects were classified as either normal osmolarity (osmolarity < 308 mOsm/L) or hyperosmolar (osmolarity ≥ 320 mOsm/L) using the Scout Pro (Trukera Medical, USA).7 Subjects were excluded if they had previous cataract surgery or exhibited any signs of glaucoma, retinal disease, diabetes, corneal dystrophy, uveitis, pterygia, pregnancy, compromised cognitive ability, or an unwillingness or inability to sign the informed consent form. OSI was measured at screening, baseline (within 1–14 days of screening) and 90 days following surgery. Subjects were asked not to begin or change the dose of ocular medication, nutritional supplements or systemic medication known to affect tear production including, but not limited to antihistamines, antidepressants, diuretics, corticosteroids or immunomodulators between screening and baseline.
Measurement Details and Statistics
In addition to OSI, OSI variation (defined as the standard deviation of a 20-second scan) was calculated for each subject at each time point. In the artificial tear arm of the study, hyperosmolar dry eye subjects (≥ 320 mOsm/L, OD or OS) were measured for OSI (20-second scans) at screening, baseline, and 5, 10, 15 and 30 minutes following instillation of a hypotonic, 150 mOsm/L, 0.18% sodium hyaluronate (Vismed, TRB Chemedica). The hyperosmolar dry eye subjects did not have cataracts.
To estimate the effect size for a clinically meaningful OSI variation, a series of 20-second traces of Gaussian noise were simulated with standard deviations set to match an approximate range of 2.5 OSI units (max-min) for modeled hyperosmolar and 1.5 OSI units for normal subjects. The standard deviations were optimized to 0.68±0.11 and 0.41±0.06 to match the estimated max-min OSI variation. When using the average standard deviation as a denominator, the model produced an expected effect size of 3.2. According to G*Power 3.1, with an alpha of 0.001 (to allow for multiple comparisons) and 95% power, the sample size was 8 subjects per group for a two tailed t-test to be able to resolve such an effect. A Student’s t-test with Bonferroni adjustments for multiplicity was conducted on the primary endpoint of the OSI variation.
Results
Thirty-one eyes of 31 patients were included. Twenty-one patients were in the cataract group, of these 10 were of normal osmolarity and 11 were hyperosmolar. Ten additional hyperosmolar eyes were included in the dry eye, non-cataract group. At 2 Hz, the OSI recordings generated 4920 estimates of light scatter across the subject cohort. Table 1 shows the demographics and study parameters of the three cohorts.
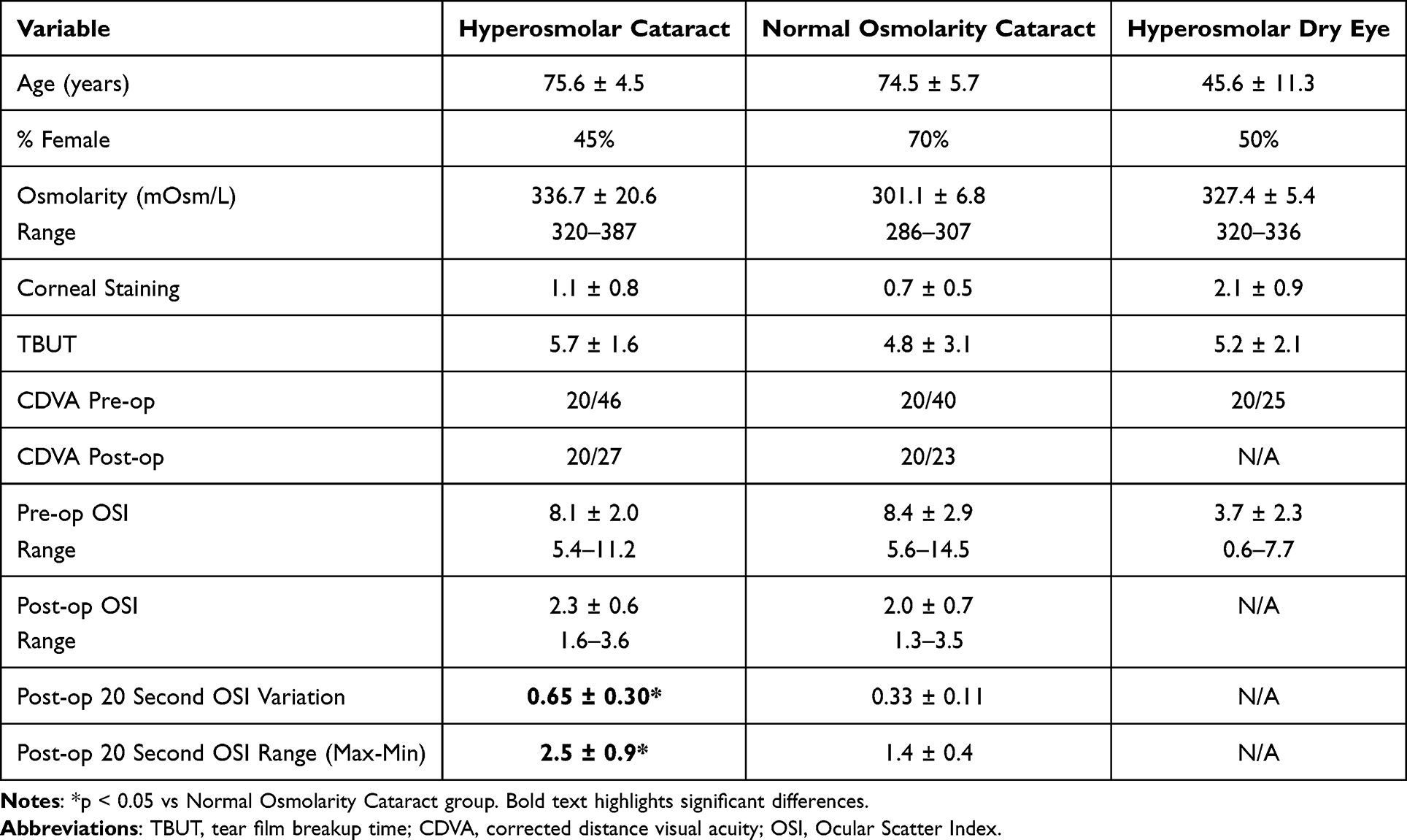 |
Table 1 Demographic and Study Information for the Patients Included in the Study. Hyperosmolar Patients Had a Baseline Tear Osmolarity ≥320 mOsm/L |
Hyperosmolar cataract patients (0.65±0.30 OSI) exhibited a significantly higher OSI variation at 3 months post-operation than normal osmolarity cataract patients (0.33±0.11 OSI, p=0.005). Although the mean light scatter as measured by OSI was not significantly different between groups, the variation (standard deviation over a 20-second scan) was markedly different between hyperosmolar and normal osmolar cohorts, demonstrating a dynamic fluctuation in vision not observed in normal subjects.
Figure 1 shows representative OSI traces of hyperosmolar and normal subjects before and after surgery. Large magnitude, high-frequency variations on the order of 2–3 OSI units were observed in hyperosmolar subjects, with some pre-operative fluctuations reaching 9 OSI units. These swings were evident both prior to and following cataract surgery if the patient was hyperosmolar but were not observed in the normal subjects, who exhibited uniformly calm traces over time. When expressed as peak-to-peak differences in OSI, the post-operative hyperosmolar cataract group showed an average fluctuation of 2.5±0.9 OSI units with a range of 1.8–5.0, and the normal osmolarity subjects averaged 1.4±0.4 OSI units with a range of 0.8–1.8, with the difference in variation being highly significant (p=0.002, two-tailed t-test). For reference, these transients approximated the expected light scatter observed in grade 2 (3.0±1.0 OSI) and grade 3 (6.0±2.0 OSI) cataracts.8
 |
Figure 1 Representative OSI traces of hyperosmolar (A) and normal (B) subjects prior to surgery at screening (blue circles), baseline (Orange triangles) and 90 days after surgery (gray squares). A = 329 mOsm/L, B = 300 mOsm/L. |
Of note, there were no significant differences in OSI variation when subjects were sorted by staining (≤ grade 1 stain = 0.47±0.22, > grade 1 stain = 0.52±.31, p=0.9), TBUT (<7 seconds = 0.49±0.30, ≥ 7 seconds = 0.54±0.18, p=0.7), number of symptoms (≤ 2 binary symptoms = 0.48±0.39, > 2 symptoms=0.52±0.13, p=0.7), severity of symptoms (< 5 = 0.52±0.32, ≥ 5 = 0.48±0.17, p=0.8) or MGD status (no MGD = 0.50±0.29, presence of MGD = 0.54±0.25, p=0.9). Statistical significance was not achieved at other relevant thresholds for the slit lamp signs and ocular surface disease symptom measurements. Figure 2 compares the classification of post-operative light scatter variation based on pre-operative osmolarity or pre-operative observations at the slit lamp. Significance in OSI variation survived Bonferroni adjustment when sorted by osmolarity (p=0.032).
 |
Figure 2 Post-operative light scatter variation based on classification by pre-operative osmolarity or pre-operative observations at the slit lamp. Note that low TBUT is a more severe sign of dry eye but showed less variation in light scatter in this cohort, emphasizing the lack of predictability of this parameter from a slit lamp examination. |
In subjects with hyperosmolar dry eye but without cataracts (Table 1), instillation of hypotonic 0.18% HA did not alter OSI at 5 minutes, but significant reductions in OSI of 28.8%, 38.5% and 36.7% (all p < 0.001) were observed at 10, 15 and 30 minutes (Figure 3). Representative scans demonstrating the reduction in light scatter after acutely lowering the osmolarity of the tear film are shown in Figure 4. In this cohort, large peak-to-peak (mean: 1.9±0.3 OSI, maximum: 4.2 OSI), high frequency (1–2 second) light scatter fluctuations were normalized 30 minutes following artificial tear instillation (peak-to-peak mean: 1.0±0.2 OSI, maximum: 2.0 OSI).
 |
Figure 3 Change from baseline in OSI expressed as a % of baseline for hyperosmolar subjects following instillation of hypotonic 0.18% sodium hyaluronate. Error bars are expressed as standard error. |
 |
Figure 4 Reduction in light scatter after acutely lowering the osmolarity of the tear film. The top row (A–C) shows three separate subjects at screening (blue circles) and baseline (Orange triangles), prior to the introduction of artificial tears. Hyperosmolar subjects showed elevated OSI along with considerable OSI variation over time at screening and baseline, indicating excessive light scatter and unstable vision. The bottom row (D–F) shows 20 second OSI traces from the same subjects at 5 minutes (green squares), 10 minutes (orange x’s), 15 minutes (gray diamonds) and 30 minutes (yellow open circles) following instillation of hypotonic 0.18% sodium hyaluronate. From 10 minutes onward, a striking reduction in OSI and OSI variation followed hypotonic HA instillation, demonstrating that the entirety of the aberrant light scatter – roughly equivalent to that of a grade 2 to 3 cataract, was due to the compromised, hyperosmolar tear film. |
Discussion
The healthy corneal epithelium features a network of glycocalyx-rich microplicae, that serve to hold onto water, provide boundary lubrication and create a smooth transition into the aqueous layer.9 When exposed to hyperosmolar conditions, epithelial cells begin to change their morphology and lose their microplicae.10 Increasing levels of hyperosmolarity on the ocular surface drive epithelial apoptosis through cytochrome c, caspase-3, JNK and ERK pathways.1,11 Excess salt thus results in desquamation, revealing the relatively hydrophobic12 glycocalyx- and microplicae-free cells beneath.10 Loss of microplicae has been observed directly from hyperosmolarity due to acute exposure keratopathy13 (an analogue for lowered blink rate due to screen use) as well as in animal models of androgen deficiency following orchiectomy14 (associated with the type of aging found in the cataract surgery population).15
Models of tear film evaporation suggest reductions in surface tension due to these altered epithelial cell phenotypes would generate strongly concentrated hyperosmolar spots in the tear film, with spikes in excess of 1,500 mOsm/L appearing after a few seconds of evaporation.16 Hyperosmolar hot spots prior to breakup are believed to be small, on the order of hundreds of microns in extent, falling rapidly to background osmolarity within a millimeter.16 As the refractive index of tears can change unpredictably with increasing osmolarity and protein concentration,17 the locally accelerated evaporation of tears within desquamated hot spots would unpredictably alter the optical properties of the tear lens. While bulk changes in optical properties of the cornea have been observed due to exposure to hyperosmolarity,18 the current study observed high temporal frequency variations in light scatter predicted by the high spatial frequency mechanism referenced above – the implications of which fundamentally alter our understanding of refractive outcomes in cataract surgery. CDVA, which is a time-averaged estimate of visual quality, does not sufficiently describe the time-varying second-order statistics of a hyperosmolar patient. Thus, even if a successful surgery has achieved target refraction, the presence of hyperosmolarity may introduce transient light scatter on the order of a grade 2–3 cataract.
Reducing tear osmolarity normalized light scatter and minimized its variation, confirming the hypothesis that the optical properties of the tear film are altered with increasing osmolarity. However, the timing and extent of the light scatter normalization was uncertain after instillation of artificial tears, likely due to variable blink rate, tear volume and mixing dynamics between subjects. As it is common for technicians to add artificial tears prior to pre-surgical biometry, it is therefore important to identify which patients are hyperosmolar prior to evaluation, given the variable time to normalization. The data in this study suggest that hyperosmolar patients had generally stabilized 15 minutes post-instillation. Biometry prior to equilibration will likely increase the chance for refractive errors in a hyperosmolar patient,3 since measurements will take place within a rapidly changing optical environment. It is not known how long the stabilization effect lasts from artificial tears, but light scatter was low and stable from 15 to 30 minutes following instillation in this study.
Prior studies have recognized the need to identify and treat dry eye prior to cataract surgery to achieve optimal outcomes,19,20 although challenges in objectively predicting patient satisfaction based on staining and TBUT have been reported.21,22 In this study, hyperosmolar patients exhibited significantly elevated variation in light scatter that was not recapitulated by staining or TBUT. Given the association between hyperosmolarity and poor outcomes in this and other studies,3,4,23,24 it may be prudent to incorporate osmolarity testing in pre-operative evaluations to identify patients that have an increased risk of post-operative light scatter variation, as these patients would not be identified by slit-lamp examination alone.
A limitation to this study was the relatively small study population. There was little overlap in the primary endpoint distribution and the sample size was sufficient given the observed effect size – suggesting that the optical effects are real. However, the population size did not allow the authors to consider questions about risk stratification by osmolarity level, for instance, and we could only conclude that increased risk of light scatter variation is related to presence of hyperosmolarity rather than the degree. Additionally, it would be interesting in future studies to appropriately power CDVA and patient satisfaction metrics when classified by osmolarity status. As these are more subjective parameters, larger cohorts would be necessary to evaluate the impact of hyperosmolarity. Another limitation is the lack of a normal OSI, normal osmolarity group exposed to artificial tears. The decision to omit this control group was driven by practical considerations, as the inclusion criteria would place normal subjects near the lower limit of quantification of the OSI instrumentation, and we did not expect to be able to observe a meaningful impact of artificial tears in such a cohort.
Conclusion
Subjects with tear film hyperosmolarity exhibited significantly increased variation in light scatter following cataract surgery that was undifferentiated by staining or TBUT. Addition of artificial tears can acutely eliminate much of the light scatter associated with hyperosmolarity, but requires at least 15 minutes to stabilize in a hyperosmolar cohort. Elevated osmolarity may be indicative of light scatter equivalent to that of a grade 2–3 cataract.
Acknowledgments
Funding support provided by Trukera Medical, 940 S. Kimball, Ste 100 Southlake, TX 76092. Sponsors assisted in study design, analysis, interpretation of data and in the writing of the report.
Disclosure
Benjamin Sullivan & Michael Berg: employment, equity, patents with Trukera Medical. Pablo Artal: grant support from Trukera Medical. Julie Schallhorn, Lisa Nijm, Darrel White: consultants for Trukera Medical. Julie Schallhorn also reports personal fees from Zeiss, Forsight V6, ViaLase, Elios, Journey 1, Novus Vision, JelliSee, and Neurotrigger, outside the submitted work. Lisa Nijm is also a consultant for TruKera Medical and Bausch and Lomb, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Luo L, Li DQ, Pflugfelder SC. Hyperosmolarity-induced apoptosis in human corneal epithelial cells is mediated by cytochrome C and MAPK pathways. Cornea. 2007;26(4):452–460. doi:10.1097/ICO.0b013e318030d259
2. Huet E, Vallée B, Delbé J, et al. EMMPRIN modulates epithelial barrier function through a MMP-mediated occludin cleavage: implications in dry eye disease. Am J Pathol. 2011;179(3):1278–1286. PMID: 21777561; PMCID: PMC3157190. doi:10.1016/j.ajpath.2011.05.036
3. Epitropoulos AT, Matossian C, Berdy GJ, Malhotra RP, Potvin R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672–1677. PMID: 26432124. doi:10.1016/j.jcrs.2015.01.016
4. Kursite A, Laganovska G. Effect of tear osmolarity on postoperative refractive error after cataract surgery. J Ophthalmol. 2023. doi:10.31288/oftalmolzh202321115
5. Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–650. PMID: 14508260. doi:10.1097/00003226-200310000-00008
6. Chylack LT, Wolfe JK, Singer DM, et al. The lens opacities classification system III. the longitudinal study of cataract study group. Arch Ophthalmol. 1993;111(6):831–836. PMID: 8512486. doi:10.1001/archopht.1993.01090060119035
7. Lemp MA, Bron AJ, Baudouin C, et al. Tear osmolarity in the diagnosis and management of dry eye disease. Am J Ophthalmol. 2011;151(5):792–798.e1. PMID: 21310379. doi:10.1016/j.ajo.2010.10.032
8. Artal P, Benito A, Pérez GM, et al. An objective scatter index based on double-pass retinal images of a point source to classify cataracts. PLoS One. 2011;6(2):e16823. PMID: 21326868; PMCID: PMC3033912. doi:10.1371/journal.pone.0016823
9. Andrews PM. Microplicae: characteristic ridge-like folds of the plasmalemma. J Cell Biol. 1976;68(3):420–429. PMID: 828906; PMCID: PMC2109650. doi:10.1083/jcb.68.3.420
10. Gilbard JP. Tear film osmolarity and keratoconjunctivitis sicca. CLAO J. 1985;11(3):243–250. PMID: 4042314.
11. Chen Z, Tong L, Li Z, et al. Hyperosmolarity-induced cornification of human corneal epithelial cells is regulated by JNK MAPK. Invest Ophthalmol Vis Sci. 2008;49(2):539–549. PMID: 18234997. doi:10.1167/iovs.07-0569
12. Iwata S, Lemp MA, Holly FJ, Dohlman CH. Evaporation rate of water from the precorneal tear film and cornea in the rabbit. Invest Ophthalmol. 1969;8(6):613–619. PMID: 5359578.
13. Lai CT, Yao WC, Lin SY, et al. Changes of ocular surface and the inflammatory response in a rabbit model of short-term exposure keratopathy. PLoS One. 2015;10(9):e0137186. PMID: 26334533; PMCID: PMC4559311. doi:10.1371/journal.pone.0137186
14. Li L, Kang Q, Wang S, Zheng X. Effects of androgen on ultrastructure of corneal epithelium and function of the tear film in BALB/c mice. Cornea. 2015;34(3):334–341. PMID: 25532998. doi:10.1097/ICO.0000000000000292
15. Sullivan DA, Sullivan BD, Evans JE, et al. Androgen deficiency, Meibomian gland dysfunction, and evaporative dry eye. Ann N Y Acad Sci. 2002;966(1):211–222. PMID: 12114274. doi:10.1111/j.1749-6632.2002.tb04217.x
16. Peng CC, Cerretani C, Braun RJ, Radke CJ. Evaporation-driven instability of the precorneal tear film. Adv Colloid Interface Sci. 2014;206:250–264. PMID: 23842140. doi:10.1016/j.cis.2013.06.001
17. Craig JP, Simmons PA, Patel S, Tomlinson A. Refractive index and osmolality of human tears. Optom Vis Sci. 1995;72(10):718–724. PMID: 8570161. doi:10.1097/00006324-199510000-00004
18. Deinema LA, Vingrys AJ, Chinnery HR, Downie LE. Optical coherence tomography reveals changes to corneal reflectivity and thickness in individuals with tear hyperosmolarity. Transl Vis Sci Technol. 2017;6(3):6. PMID: 28553560; PMCID: PMC5444496. doi:10.1167/tvst.6.3.6
19. Schallhorn SC, Hettinger KA, Teenan D, Venter JA, Hannan SJ, Schallhorn JM. Predictors of patient satisfaction after refractive lens exchange with an extended depth of focus IOL. J Refract Surg. 2020;36(3):175–184. PMID: 32159822. doi:10.3928/1081597X-20200211-01
20. Donaldson K, Parkhurst G, Saenz B, Whitley W, Williamson B, Hovanesian J. Call to action: treating dry eye disease and setting the foundation for successful surgery. J Cataract Refract Surg. 2022;48(5):623–629. PMID: 34694257; PMCID: PMC9018211. doi:10.1097/j.jcrs.0000000000000844
21. Szakáts I, Sebestyén M, Tóth É, Purebl G. Dry eye symptoms, patient-reported visual functioning, and health anxiety influencing patient satisfaction after cataract surgery. Curr Eye Res. 2017;42(6):832–836. PMID: 28129000. doi:10.1080/02713683.2016.1262429
22. Siew L, Tong L. The effect of past cataract surgery within the medium to long-term period on patients with dry eye disease. J Clin Med. 2022;11(4):972. PMID: 35207244; PMCID: PMC8878219. doi:10.3390/jcm11040972
23. Igarashi T, Takahashi H, Kobayashi M, et al. Changes in tear osmolarity after cataract surgery. J Nippon Med Sch. 2021;88(3):204–208. PMID: 34193743. doi:10.1272/jnms.JNMS.2021_88-405
24. González-Mesa A, Moreno-Arrones JP, Ferrari D, Teus MA. Role of tear osmolarity in dry eye symptoms after cataract surgery. Am J Ophthalmol. 2016;170:128–132. PMID: 27521606. doi:10.1016/j.ajo.2016.08.002
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prospective Randomized Single-Masked Study of Bilateral Isofocal Optic-Design or Monofocal Intraocular Lenses
Ang RET, Stodulka P, Poyales F
Clinical Ophthalmology 2023, 17:2231-2242
Published Date: 4 August 2023
The Effects of Low Viscosity Preservative-Free Chloroprocaine Ophthalmic Gel 3% versus BAK-Containing Tetracaine 0.5% on the Bactericidal Action of Povidone-Iodine
Ilyas H, Costine R
Clinical Ophthalmology 2024, 18:825-831
Published Date: 13 March 2024