")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
The Association Between Periodontitis and the Prevalence and Prognosis of Metabolic Syndrome
Authors Li T , Wu H, Fu Z, Li H, Li Q, Liu Y, Zhang Q
Received 8 November 2024
Accepted for publication 20 January 2025
Published 21 February 2025 Volume 2025:18 Pages 1053—1065
DOI https://doi.org/10.2147/JMDH.S499516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Tao Li, Huadong Wu, Zhenzhen Fu, Hong Li, Quan Li, Yi Liu, Qiang Zhang
Department of Oral and Maxillofacial Surgery, The First Affiliated Hospital, Jiangxi Medical College, Nanchang University, Jiangxi, People’s Republic of China
Correspondence: Qiang Zhang, Department of Oral and Maxillofacial Surgery, The First Affiliated Hospital, Jiangxi Medical College, Nanchang University, Jiangxi, People’s Republic of China, Email [email protected]
Objective: Periodontitis and metabolic syndrome (MetS) are both linked to inflammation, but their association remains unclear. This study aimed to explore the association between periodontitis and MetS prevalence and evaluate its impact on the prognosis of all-cause and cardiovascular mortality in MetS.
Methods: Data were obtained from the National Health and Nutrition Examination Survey (NHANES) database. Logistic regression analysis was used to investigate the association between periodontitis and the prevalence of MetS, while Cox regression analysis was applied to assess the association between periodontal status and the poor prognosis in individuals with MetS. Furthermore, restricted cubic spline (RCS) analysis was performed to evaluate the linear and nonlinear associations between periodontal parameters, including attachment loss (AL) and probing depth (PD), and the prevalence and mortality of MetS.
Results: A total of 9,270 individuals were included in the analysis. Individuals with periodontitis had a higher prevalence of MetS compared to those without periodontitis (OR=1.24, 95% CI: 1.08– 1.43). Cox regression analysis revealed that periodontitis was associated with an increased risk of all-cause mortality (HR=2.03, 95% CI:1.40– 2.92) and cardiovascular mortality (HR=2.32, 95% CI:1.05– 5.10) among individuals with MetS. Furthermore, the RCS analysis demonstrated that AL had a nonlinear association with the risk of prevalence, all-cause mortality and cardiovascular mortality in MetS (P for nonlinearity < 0.05). However, PD was linearly associated with the increased risks of these outcomes (P overall < 0.05).
Conclusion: Periodontitis is associated with an increased risk of MetS, as well as higher risks of all-cause and cardiovascular mortality.
Keywords: MetS, periodontitis, NHANES
Introduction
Metabolic syndrome (MetS) comprises a cluster of risk factors such as obesity, dyslipidemia, hypertension, insulin resistance, and hyperglycemia.1 It is estimated around 40% of people over 60 years old meet the diagnostic criteria of MetS in the United States.2 There are several studies have reported that MetS is related to a higher risk of cardiovascular disease, cerebrovascular disease, and diabetes.2–5 Given the substantial influence of MetS on human health, early detection and intervention strategies for MetS are key topics of discussion among researchers in related fields.
People with oral diseases are prone to metabolic disorders.6 Periodontitis, a common oral disease, is typically triggered by ecologically dysfunctional changes in the microbiota, eventually resulting in the loss of periodontal attachments.7,8 According to large-scale epidemiological studies, as many as half of the world’s adults suffer from periodontal disease, with 10.5–12.0% at risk of severe periodontitis.9 In addition, individuals with periodontitis have higher serum levels of proinflammatory cytokines than non-periodontitis. Consequently, periodontitis is related to several chronic diseases, including aspiration pneumonia and cardiovascular disease.10
Periodontal disease and MetS exhibit pro-inflammatory and immune response effects, with shared inflammatory mediators such as C-reactive protein, prostaglandin E2, interleukin-1β, and tumor necrosis factor-α. Studies have indicated that the pathological processes of these two conditions involve common inflammatory signaling pathways, dysregulated adipokine production, exacerbated oxidative stress, and disrupted matrix remodeling. These interconnected mechanisms link localized periodontal inflammation to systemic metabolic dysregulation and adverse cardiovascular outcomes.11 Furthermore, a bidirectional relationship has been observed between periodontal disease and metabolic syndrome (MetS), potentially linked to systemic inflammation triggered by periodontal infections. Persistent chronic inflammation may contribute to the development of insulin resistance, disrupt lipid metabolism, and accelerate the progression of MetS.12
Although previous research has evaluated the impact of periodontitis on MetS. However, the definitions for periodontitis and MetS varied significantly, resulting in considerable heterogeneity in these studies. Furthermore, there have been no studies on the association between periodontitis and MetS mortality. The National Health and Nutrition Examination Survey (NHANES) database is an invaluable resource that not only provides detailed information on the diagnosis of periodontitis and metabolic syndrome but also includes follow-up survival data for each participant. Therefore, we investigated the impact of periodontitis on prognosis and the prevalence of MetS in individuals through NHANES.
Materials and Methods
Research Design and Data Sources
The NHANES database is a publicly available database reviewed and approved by the National Center for Health Statistics (NCHS). As displayed in Figure 1, 30468 individuals were included from the NHANES 2009–2014 cycles. Among these individuals, those with missing variable data were excluded, and 9,270 individuals to assess the impact of periodontitis on the prevalence of MetS. Meanwhile, 3,301 were included in the investigation of the impact of periodontitis on its mortality.
 |
Figure 1 The flowchart of this study. Abbreviations: NHANES, the National Health and Nutrition Examination Survey; MetS, metabolic syndrome. |
Definition for Periodontitis
Periodontitis was diagnosed based on the categorization system developed by the American Academy of Periodontology and the Centers for Disease Control and Prevention (CDC-AAP).13 Individuals identified with mild, moderate, or severe periodontitis were categorized into the periodontitis group, whereas those without a periodontitis diagnosis were placed in the non-periodontitis group in this study. In addition, we calculated the attachment loss (AL) and probing depth (PD) for each participant, which were used to further explore the relationships between periodontal parameters and the prevalence and prognosis of MetS.
Diagnostic Definitions for MetS
MetS is defined using harmonized criteria proposed by the International Diabetes Federation (IDF) and the American Heart Association/National Heart, Lung, and Blood Institute (AHA/NHLBI) in 2009.2 When at least three of the following five elements are present, MetS is diagnosed. (1): waist circumference (WC) not less than 102 cm for men and not less than 88 cm for women; (2) triglycerides (TG) not less than 150 mg/dL; (3) blood pressure (BP) ≥130 mmHg or diastolic BP ≥85 mmHg, or the use of antihypertensive medication; (4) fasting blood glucose (FBG) not less than 100 mg/dL, or the use of medication to control blood glucose levels; (5) high-density lipoprotein cholesterol (HDL) less than 50 mg/dL for women and less than 40 mg/dL for men, or the use of medication to manage lipid levels.
Mortality Data and Definition
Following the International Classification of Diseases (ICD-10), which is employed to identify potential causes of death, the NCHS categorizes cardiovascular mortality as death due to heart disease, denoted by the ICD-10 codes I00-I09, I11, I13, and I20-I51.14
Definition of Covariables
The demographic characteristics included age, gender, race, and education. Education was categorized into three groups: less than high school, high school, and more than high school. Using 100 cigarettes as nodes, smoking status was defined as follows: “never” for those who had smoked fewer than 100 cigarettes in their lifetime, “former” for those who had smoked more than 100 cigarettes but were not currently smoking, and “now” for those who had smoked more than 100 cigarettes and were currently smoking either occasionally or regularly.15 The categorization of alcohol consumption status was defined as follows: “never” (fewer than 12 drinks in a lifetime), “former” (at least 12 drinks in one year but none in the past year, or no drinks in the past year but at least 12 drinks in a lifetime), “mild” (an average of up to 1 drink per day for women or up to 2 drinks per day for men over the past 12 months), “moderate” (1 to 3 drinks per day for women or 2 to 4 drinks per day for men), and “heavy” (an average of 4 or more drinks per day for women or 5 or more drinks per day for men in the past 12 months).16 The Healthy Eating Index-2015 (HEI-2015) is a dietary quality metric devised by the Center for Nutrition Policy and Promotion at the United States Department of Agriculture (USDA). If the two-day average HEI-2015 score was at or above the 60th percentile, individuals were considered to “healthy diet”; otherwise, they were classified as “unhealthy diet”.17,18 Physical activity (PA) data were collected through a questionnaire-based on the Global Physical Activity Questionnaire, which categorized respondents according to adherence to US PA guidelines (adults should perform moderate-intensity PA for at least 150 minutes per week, equivalent to 600 metabolic equivalent (MET) minutes per week). Based on PA recommendations, individuals were categorized as “physically inactive” (fewer than 600 MET minutes per week) or “physically active” (600 or more MET minutes per week).18,19
Statistical Analysis
Due to the intricate NHANES sampling design, all analyses accounted for sample weights to accurately analyze the NHANES data. Weighted means ± standard errors were applied to continuous data, whereas weighted frequency percentages represented categorical variables. Mann–Whitney U-test and Rao-Scott test were to examine the differences between the two groups. Logistic regression models were performed to examine the associations between periodontitis and the prevalence of MetS prevalence. Cox regression models were used to analyze the effect of periodontitis on all-cause and cardiovascular mortality in MetS individuals. We constructed three models to control for the influence of potential confounding variables. Model 1: Unadjusted model; Model 2: Adjusted for age, gender, race; Model 3: Adjusted for age, gender, race, smoking status, alcohol consumption, education, physical activity, and HEI-2015. The restricted cubic spline (RCS) analysis was conducted to explore the dose-response associations of AL and PD with the prevalence, all-cause mortality, and cardiovascular mortality in MetS. R software (version 4.3.1) was used for all analyses in this study.
Results
Baseline Characteristics
Table 1 indicates that 9,270 individuals in all were enrolled in the research, comprising 3303 individuals with MetS and 5967 without MetS. MetS individuals were more highly distributed among those ≥ 60 years, unhealthy diets, physical activity inactive, and periodontitis. Furthermore, there were differences between all variables except gender.
 |
Table 1 The Baseline Characteristics of Individuals in This Study |
Association Between Periodontitis and the Prevalence of MetS and Its Components
As displayed in Table 2, all three models demonstrated the increased risk of MetS in individuals with periodontitis compared to those without periodontitis (Model 1: OR=1.48, 95% CI 1.30–1.69; Model 2: OR=1.38, 95% CI:1.21–1.59; Model 3: OR=1.24, 95% CI: 1.08–1.43). Moreover, periodontitis was associated with an increased risk of elevated FBG (P < 0.001), WC (P < 0.002), and BP (P < 0.001), which are components of MetS. However, no association was found between periodontitis and elevated TG (P = 0.238) or decreased HDL levels (P = 0.635). Given the significance of periodontal parameters AL and PD in evaluating the severity of periodontitis, we conducted a further analysis to explore the impact of AL and PD on the prevalence of MetS and its components. It can be seen from Tables 3 and 4 that both AL and PD were associated with the prevalence MetS, respectively (P < 0.05), although significant association were not observed with all components of MetS. Compared to the Q1, individuals in the Q4 quantile of AL had a 31% increased risk of MetS (OR=1.31, 95% CI: 1.06–1.61, Table 3). Similarly, individuals in the Q4 quantile of PD demonstrated a 32% increased risk of MetS (OR=1.32, 95% CI: 1.10–1.59, Table 4). However, the results of the RCS analysis shown in Figure 2A indicated a nonlinear association between AL and the prevalence of MetS (P for non-linearity < 0.001). However, PD was significantly positively associated with the prevalence of MetS (Figure 2B, P for overall = 0.004).
 |
Table 2 The Association Between Periodontitis and the Prevalence of MetS and Its Components |
 |
Table 3 The Association Between AL and the Prevalence of MetS and Its Components |
 |
Table 4 The Association Between PD and the Prevalence of MetS and Its Components |
 |
Figure 2 Restricted cubic spline curves for the associations of AL and PD with the risk of MetS. OR were adjusted for age, gender, race, education, smoking status, alcohol consumption, physical activity, and HEI-2015. (A) AL and the risk of MetS; (B) PD and the risk of MetS. Abbreviations: AL, attachment loss; PD, probing depth; OR, Odds Ratio; CI, Confidence Interval. |
Association Between Periodontitis and the Prognosis of MetS
KM survival curves analysis and Cox proportional hazards regression models were used to compare the impact of periodontitis on the prognosis for survival in individuals in the MetS. As displayed in Figure 3A and B, the KM analysis revealed that individuals with periodontitis had significantly higher all-cause and cardiovascular mortality compared to those without periodontitis among individuals with MetS (P < 0.001). As seen in Table 5, three models all demonstrated that periodontitis was associated with an increased risk of all-cause mortality (Model 1: HR = 2.67, 95% CI: 1.92–3.70; Model 2: HR = 2.29, 95% CI: 1.58–3.32; Model 3: HR = 2.03, 95% CI: 1.40–2.92) and cardiovascular mortality (Model 1: HR = 3.29, 95% CI: 1.59–6.82; Model 2: HR = 2.46, 95% CI: 1.12–5.41; Model 3: HR = 2.32, 95% CI:1.05–5.10). Table 6 indicated that individuals in the Q4 quartile of AL demonstrated a significantly higher risk of both all-cause mortality (HR = 3.77, 95% CI: 2.43–5.84) and cardiovascular mortality (HR = 4.28, 95% CI: 1.73–10.61) compared to Q1. Meanwhile, a similar trend was observed for PD, where individuals in the Q4 quartile suggested an increased risk of all-cause mortality (HR = 1.90, 95% CI: 1.21–3.00) and cardiovascular mortality (HR = 3.13, 95% CI: 1.21–8.05) compared to those in Q1. In addition, we further investigated the impact of changes in AL and PD on the prognosis of MetS individuals by RCS analysis. Figure 4A and B demonstrated nonlinear associations between AL and the risks of all-cause (P for non-linearity < 0.001) and cardiovascular (P for non-linearity = 0.007) mortality. Specifically, when AL exceeded a value of 2, the effect of further increases of AL on all-cause and cardiovascular mortality gradually stabilized in MetS. In contrast, PD displayed linear associations with both all-cause (P for overall = 0.004) and cardiovascular (P for overall < 0.001) mortality, with risk continuously escalating as PD levels increased (Figure 4C and D).
 |
Table 5 The Association Between Periodontitis and the Prognosis of MetS |
 |
Table 6 The Association of AL and PD With the Prognosis of MetS |
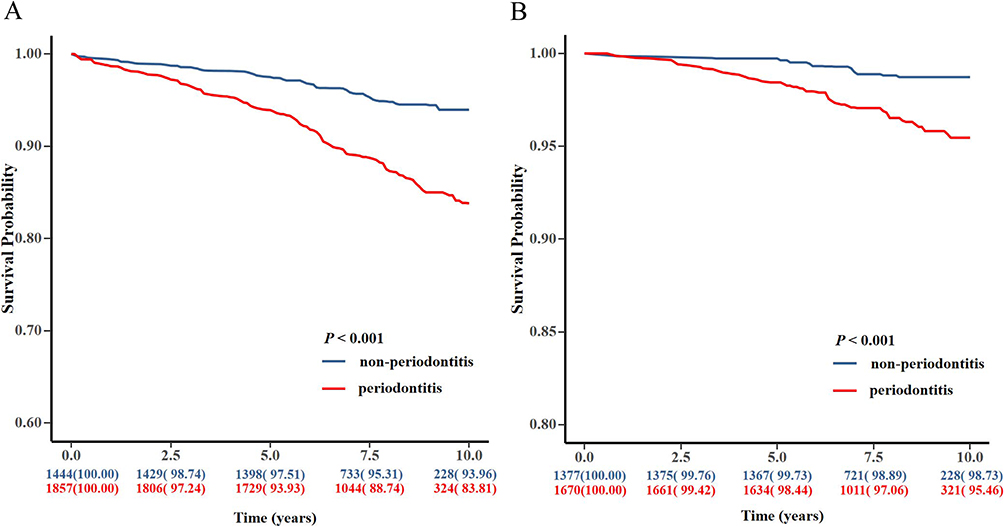 |
Figure 3 Kaplan‒Meier survival curves of MetS patients with/without periodontitis. (A) All-cause mortality; (B) Cardiovascular mortality. Abbreviations: AL, attachment loss; PD, probing depth. |
 |
Figure 4 Restricted cubic spline curves for the associations of AL and PD with the prognosis of MetS. (A) AL and the risk of all-cause mortality. (B) AL and the risk of cardiovascular mortality. (C) PD and the risk of all-cause mortality. (D) PD and the risk of cardiovascular mortality. HR were adjusted for age, gender, race, education, smoking status, alcohol consumption, physical activity, and HEI-2015. Abbreviations: AL, attachment loss; PD, probing depth. |
Discussion
MetS has become a global health concern as Western lifestyles become more prevalent and economic growth accelerates.20 It is a complex disorder that brings together several distinct health issues. Without proper management, it could gradually develop into metabolic imbalances, eventually increasing mortality.21 In this study, we investigated the effect of periodontitis on MetS using the NHANES database.
Considering that variables such as age, gender, race, smoking, alcohol consumption, education, physical activity, and diet are shared influence factors for various chronic diseases,22 we constructed three models to minimize potential interference in this study. Consistent with the findings of most research,12,23 all models in our analysis indicated periodontitis could increase the risk of MetS compared to non-periodontitis. MetS comprises five components: WC, BP, FBG, TG, and HDL. Therefore, we also investigated the association between periodontitis and each component of MetS. The results showed that periodontitis was significantly associated with abdominal obesity, elevated blood pressure, and high blood glucose levels. There is strong evidence supporting these findings. For instance, a recent 8-year longitudinal study conducted in Japan by Saito M et al revealed an association between periodontitis and abdominal obesity, suggesting that the underlying mechanisms may involve inflammatory cytokines and reactive oxygen species (ROS),5 Furthermore, periodontitis may worsen diabetes progression by increasing the levels of tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and resistin. These mediators interfere with insulin receptors and their downstream signaling pathways, resulting in insulin resistance and subsequent increases in blood glucose levels.24 Some studies reported that periodontitis could increase the prevalence of hypertension and identified that c-reactive proteins and leukocyte levels, markers of systemic inflammation, could serve as biological mediators in this relationship.25,26 Similarly, a recent cohort study demonstrated that BP was higher in participants with periodontitis compared to those without, which may be related to oral-gut microbial transmission.27 In summary, the increased risk of MetS associated with periodontitis may be attributed to the involvement of inflammatory cytokines, oxidative stress, microbial dysbiosis and so on. Moreover, periodontitis has been considered to potentially affect lipid metabolism in previous studies, including the ability to elevate TG levels and reduce HDL levels.28,29 Notably, this association was not observed in our study. A possible and sensible interpretation of these results might be that differences in study populations and confounding factors in the analysis may have influenced the results.
In addition, periodontitis, as a chronic inflammatory disease, has been widely recognized as associated with increased all-cause mortality and cardiovascular mortality in the general population.30 Therefore, we further explored the impact of periodontitis on the prognosis of MetS. Our study indicates that periodontitis increases the risk of all-cause and cardiovascular mortality in MetS participants. The mechanisms by which periodontitis contributes to mortality in individuals with MetS remain unclear. However, it is well-established that periodontitis is associated with poor prognoses in various chronic diseases, including diabetes and hypertension.31,32 Further comprehensive and in-depth research is undoubtedly needed in the future.
After evaluating the effects of periodontal parameters on MetS, PD and AL were found to be significantly associated with the prevalence and prognosis of MetS, further supporting our conclusions. Additionally, RCS analysis revealed PD was positively associated with the prevalence, all-cause mortality, and cardiovascular mortality in MetS. However, beyond a certain threshold of AL, the risk for MetS gradually decreases, which was similar to the findings of Fukui N.33 A plausible explanation is that deep PD signifies the current state of inflammation in periodontal tissues, whereas the presence of AL indicates cumulative periodontal tissue damage caused by periodontitis, which may not necessarily reflect the current inflammatory status.33,34
This study utilized a weighted design based on the NHANES sample to ensure nationwide representativeness.35–37 Furthermore, we not only investigated the association between periodontitis and the risk of MetS but also evaluated the potential impact of periodontitis on the poor prognosis of MetS, providing valuable insights and references for further research in this field. However, there are several limitations should be acknowledged. First, although our results indicated a positive association between periodontitis and MetS parameters, as a cross-sectional study, we cannot infer causality from this association. Second, rigorous adjustments were performed to account for confounding factors, but the potential impact of unmeasured or residual confounders cannot be entirely eliminated. Additionally, the absence of oral imaging data in the NHANES 2009–2014 dataset restricted the utilization of the most recent classification criteria for periodontitis.38 Therefore, large-scale prospective studies are required to establish the causal relationship between periodontitis and MetS and to elucidate the underlying mechanisms.
Conclusion
In conclusion, periodontitis may be linked to a higher risk of MetS and increased all-cause and cardiovascular mortality. It is advised that healthcare professionals consider periodontitis as a potential factor when preventing and managing MetS. Early intervention and treatment of periodontitis may, to some extent, improve the prognosis of MetS, thereby contributing to the overall health improvement of patients.
Data Sharing Statement
Publicly available datasets were analyzed in this study. This data can be found here: www.cdc.gov/nchs/nhanes/.
Ethics Approval and Consent to Participate
The NHANES 2009-2014 was approved by the NCHS Research Ethics Review Board (NHANES 2009-2010: Continuation of Protocol #2005-06; NHANES 2001-2014: Protocol #2011-17) and acquired all the eligible individuals’ informed consent. And The Ethics Committee of The First Affiliated Hospital, Jiangxi Medical College, Nanchang University deemed that this research is based on open-source data, so the need for ethics approval was waived.
Acknowledgments
Thanks to the creators of the NHANES database and all the staff for providing us with a public database.
Author Contributions
All authors reviewed the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the First Affiliated Hospital of Nanchang University Clinical Research and Cultivation Project (YFYLCYJPY202305), the National Natural Science Foundation of China (81560189), the Science and Technology Plan of Jiangxi Provincial Health Commission (SKJP220219792).
Disclosure
All authors declare no conflict of interest in this study.
References
1. Ahluwalia N, Raghavan R, Zhang G, et al. Vitamin D status and prevalence of metabolic syndrome by race and Hispanic origin in US adults: findings from the 2007–2014 NHANES. Am J Clin Nutr. 2022;116(5):1400–1408. doi:10.1093/ajcn/nqac234
2. Qureshi D, Collister J, Allen NE, et al. Association between metabolic syndrome and risk of incident dementia in UK Biobank. Alzheimers Dement. 2024;20(1):447–458. doi:10.1002/alz.13439
3. Zhao Y, Shao W, Zhu Q, et al. Association between systemic immune-inflammation index and metabolic syndrome and its components: results from the National Health and Nutrition Examination Survey 2011–2016. J Transl Med. 2023;21(1):691. doi:10.1186/s12967-023-04491-y
4. Chen Y, Xu W, Zhang W, et al. Plasma metabolic fingerprints for large-scale screening and personalized risk stratification of metabolic syndrome. Cell Rep Med. 2023;4(7):101109. doi:10.1016/j.xcrm.2023.101109
5. Saito M, Shimazaki Y, Yoshii S, et al. Periodontitis and the incidence of metabolic syndrome: an 8-year longitudinal study of an adult Japanese cohort. J Clin Periodontol. 2024;51(1):54–62. doi:10.1111/jcpe.13881
6. Nazir MA, AlGhamdi L, AlKadi M, et al. The burden of diabetes, its oral complications and their prevention and management. Open Access Maced J Med Sci. 2018;6(8):1545–1553. doi:10.3889/oamjms.2018.294
7. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Clin Periodontol. 2018;45(Suppl 20):S149–S161. doi:10.1111/jcpe.12945
8. Milanesi FC, Greggianin BF, Dos SG, et al. Effect of periodontal treatment on glycated haemoglobin and metabolic syndrome parameters: a randomized clinical trial. J Clin Periodontol. 2023;50(1):11–21. doi:10.1111/jcpe.13717
9. Ye X, Bai Y, Li M, et al. Genetic associations between circulating immune cells and periodontitis highlight the prospect of systemic immunoregulation in periodontal care. Elife. 2024;12. doi:10.7554/eLife.92895.3
10. Suh JS, Kim S, Bostrom KI, et al. Periodontitis-induced systemic inflammation exacerbates atherosclerosis partly via endothelial-mesenchymal transition in mice. Int J Oral Sci. 2019;11(3):21. doi:10.1038/s41368-019-0054-1
11. Thomas JT, Joseph B, Varghese S, et al. Association between metabolic syndrome and salivary MMP-8, myeloperoxidase in periodontitis. Oral Dis. 2024.
12. Ayuthaya B, Lertpimonchai A, Samaranayake L, et al. The potential effect of periodontal disease on the development of metabolic syndrome: a 10-year observational study in a Thai Adult Cohort. J Clin Periodontol. 2024;52:339–352. doi:10.1111/jcpe.14068
13. Eke PI, Page RC, Wei L, et al. Update of the case definitions for population-based surveillance of periodontitis. J Periodontol. 2012;83(12):1449–1454. doi:10.1902/jop.2012.110664
14. Zhang X, Wei R, Wang X, et al. The neutrophil-to-lymphocyte ratio is associated with all-cause and cardiovascular mortality among individuals with hypertension. Cardiovasc Diabetol. 2024;23(1):117. doi:10.1186/s12933-024-02191-5
15. Dong G, Gan M, Xu S, et al. The neutrophil-lymphocyte ratio as a risk factor for all-cause and cardiovascular mortality among individuals with diabetes: evidence from the NHANES 2003–2016. Cardiovasc Diabetol. 2023;22(1):267. doi:10.1186/s12933-023-01998-y
16. Jiang M, Tang X, Wang P, et al. Association between daily alcohol consumption and serum alpha klotho levels among U.S. adults over 40 years old: a cross-sectional study. BMC Public Health. 2023;23(1):1901. doi:10.1186/s12889-023-16830-1
17. Liang J, Huang S, Jiang N, et al. Association between joint physical activity and dietary quality and lower risk of depression symptoms in US Adults: cross-sectional NHANES Study. JMIR Public Health Surveill. 2023;9:e45776. doi:10.2196/45776
18. Zhu Y, Wang Z. Association between joint physical activity and healthy dietary patterns and hypertension in US adults: cross-sectional NHANES study. BMC Public Health. 2024;24(1):855. doi:10.1186/s12889-024-18346-8
19. Chu NM, Hong J, Harasemiw O, et al. Chronic kidney disease, physical activity and cognitive function in older adults-results from the National Health and Nutrition Examination Survey (2011–2014). Nephrol Dial Transplant. 2022;37(11):2180–2189. doi:10.1093/ndt/gfab338
20. Lu Y, Wang M, Bao J, et al. Association between oxidative balance score and metabolic syndrome and its components in US adults: a cross-sectional study from NHANES 2011–2018. Front Nutr. 2024;11:1375060. doi:10.3389/fnut.2024.1375060
21. Bruzzone C, Gil-Redondo R, Seco M, et al. A molecular signature for the metabolic syndrome by urine metabolomics. Cardiovasc Diabetol. 2021;20(1):155. doi:10.1186/s12933-021-01349-9
22. Marruganti C, Suvan JE, D’Aiuto F. Periodontitis and metabolic diseases (diabetes and obesity): tackling multimorbidity. Periodontol. 2023. doi:10.1111/prd.12536
23. Gomes-Filho IS, Balinha I, Da CS, et al. Moderate and severe periodontitis are positively associated with metabolic syndrome. Clin Oral Investig. 2021;25(6):3719–3727. doi:10.1007/s00784-020-03699-2
24. Jepsen S, Suvan J, Deschner J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontol. 2020;83(1):125–153. doi:10.1111/prd.12326
25. Munoz AE, Leira Y, Miro CQ, et al. Is systemic inflammation a missing link between periodontitis and hypertension? Results from two large population-based surveys. J Intern Med. 2021;289(4):532–546. doi:10.1111/joim.13180
26. Torrungruang K, Vathesatogkit P, Mahanonda R, et al. Periodontitis and hypertension are linked through systemic inflammation: a 5-year longitudinal study. J Clin Periodontol. 2024;51(5):536–546. doi:10.1111/jcpe.13942
27. Chen BY, Lin WZ, Li YL, et al. Roles of oral microbiota and oral-gut microbial transmission in hypertension. J Adv Res. 2023;43:147–161. doi:10.1016/j.jare.2022.03.007
28. Zhou LJ, Lin WZ, Meng XQ, et al. Periodontitis exacerbates atherosclerosis through Fusobacterium nucleatum-promoted hepatic glycolysis and lipogenesis. Cardiovasc Res. 2023;119(8):1706–1717. doi:10.1093/cvr/cvad045
29. Mikami R, Mizutani K, Matsuyama Y, et al. Association between periodontal inflammation and serum lipid profile in a healthy population: a cross-sectional study. J Periodontal Res. 2021;56(6):1037–1045. doi:10.1111/jre.12917
30. Bond JC, McDonough R, Alshihayb TS, et al. Periodontitis is associated with an increased hazard of mortality in a longitudinal cohort study over 50 years. J Clin Periodontol. 2023;50(1):71–79. doi:10.1111/jcpe.13722
31. Li W, Peng J, Shang Q, et al. Periodontitis and the risk of all-cause and cause-specific mortality among US adults with diabetes: a population-based cohort study. J Clin Periodontol. 2024;51(3):288–298. doi:10.1111/jcpe.13901
32. Li J, Yao Y, Yin W, et al. Association of periodontitis with cardiovascular and all-cause mortality in hypertensive individuals: insights from a NHANES cohort study. BMC Oral Health. 2024;24(1):950. doi:10.1186/s12903-024-04708-6
33. Fukui N, Shimazaki Y, Shinagawa T, et al. Periodontal status and metabolic syndrome in middle-aged Japanese. J Periodontol. 2012;83(11):1363–1371. doi:10.1902/jop.2012.110605
34. Watanabe K, Cho YD. Periodontal disease and metabolic syndrome: a qualitative critical review of their association. Arch Oral Biol. 2014;59(8):855–870. doi:10.1016/j.archoralbio.2014.05.003
35. Frank SM, Jaacks LM, Meyer K, et al. Dietary quality and dietary greenhouse gas emissions in the USA: a comparison of the planetary health diet index, healthy eating index-2015, and dietary approaches to stop hypertension. Int J Behav Nutr Phys Act. 2024;21(1):36. doi:10.1186/s12966-024-01581-y
36. Assadourian JN, Peterson ED, Gupta A, et al. Use of dietary supplements among people with atherosclerotic cardiovascular disease in the United States: a population-based analysis from NHANES. J Am Heart Assoc. 2024;13(9):e33748. doi:10.1161/JAHA.123.033748
37. Hampson HE, Costello E, Walker DI, et al. Associations of dietary intake and longitudinal measures of per- and polyfluoroalkyl substances (PFAS) in predominantly Hispanic young Adults: a multicohort study. Environ Int. 2024;185:108454. doi:10.1016/j.envint.2024.108454
38. Guo J, Xu R, Liu R, et al. Association between the systemic immune inflammation index and periodontitis: a cross-sectional study. J Transl Med. 2024;22(1):96. doi:10.1186/s12967-024-04888-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.