")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
The Association Between Life’s Essential 8 and Psoriasis in American Adults: A Cross-Sectional NHANES Study
Authors Zhang W, Yuan Z, Wang Y , Jin Z, Luo Z , Wang X
Received 2 July 2024
Accepted for publication 4 November 2024
Published 12 November 2024 Volume 2024:17 Pages 2555—2563
DOI https://doi.org/10.2147/CCID.S476594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Weiqing Zhang,1,* Zengze Yuan,1,* Yihan Wang,1 Zhaokai Jin,2 Ziyue Luo,1 Xinchang Wang1
1The Second Affiliated Hospital of Zhejiang Chinese Medical University (Xinhua Hospital of Zhejiang Province), Hangzhou, Zhejiang, People’s Republic of China; 2The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinchang Wang, Email [email protected]
Purpose: Life’s Essentials 8 (LE8) is a new indicator developed by the American Heart Association to assess cardiovascular health, including diet, physical activity, nicotine exposure, sleep health, body mass index, blood lipids, blood glucose and blood pressure. And more and more studies have shown that this index can evaluate other diseases, such as chronic kidney disease, abdominal aortic calcification and so on. However, there is no relevant study to evaluate the association between LE8 and psoriasis. The purpose of this study was to investigate the relationship between LE8 and the prevalence of psoriasis in American adults.
Patients and Methods: The data are from the National Health and Nutrition Examination Survey (NHANES) of the United States from 2003 to 2006, 2009 to 2014. Psoriasis was the dependent variable. LE8 is an independent variable and is divided into three levels: high, medium and low. Multivariate logistic regression model was used to explore the relationship between LE8 and psoriasis.
Results: A total of 13430 people were included in this study, including 391 patients with psoriasis and 13039 patients without psoriasis. The prevalence of psoriasis was 2.91%. In the fully adjusted logistic regression model, LE8 score was negatively correlated with psoriasis (OR=0.99; 95% CI, 0.98– 0.99, P=0.0003). And this result still exists when LE8 is divided into high, medium and low groups. Compared with the low LE8 group, the high LE8 group had a 61% lower risk of psoriasis (OR=0.39; 95% CI, 0.26– 0.57, p < 0.0001).
Conclusion: This cross-sectional study suggested that LE8 score was negatively correlated with psoriasis risk.
Keywords: Life’s Essentials 8, NHANES, Cross-sectional study, Psoriasis
Introduction
Psoriasis is a chronic inflammatory skin disease that affects around 2–3% of the global population.1 Psoriasis is characterized by well-defined erythematous patches covered with silvery white scales, which typically occur symmetrically on the elbows, knees, trunk, and scalp, and can cause significant physiological and psychological issues for patients.2 Moreover, there is an increasing awareness that psoriasis is not solely a skin disease but also linked to systemic conditions such as Crohn’s disease, diabetes (especially type 2 diabetes), metabolic syndrome, depression, and cardiovascular disease.3–6 It is evident that psoriasis poses a significant public health burden.
In 2010, the American Heart Association introduced Life’s Simple 7 (LE7), an indicator for assessing cardiovascular health. This initiative aims to shift the focus from solely treating diseases to promoting and safeguarding positive health in both the general population and individuals.7 Later, it was updated to Life’s Essentials 8 (LE8) in July 2022. Compared to LE7, LE8 includes sleep indicators and updates other scoring algorithms.8 LE8 was initially used as an indicator to evaluate cardiovascular health, and the LE8 score is positively correlated with the degree of cardiovascular health.9 Some scholars have also found that it is applicable as an indicator for other diseases. For example, Zongao Cai et al found a negative correlation between the LE8 score and the risk of abdominal aortic calcification in elderly individuals in the United States.10 Yuqing Ren et al discovered a nonlinear negative correlation between LE8 and the prevalence of chronic kidney disease.11 However, LE8 has not been utilized to assess the risk of psoriasis. Therefore, in this study, we investigated the relationship between LE8 and psoriasis to address this knowledge gap.
Materials and Methods
Data Source
The NHANES, a publicly accessible database in the United States, served as the data source for this study. The NHANES database contains information on demographics, diet, exams, lab tests, and questionnaires, as well as restricted data. Access to restricted data requires the submission of an application. The ethics review committee of the National Research Center for Health Statistics approved the method of the study because all participants provided written permission at the beginning of recruitment.
Study Participants
We combined NHANES cycles from 2003–2004, 2005–2006, 2009–2010, 2011–2012, and 2013–2014, as these are the only cycles containing information about psoriasis, for subsequent analysis. The exclusion criteria included: (1) lack of psoriasis information; (2) incomplete LE8 score (missing any of the four health behaviors or four health factors); and (3) missing data for other covariates. A total of 13,430 participants were included in the analysis. (Figure 1).
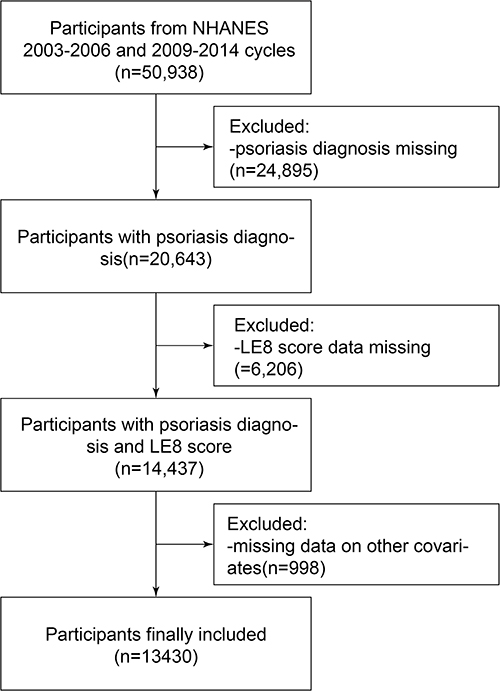 |
Figure 1 Flow chart of participant selection. |
Definition of LE8
The LE8 scoring algorithm comprises four health behaviors (diet, physical activity, nicotine exposure, and sleep duration) and four health factors (body mass index [BMI], non-high-density-lipoprotein cholesterol, blood glucose, and blood pressure). Each indicator is scored on a scale from 0 to 100 points, reflecting its contribution to overall cardiovascular health.9 Diet indicators were assessed using the Healthy Eating Index 2015. Questionnaire data were used to collect information on physical activity, nicotine exposure, sleep duration, and diabetes status. Laboratory data provided information on blood lipids and blood glucose levels, while blood pressure, height, and weight measurements were taken at the mobile examination center. The detailed algorithm to calculate the LE8 scores for the indicators in the NHANES data has been published previously (Table S1), in which each of the 8 indicators was scored on a scale ranging from 0 to 100, and the total LE8 score was calculated as an unweighted average of the 8 indicators.9
Definition of Psoriasis
Psoriasis was diagnosed by professional physicians through pattern recognition, which involved careful morphological assessment of the skin lesions.12 The classic description of psoriasis includes well-defined erythematous patches covered with silvery scales. Information was collected using an interviewer-assisted questionnaire. Participants were asked, “Have you ever been told by a health care provider that you had psoriasis?” In our study, participants who answered affirmatively were classified as having psoriasis, while those who refused to answer or indicated that they did not know were excluded.
Covariates
Based on previous literature, the following covariates were selected: age at interview, sex (male, female), race/ethnicity (Mexican American, Other Hispanic, non-Hispanic white, non-Hispanic black, other race/multiracial), family Poverty Income Ratio (PIR) (<1.30, 1.30–3.50, >3.50), education levels (Less than high school, High School Grad or Equivalent, More than high school), marital status (divorced/separated/widowed, Married/living with a partner, never married), and cardiovascular disease (yes, no). A positive response to any of the following statements was considered indicative of cardiovascular disease: “ever told you had congestive heart failure”, “ever told you had coronary heart disease”, “ever told you had angina/angina pectoris”, “ever told you had a heart attack”, or “ever told you had a stroke”.13
Statistical Analysis
Data merging was performed using EmpowerStats (version 2.0) and the statistical software package R (version 4.1.3), while images in this paper were created using Adobe Illustrator (version 2021). Categorical variables were expressed as percentages, while continuous variables were expressed as standard deviations. While sampling weights are typically used to produce representative and unbiased statistics in the analysis of a complex survey, they could also reduce the precision of the estimates. Additionally, sampling weights could introduce a degree of over-adjustment bias.14–16 Thus, we conducted the analysis without incorporating sampling weights, consistent with some previous research using NHANES data.14–16 The chi-square test and Kruskal–Wallis test were used to assess significant differences between psoriasis patients and non-psoriasis patients. Multivariate logistic regression models were initially used to evaluate the independent association between LE8 and psoriasis. In this study, Model I was unadjusted for covariates, Model II was adjusted only for sex, age, and race, and Model III was adjusted for PIR, education level, marital status, and cardiovascular disease based on Model II. The dose-response association between Life’s Essential 8 and psoriasis was then assessed using smooth curve fitting. Subgroup analysis and interaction tests were performed to assess the effect of confounders on the relationship between Life’s Essential 8 and psoriasis. Statistical significance was defined as a p-value below 0.05.
Result
Baseline Characteristics of Participants
Baseline characteristics of the 13,430 subjects included in this study showed that 48.65% were males and 51.35% were females. The overall prevalence of psoriasis in the study population was 2.91%. Patients with psoriasis had a higher average age (47.33 ± 17.03 years), a higher proportion of non-Hispanic white individuals (61.64%), and a higher prevalence of cardiovascular disease (15.09%) compared to those without psoriasis, which are consistent with previous research findings.17 Furthermore, the LE8 score was significantly higher in psoriasis patients compared to non-psoriasis patients. (Table 1).
 |
Table 1 Baseline Characteristics of Participants (N=13430) |
The Association Between LE8 and Psoriasis
The results indicated that the risk of psoriasis decreased with an increase in the LE8 score (Table 2). Model I (OR=0.99; 95% CI, 0.98–0.99, p<0.001) and model II (OR=0.99; 95% CI, 0.98–0.99, p<0.001) showed significant correlation. In model III, the relationship between LE8 score and psoriasis was consistent (OR=0.99; 95% CI, 0.98–0.99, p=0.0003). Furthermore, converting the LE8 score from a continuous variable to a categorical variable revealed more significant results. Participants in the fully adjusted highest group had a 61% (OR=0.39; 95% CI, 0.26–0.57, p <0.0001) lower risk of psoriasis compared to those in the lowest group. The risk of psoriasis in the moderate group was significantly lower than that in the lowest group (OR=0.65;95% CI, 0.49–0.79, p=0.0002). Additionally, smooth curve fitting was used to assess the relationship between the LE8 score and psoriasis, revealing a negative correlation in this study, as depicted in Figure 2.
 |
Table 2 Association Between LE8 and Psoriasis in Different Models |
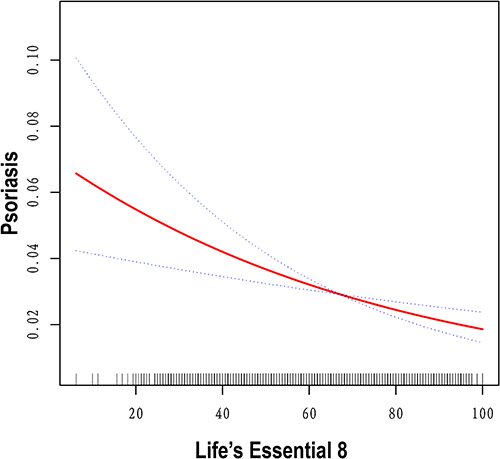 |
Figure 2 Dose-response relationship between LE8 and psoriasis. A nonlinear association between LE8 and psoriasis was identified using a generalized additive model. The solid red line represents the smooth curve fit between the variables, while the blue bands represent the 95% confidence interval from the fit. All analyses were adjusted for sex, age, race, PIR, education level, marital status, and cardiovascular disease. |
Subgroup Analysis
In order to further explore the role of confounding factors in the association between the LE8 score and psoriasis, participants were divided into subgroups based on cardiovascular diseases, gender, age, race, education level, marital status, and poverty ratio (Table 3). A statistically significant association was observed only in elderly men of other Hispanic or other race/multiracial race, with education beyond high school, middle income, no cardiovascular disease, and a partner (all p<0.05). However, we did not find any significant interaction between the LE8 score and these potential confounders (all P values of interaction>0.05).
 |
Table 3 Subgroup Analysis for the Association Between LE8 and Psoriasis |
Discussion
This cross-sectional study is the first to investigate the association between the LE8 score and the risk of psoriasis in a large, nationally representative sample. The cross-sectional survey revealed a negative correlation between the LE8 score and the likelihood of psoriasis. A higher LE8 score was associated with a lower probability of psoriasis.
The LE8 score was initially developed to assess cardiovascular health, and its role in assessing the relationship between cardiovascular diseases appears to be well-established.18,19 It is worth mentioning that in recent years, the LE8 score has become increasingly widely used in clinical settings. Some scholars have found that the LE8 score is associated with abdominal aortic calcification and nonalcoholic fatty liver disease.10,20 However, there are no reports on the relationship between LE8 and psoriasis. Therefore, there is no reason not to explore this relationship. We will explore the relevant reasons from the following aspects.
Firstly, the LE8 score includes four healthy behaviors: diet, physical activity, nicotine exposure, and sleep health. Regarding diet, a study from the French NutriNet-Santé cohort indicated a negative correlation between the Mediterranean diet and the severity of psoriasis.21 Furthermore, in mouse experiments, the Western diet was found to activate the interleukin-23 (IL-23) signaling pathway, thereby increasing IL-23-stimulated γδ IL-17A production in T cells, which is essential for skin inflammation development.22,23 Additionally, IL-23 overexpression resulted in reduced microbial diversity and significant dysbiosis in mice fed a Western diet.24 Interestingly, switching from the Western diet to the standard diet after IL-23 release led to a decrease in skin inflammation and partial reversal of intestinal microbiota.24 Moreover, Frankel et al discovered that engaging in at least 20.9 MET-hours (equivalent to 105 minutes of running or 180 minutes of swimming or playing tennis) of vigorous exercise per week reduced the risk of psoriasis by 25–30% compared to not engaging in any vigorous exercise.25 Furthermore, skin lesions are the primary pathological changes in psoriasis, causing itching that typically worsens at night due to reduced sensory thresholds, leading to sleep disturbances.26,27 This contributes significantly to poor sleep quality in patients with psoriasis. Interestingly, insufficient sleep may also promote the development of psoriasis. Wen Qing Li et al found that the hazard ratio for psoriasis among night shift workers during a 10-year follow-up period was 1.23.28 Furthermore, smoking is a recognized risk factor for psoriasis. Eun Joo Lee et al demonstrated a positive correlation between the amount of smoking and/or smoking duration and the occurrence of psoriasis.29
Additionally, the LE8 score includes four health factors: body mass index, blood lipids, blood glucose, and blood pressure. Obesity is a well-established risk factor for psoriasis. Mechanistic research suggests that this association may be attributed to obesity and endoplasmic reticulum stress in adipocytes, which increase the production of proinflammatory cytokines in adipose tissue. These cytokines enter the bloodstream, triggering inflammation in various tissues, including the skin, and consequently, inducing the development of psoriasis.30 Metabolic syndrome is characterized by a cluster of conditions including obesity, blood pressure abnormalities, dyslipidemia, and blood glucose abnormalities, all of which have been reported to be associated with psoriasis.31–33 These findings substantially contribute to understanding the role of LE8 in the development of psoriasis.
Overall, the components of the LE8 score are closely associated with the risk of psoriasis. Thus, using the LE8 score to assess psoriasis is meaningful. Additionally, the LE8 score can serve as a reminder for individuals, particularly those at high risk of psoriasis, to maintain a healthy lifestyle. Our study findings could offer valuable guidance for managing and preventing the risk of psoriasis.
Our study has several notable strengths. Firstly, the data for this study are from the NHANES database, which is representative, publicly available, free, and easy to access. Secondly, we comprehensively evaluated the direct impact of the LE8 score on psoriasis, filling a gap in previous studies. However, the study also has some limitations. Firstly, causality cannot be determined in cross-sectional studies. Secondly, the diagnosis of psoriasis is based on a self-reported questionnaire, which introduces the possibility of recall bias. Thirdly, the NHANES database only contains data from Americans and may not represent the demographic data of other countries. Finally, we cannot draw direct conclusions from the research results, and further prospective studies are needed to confirm these findings.
Conclusion
The LE8 score was negatively correlated with the prevalence of psoriasis in adults. The results emphasize that LE8 can be applied to clinical practice, help patients and the general population to identify the risk of psoriasis as soon as possible, and minimize the disease burden. The causal relationship and exact mechanism between LE8 and psoriasis should be further explored in the future.
Abbreviations
LE8, Life’s Essential 8; LE7, Life’s Simple 7; OR, odds ratio; CI, confidence interval; PIR, Poverty Income Ratio.
Ethical Approval and Consent to Participate
These studies involving humans have been approved by the Ethics Review Committee of the National Center for Health Statistics. These studies were conducted based on local legislation and institutional requirements. According to national legislation and institutional requirements, participants or their legal guardians/close relatives do not require written informed consent. For detailed information, please visit https://www.cdc.gov/nchs/Nhanes/irba98.htm. In addition, in China, the National Health Commission, the Ministry of education, the Ministry of science and technology and the State Administration of traditional Chinese Medicine published the “life science and medical research involving human beings” in February 2023, which stipulates that “under the premise of using human information data or biological samples, causing no harm to human beings, and not involving sensitive personal information or commercial interests”, some cases of life science and medical research involving human beings can be exempted from ethical review. Our research is about the NHANES database and does not involve sensitive personal information or commercial interests, therefore our research is exempt from ethical approval.
Acknowledgments
We thank the staff of the CDC National Center for health statistics for designing, collecting, managing NHANES data and publishing data for public use. We thank all the research participants for their cooperation.
Disclosure
Weiqing Zhang and Zengze Yuan contributed equally to this work and share first authorship. All authors declare no conflicts of interest in this work.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
2. Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263–271. doi:10.1016/S0140-6736(07)61128-3
3. Esposito M, Saraceno R, Giunta A, Maccarone M, Chimenti S. An Italian study on psoriasis and depression. Dermatology. 2006;212(2):123–127. doi:10.1159/000090652
4. Sommer DM, Jenisch S, Suchan M, Christophers E, Weichenthal M. Increased prevalence of the metabolic syndrome in patients with moderate to severe psoriasis. Arch Dermatol Res. 2006;298(7):321–328. doi:10.1007/s00403-006-0703-z
5. Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB, Gelfand JM. Prevalence of cardiovascular risk factors in patients with psoriasis. J Am Acad Dermatol. 2006;55(5):829–835. doi:10.1016/j.jaad.2006.08.040
6. Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol. 1995;32(6):982–986. doi:10.1016/0190-9622(95)91336-X
7. Lloyd-Jones DM, Hong Y, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through. 2020 and beyond. Circulation. 2010;121(4):586–613. doi:10.1161/CIRCULATIONAHA.109.192703
8. Ioachimescu OC. From seven sweethearts to life begins at eight thirty: a journey from life’s simple 7 to life’s essential 8 and beyond. J Am Heart Assoc. 2022;11(21):e027658. doi:10.1161/JAHA.122.027658
9. Lloyd-Jones DM, Allen NB, Anderson CAM, et al. Life’s essential 8: updating and enhancing the American Heart Association’s construct of cardiovascular health: a Presidential Advisory From the American Heart Association. Circulation. 2022;146(5):e18–e43. doi:10.1161/CIR.0000000000001078
10. Cai Z, Liu Z, Zhang Y, et al. Associations between life’s essential 8 and abdominal aortic calcification among middle-aged and elderly populations. J Am Heart Assoc. 2023;12(24):e031146. doi:10.1161/JAHA.123.031146
11. Ren Y, Cai Z, Guo C, et al. Associations between life’s essential 8 and chronic kidney disease. J Am Heart Assoc. 2023;12(24):e030564. doi:10.1161/JAHA.123.030564
12. Raychaudhuri SK, Maverakis E, Raychaudhuri SP. Diagnosis and classification of psoriasis. Autoimmun Rev. 2014;13(4–5):490–495. doi:10.1016/j.autrev.2014.01.008
13. Dang K, Wang X, Hu J, et al. The association between triglyceride-glucose index and its combination with obesity indicators and cardiovascular disease: NHANES 2003–2018. Cardiovasc Diabetol. 2024;23(1):8. doi:10.1186/s12933-023-02115-9
14. Zhang Y, Dong T, Hu W, et al. Association between exposure to a mixture of phenols, pesticides, and phthalates and obesity: comparison of three statistical models. Environ Int. 2019;123:325–336. doi:10.1016/j.envint.2018.11.076
15. Kim S, Kim S, Won S, Choi K. Considering common sources of exposure in association studies - Urinary benzophenone-3 and DEHP metabolites are associated with altered thyroid hormone balance in the NHANES 2007–2008. Environ Int. 2017;107:25–32. doi:10.1016/j.envint.2017.06.013
16. Blount BC, Pirkle JL, Osterloh JD, Valentin-Blasini L, Caldwell KL. Urinary perchlorate and thyroid hormone levels in adolescent and adult men and women living in the United States. Environ Health Perspect. 2006;114(12):1865–1871. doi:10.1289/ehp.9466
17. Kamiya K, Kishimoto M, Sugai J, Komine M, Ohtsuki M. Risk factors for the development of psoriasis. Int J Mol Sci. 2019;20(18):4347. doi:10.3390/ijms20184347
18. Petermann-Rocha F, Deo S, Celis-Morales C, et al. An opportunity for prevention: associations between the life’s essential 8 score and cardiovascular incidence using prospective data from UK biobank. Curr Probl Cardiol. 2023;48(4):101540. doi:10.1016/j.cpcardiol.2022.101540
19. Sun J, Li Y, Zhao M, et al. Association of the American Heart Association’s new “Life’s Essential 8” with all-cause and cardiovascular disease-specific mortality: prospective cohort study. BMC Med. 2023;21(1):116. doi:10.1186/s12916-023-02824-8
20. Wang L, Yi J, Guo X, Ren X. Associations between life’s essential 8 and non-alcoholic fatty liver disease among US adults. J Transl Med. 2022;20(1):616. doi:10.1186/s12967-022-03839-0
21. Phan C, Touvier M, Kesse-Guyot E, et al. Association between Mediterranean anti-inflammatory dietary profile and severity of psoriasis: results from the nutrinet-santé cohort. JAMA Dermatol. 2018;154(9):1017–1024. doi:10.1001/jamadermatol.2018.2127
22. Mabuchi T, Takekoshi T, Hwang ST. Epidermal CCR6+ γδ T cells are major producers of IL-22 and IL-17 in a murine model of psoriasiform dermatitis. J Immunol. 2011;187(10):5026–5031. doi:10.4049/jimmunol.1101817
23. Shi Z, Wu X, Yu S, et al. Short-term exposure to a western diet induces psoriasiform dermatitis by promoting accumulation of IL-17A-producing γδ T cells. J Invest Dermatol. 2020;140(9):1815–1823. doi:10.1016/j.jid.2020.01.020
24. Shi Z, Wu X, Santos Rocha C, et al. Short-term western diet intake promotes IL-23‒mediated skin and joint inflammation accompanied by changes to the gut microbiota in mice. J Invest Dermatol. 2021;141(7):1780–1791. doi:10.1016/j.jid.2020.11.032
25. Frankel HC, Han J, Li T, Qureshi AA. The association between physical activity and the risk of incident psoriasis. Arch Dermatol. 2012;148(8):918–924. doi:10.1001/archdermatol.2012.943
26. Smolensky MH, Portaluppi F, Manfredini R, et al. Diurnal and twenty-four hour patterning of human diseases: acute and chronic common and uncommon medical conditions. Sleep Med Rev. 2015;21:12–22. doi:10.1016/j.smrv.2014.06.005
27. Spindler M, Przybyłowicz K, Hawro M, et al. Sleep disturbance in adult dermatologic patients: a cross-sectional study on prevalence, burden, and associated factors. J Am Acad Dermatol. 2021;85(4):910–922. doi:10.1016/j.jaad.2021.04.015
28. Li W-Q, Qureshi AA, Schernhammer ES, Han J. Rotating night-shift work and risk of psoriasis in US women. J Invest Dermatol. 2013;133(2):565–567. doi:10.1038/jid.2012.285
29. Lee EJ, Han KD, Han JH, Lee JH. Smoking and risk of psoriasis: a nationwide cohort study. J Am Acad Dermatol. 2017;77(3):573–575. doi:10.1016/j.jaad.2017.04.015
30. Cooper PO, Haas MR, Noonepalle SKR, Shook BA. Dermal drivers of injury-induced inflammation: contribution of adipocytes and fibroblasts. Int J Mol Sci. 2021;22(4). doi:10.3390/ijms22041933
31. Snekvik I, Nilsen TIL, Romundstad PR, Saunes M. Metabolic syndrome and risk of incident psoriasis: prospective data from the HUNT Study, Norway. Br J Dermatol. 2019;180(1):94–99. doi:10.1111/bjd.16885
32. Zhou Y, Han L, Wang Z, et al. Bioinformatic analysis of the potential common pathogenic mechanisms for psoriasis and metabolic syndrome. Inflammation. 2023;46(4):1381–1395. doi:10.1007/s10753-023-01815-4
33. Armstrong AW, Harskamp CT, Armstrong EJ. Psoriasis and metabolic syndrome: a systematic review and meta-analysis of observational studies. J Am Acad Dermatol. 2013;68(4):654–662. doi:10.1016/j.jaad.2012.08.015
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anxiety and Depression in People with Eczema or Psoriasis: A Comparison of Associations in UK Biobank and Linked Primary Care Data
Matthewman J, Mansfield KE, Hayes JF, Adesanya EI, Smith CH, Roberts A, Langan SM, Henderson AD
Clinical Epidemiology 2023, 15:891-899
Published Date: 7 August 2023
Association of Complete Blood Cell Count-Derived Inflammatory Biomarkers with Psoriasis and Mortality
Zhao Y, Yang XT, Bai YP, Li LF
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3267-3278
Published Date: 13 November 2023
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Association Between Triglyceride Glucose Index and Infertility in Reproductive-Aged Women: A Cross-Sectional Study
Zhuang J, Wang S, Wang Y, Hu R, Wu Y
International Journal of Women's Health 2024, 16:937-946
Published Date: 27 May 2024
Association Between Weight-Adjusted Waist Index and Cognitive Function in Older Adults Without Diabetes: A Cross-Sectional Study
Wang Q, Yin Y, Liu W, Li L, Wang Z, Tian Y, Fan J
Clinical Interventions in Aging 2025, 20:69-79
Published Date: 25 January 2025