")
Back to Journals » Clinical Ophthalmology » Volume 19
The Association Between Refraction, Ocular Biometry, and a Child’s Behavior Assessed by Conners’ Parental Rating Scale
Authors Cohen Y , Eidel M, Greenberger Y, Vidan A, Chassid O
Received 24 January 2025
Accepted for publication 25 March 2025
Published 1 April 2025 Volume 2025:19 Pages 1183—1190
DOI https://doi.org/10.2147/OPTH.S513759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuval Cohen,1,2 Michael Eidel,3 Yehuda Greenberger,1 Aviv Vidan,1,2 Otzem Chassid1,2
1Department of Ophthalmology, Ziv Medical Center, Safed, Israel; 2Azrieli Faculty of Medicine, Bar-Ilan University, Safed, Israel; 3Pediatric Neurology and Child Development Institute, Hillel Yaffe Medical Center, Hadera, Israel
Correspondence: Yuval Cohen, Department of Ophthalmology, Ziv Medical Center, Safed, Israel, Email [email protected]
Purpose: To examine the association between refraction, ocular biometry and a child’s behavioral disorder using the Conners’ Parent Rating Scale.
Materials and Methods: This cohort study recruited 139 children aged 6– 9 years old. Their legal guardians completed the Conners’ Parent Rating Scale [the revised-long version (CPRS-R-L)], and the individual responses were entered into the software scoring program, resulting in 14 scores for behavioral disorders. Cycloplegic refraction and ocular biometry were performed. Correlation analyses among the 14 behavioral scores, refraction, and biometry were performed. The analyses were performed for three refractive groups: hyperopia, emmetropia, and myopia.
Results: Children (N = 93) with mean age of 7.2 ± 1.2 y were included. Spherical equivalent (SE) of the refractive groups were +3.46± 1.71 diopters (D), 0.61 ± 0.41 D and − 1.76 ± 2.15 D (p < 0.0001). The CPRS-R-L subscale scores positively correlated with sphere, SE, and negatively correlated with cylinder. With the exception of oppositional behavioral subscale that had higher than mean score, 13 CPRS-R-L scores fell within the normal range, regardless of refraction. CPRS-R-L subscale scores negatively correlated with axial length. Axial length shorter than 22.5 mm had CPRS-R-L 95th percentile, some of which surpassed the normal range score of CPRS-R-L, and indicate the presence of ADHD concerns.
Conclusion: Refraction, astigmatism, and axial length were associated with Conners’ behavioral subscales and warrant additional studies to clarify any cause–effect relationship.
Keywords: hyperopia, ADHD, Conners’ parental rating scale, a child’s behavior, ocular biometry
Introduction
Childhood behavioral disorders, including ADHD, result in learning difficulties. Studying the link between refraction and disruptive behavioral patterns is challenging. Tools used to examine a child’s behavioral development should be developmentally sensitive and account for age-appropriate variation. Several studies have examined the link between refractive error and ADHD, a chronic condition that affects children and includes a combination of persistent problems such as difficulty sustaining attention, hyperactivity, and impulsive behavior.1–3 Aghai et al,4 reported a high rate of behavioral disorders in hyperopic and hyperopia-astigmatic children. Their study used the Rutter questionnaire, a screening tool that has been designed to detect behavioral disorders other than ADHD. Mezer and Wygnanski-Jaffe,3 evaluated ocular features in children with ADHD and reported significant ametropia, particularly astigmatism, in most cases. Additionally, binocular function difficulties and convergence insufficiency have also been found to be associated with ADHD.5,6 Contrary to this, Fabian et al7 reported that hyperopia and astigmatism were not more common in the ADHD group; thus, they concluded that it could not be a major factor contributing to disabilities associated with ADHD in children. Therefore, the contribution of refractive error to behavioral disorders and ADHD remains controversial. Studies examining the association between ocular biometry and children’s behavior are scarce.
The revised Conners’ Rating Scale (CRS-R) is used to assess ADHD and other behavioral problems in children.8 Conners’ Parent Rating Scale (CPRS) was developed as a comprehensive checklist for acquiring parental reports on childhood behavioral problems.9 The revised-long version CPRS (CPRS-R-L), answered by parents, consists of 80 items and includes 14 index scores related directly to ADHD scores. The other half was related to comorbid behavioral problems.
The objectives of this study were to examine the correlation between refraction, ocular biometry and CPRS-R:L index scores related to ADHD and its comorbid behavioral problems in children ages 6–9.
Materials and Methods
This retrospective cohort study was designed to correlate refraction and ocular biometry, to behavior evaluated by CPRS-R-L in children aged 6–9 years who were referred to the pediatric ophthalmology clinic for refractive error follow-up or suspected refractive error. The study was approved by Ziv Medical Center Ethics Committee in 2020 and was performed in accordance with the tenets of the Declaration of Helsinki of the World Medical Association. Written informed consent was obtained from all participants’ legal guardians. Individuals with a history of ocular surgery or other abnormalities that compromise visual function, such as cataracts, glaucoma, retinitis pigmentosa, retinal detachment, or strabismus, were excluded. Data of age at first prescription glasses was documented, and we excluded ametropic children who wore glasses for less than six months. The subjects included were in regular education classes and accompanied by their legal guardians who completed the CPRS-R-L.
Refraction and Examination
Cycloplegia was induced with 1 drop of cyclopentolate 1.0% and 1 drop of Tropicamide 1% administered twice, 10 minutes apart. Cycloplegic refraction was performed using an autorefractor (KR-8800, Topcon Corp). Before dilation, the anterior segment was examined using a slit lamp. After pupil dilation, fundus examination was performed by a trained ophthalmologist using a 90.0 D lens (Volk Optical, Inc) to exclude other eye diseases. We defined the groups according to their SE accordingly: hyperopic (SE > +1D), emmetropic (+1.0D to −0.5D) and myopic (<-0.5D).
Ocular Biometry
Optical biometric measurements using the Lenstar LS900 were obtained by a trained examiner. All measurements were performed before pupil dilation, in a semi-dark room. Lenstar LS900 measurements for the corneal curvature, central corneal thickness (CCT), anterior chamber diameter (ACD), white-to-white (WTW) diameter, lens thickness and axial length were extracted from the device using a spreadsheet file.
We divided the children into three axial length groups for analysis based on T score results. The inverse correlation between axial length and T score pointed to an intersection between axial length of >22.5 mm and T score of 60 (which is considered a normal value); Axial length >22.5mm defined as relatively long axial length group (N:34). The short (<21.5 mm; N: 27) and medium (21.5–22.5 mm; N: 32) axial length groups were determined by approximately halving the remaining number of participants.
Conners’ Parent Rating Scale
Parents were asked to rate the paper-and-pencil form of the CPRS-R-L, with an 80 item-pool using 4-point Likert scales (ranging from 0 (not at all true) to 3 (very much true). An evaluator input the individual responses to the software scoring program, resulting in 14 raw T-scores. CPRS-R-L converts the raw scores to 14 behavioral subclasses, reflecting what is typical or atypical for that age category (6–9 years in our study) and gender. The behavioral subclasses included oppositional, cognitive problems/inattention, hyperactivity, anxious/shy, perfectionism, social problems, psychosomatic, and ADHD subscales (ADHD index, Conners’ global index [CGI], restless-impulsive, CGI emotional lability, DSM-inattentive, DSM-hyperactive/impulsive, and DSM total). T-scores are presented in Table 1. Percentiles are reported for a normalized standard theoretical distribution as well as from normative data. T-scores falling below 60, generally indicate typical or absent ADHD concerns for the child’s age and gender. Average scores (40–59 score = 16th-83rd percentile) are in the white band, borderline scores are slightly atypical, and are colored pink. The atypical scores and markedly atypical scores (above the 98th percentile) gradually reached a red tone.
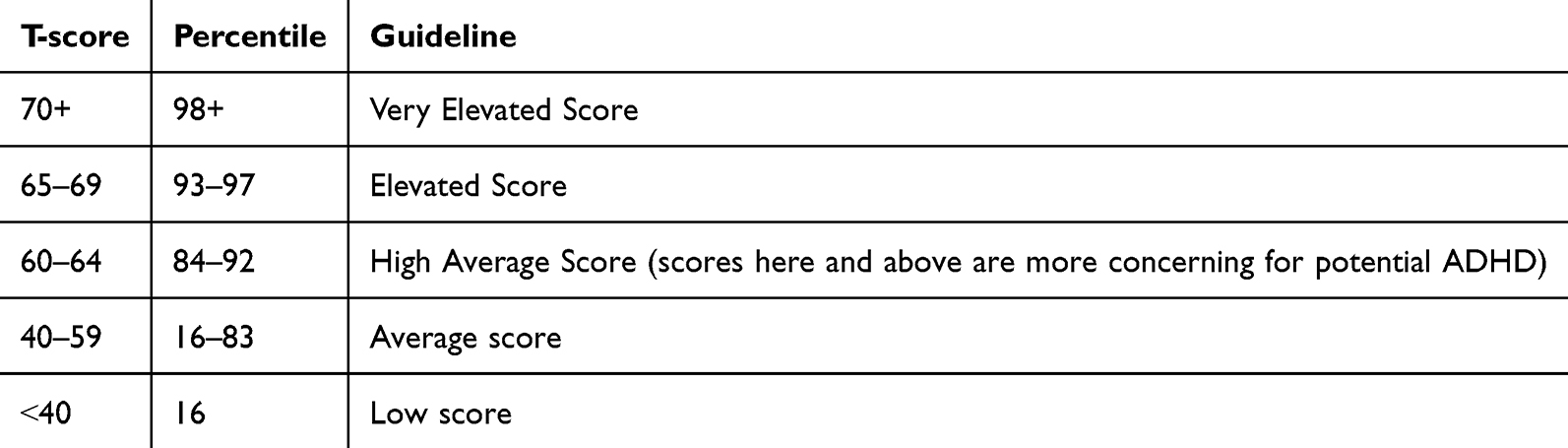 |
Table 1 T Score Levels and Percentile of CPRS-R-L |
Statistical Analysis
We determined the minimum sample size of 90 based on an effect size of 0.25–0.3, significance of 0.05 and power level of 0.80. The estimated low effect size evolved from a pilot data. Results are presented as the mean ± standard deviation (SD). The right eye was used for data collection and analysis. Kendall’s tau rank correlation analysis was used to assess the correlation between refraction (sphere, SE, and cylinder) and biometry parameters, and the T-scores of the subclasses. Data analysis was performed on refraction groups: hyperopic, emmetropic, myopic, and axial length. Analyses were performed using SPSS (version 23.0; IBM Corp., Armonk, NY, USA).
Results
We examined 139 children and included 93 children, excluding those who were noncompliant with completing the Conners’ questionnaire (N = 26) or performing ocular biometry (N = 13). Seven children with ocular pathologies were excluded from this study. Children’s age was 7.23 ± 1.21 years (6–9) and did not significantly correlate with the CRSP-R-L score, verifying that the CRSP-R-L score was independent of age at this specific age (6–9 years) category.
The correlations between CPRS-R-L, refraction and ocular biometry are presented in Table 2. The CPRS-R-L subscale scores positively correlated with sphere, SE, and negatively correlated with cylinder. Corneal curvature, corneal thickness, WTW diameter, ACD, and lens thickness did not correlate with CPRS-R-L. Axial length was the only biometric that correlated with CPRS-R-L and the only biometric parameter presented in Table 2. While the sphere showed a significant positive correlation with the CPRS-R-L in the five subscales, SE had only four positive correlations. A significantly weak inverse correlation was found between axial length and CPRS-R-L subscales; the shorter the axial length, the higher the CPRS-R-L for cognitive problems/inattention, hyperactivity, anxious-shy, impulsive, emotional instability, and ADHD.
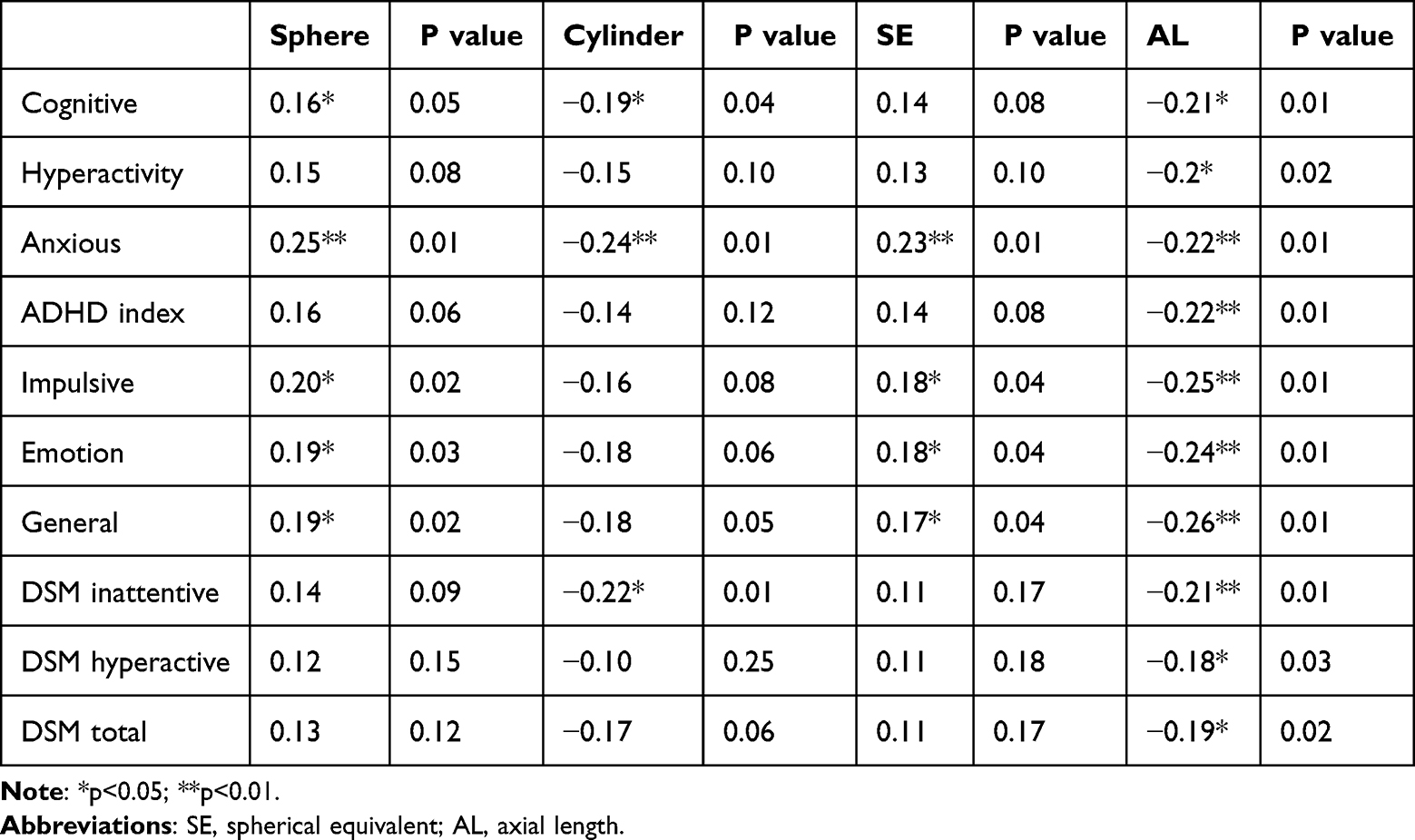 |
Table 2 Correlations Between CPRS-R-L, Refraction and Ocular Biometry |
The hyperopic, emmetropic, and myopic groups had similar mean age (Table 3). The refractive groups differed significantly in sphere, SE, ACD, and axial length (p < 0.05). Children underwent follow-up examinations for hyperopic and myopic refractive errors at least 6 months after their vision prescription was given. The time from first prescription glasses for the hyperopic and myopic participants was 3.68 ± 1.31 and 1.11 ± 1.13 years, respectively.
 |
Table 3 Demographic, Refraction and Biometry |
Figure 1 depicts the CPRS-R-L for hyperopic, emmetropic, and myopic children. With the exception of the oppositional subscale score for the hyperopic group, most T-scores fell within the normal range of 40–59, regardless of their refraction. Hyperopic children had oppositional subscale scores greater than 83% (63.07 ± 16.32), which is considered borderline for children age 6–9 years. Total ADHD scores were 56.26 ± 13.27, 52.5 ± 10.51, 48.6 ± 6.32 for the hyperopic, emmetropic, and myopic groups, respectively, with statistically non-significant differences/tendency for significance (One-way ANOVA; p=0.14).
 |
Figure 1 Refraction Groups and CPRS-R-L. Figure 1 depicts the CPRS-R-L for the hyperopic, emmetropic and myopic children at each behavioral subtype. Most subtype scores fall within normal range. Error bars: 95% confidence interval. |
Based on CPRS-R-L scores, we divided the children into three axial length groups for further analysis depicted in Figure 2 (short, medium, and relatively long axial length groups, <21.5 mm (N:27), 21.5–22.5 mm (N:32), >22.5 mm (N:34), respectively). The CPRS-R-L of the axial length groups significantly differed in cognitive, hyperactivity, ADHD index, impulsivity, emotion, DSM general, DSM hyperactivity, and DSM total scores (One-Way ANOVA; P = 0.08, 0.03, 0.03, 0.001, 0.03, 0.02, and 0.03, respectively). Except for the oppositional behavior, the CPRS-R-L of the relatively long axial length group (> 22.5 mm) was < 60, which was within the normal range. CPRS-R-L of the short and medium axial length groups, in part, surpass the normal T score range in most ADHD subscales.
 |
Figure 2 CPRS-R-L and Axial Length Subgroups. Error bars: 95% confidence interval, Conner’s score: CPRS-R-L. |
Discussion
In our study, the association between refraction, ocular biometry, and behavioral disorders in children was evaluated using the CPRS-R-L. We showed that in children between the ages of 6–9, refraction, astigmatism, and axial length were significantly associated with CPRS-R-L score. The more hyperopic the child is, the higher the CPRS-R-L, which includes cognitive problems/inattention, anxiety, impulsivity, emotion, and general ADHD. The shorter the eye, the higher were the CPRS-R-L subscale scores for cognitive problems/inattention, hyperactivity, anxious-shy, impulsive, emotional instability, and ADHD. This study supports the link between hyperopia and hyperactive, inattentive children.
The Conners’ Rating Scale (CRS) began in 1960 as an untitled collection of informal questions given to parents to document the multiple problematic behaviors of children who brought them to the Harriet Lane Home clinics associated with the Johns Hopkins Hospital in the USA. In 1973, the first version of a psychometric scale, including 93 items, was established, possessing strong and lasting cross-cultural robustness for identifying “hyperkinetic” children.10,11 Conners’ (1997) revision of the CPRS consists of an 80 item long form.8 Factor analysis produced seven behavioral subscales: (1) oppositional, (2) cognitive problems, (3) hyperactivity, (4) anxiety-shy, (5) perfectionism, (6) social problems, and (7) psychosomatic. The CPRS-R:L also contains the Conners’ Global Index (CGI), also known as the impulsive–hyperactive scale, and DSM-IV symptom subscale. Factor analytic studies by Parker et al described two distinct factors of CGI that are now considered subscales of the CGI: (1) emotional lability and (2) restlessness/impulsivity.12 Lastly, the CPRS-R:L assists in the diagnosis of ADHD with its ADHD DSM-IV symptom scale, composed of two subscales meant to distinguish between ADD with and without hyperactivity: (1) DSM-IV Inattentive and (2) DSM-IV hyperactive/impulsive. The Conners’ rating scale analysis was dependent on age. In our study, CPRS-R:L was analyzed for the age range of 6–9 years, where learning and reading skills were challenged by behavioral disruption.
CPRS-R:L has a scale from 38 to 90, with a T-score higher than 60, representing a risk for the specific behavioral subscale. CPRS-R:L does not distinguish between normative individual differences and clinically significant behaviors. The CPRS-R:L should be further assessed by teachers and neurologists to diagnose ADHD and efforts for intervention and prevention.13 In our study, the SE was linked to CPRS-R:L in the inattention, hyperactivity, anxiousness, and impulsiveness subclasses. As most T-scores were below 60, we used the CPRS-R:L as the sole tool for documenting a suspected disruption of behaviors. Further studies are needed to assess the clinical relevance of these differences.
Refractive error, as a part of visual function, is a critical component of a child’s development and can reflect dependent cognitive functions. Hyperopia is associated with learning difficulties, late developmental milestones in reading ability,14 and slow reading speed.15 Moreover, children with uncorrected moderate hyperopia performed significantly worse on early literacy tests than did age-matched controls.16 Previous study showed that impaired reading performance could be artificially induced by simulated bilateral hyperopia, suggesting that refractive error correction can reverse this learning disability.17 In our study, even with correction of refractive error for at least six months, refraction was still associated with behavioral subscales and did not completely lower inattention, hyperactivity, anxiousness, and impulsiveness. Thus, refractive correction may not resolve the learning difficulties.
In general, the correction of hyperopia, particularly in young children, is not straightforward, since most hyperopic refractive errors do not produce symptoms experienced by the child, and the goals of treatment for hyperopia are to improve binocular function and reduce patient symptoms.18 Further studies assessing the CPRS-R:L scores before correcting ametropic and after prescribing glasses might provide an additional insight to the importance of wearing glasses on the child’s behavior.
In our study, axial length was associated with most ADHD scores. The association between the behavioral subscales and ocular structure supports a more complex long-lasting relationship between ocular shape, brain structure, and function, rather than dependence on glasses. It has been hypothesized that there may be a link between axial length of the eyeball and cerebral development in children with myopia.19 Brain structural changes noted in children diagnosed with ADHD showed small intracranial volumes and subcortical brain structures relative to controls.20 Moreover, ADHD symptoms have been associated with functional abnormalities in the left subgyral white matter of the frontal lobe, right medial frontal gyrus, right cingulate, and the frontal lobe.21 Further studies should be performed to evaluate the link between ocular and brain structures in children with ADHD and their related behaviors.
The limitations of our study include: First, the use of the Conners’ Parental Score, a subjective questionnaire that could be biased by overprotective parents rating a child’s behavioral disruption as lower than expected. The CPRS-R:L suggests that the diagnosis of clinically significant behaviors should be confirmed by neurological examination. Second, the study had a high dropout rate of 33%. It is explained by low compliance when completing long questionnaire, and especially when any participants’ legal guardians that had not fully completed the CPRS-R:L was excluded. Third, selection bias as our participants were recruited from a tertiary eye clinic with presumably complex disorders necessitating treatment.
In conclusion, the complexity of the relationships between refraction, astigmatism, axial length, and Conners’ behavioral subscale scores warrant additional studies to clarify any cause–effect relationship.
Acknowledgments
The abstract of this paper was presented at Investigative Ophthalmology & Visual Science (ARVO) conference as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” at the ARVO conference June 2022, Vol.63, 1426 – F0384.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Granet DB, Gomi CF, Ventura R, Miller-Scholte A. The relationship between convergence insufficiency and ADHD. Strabismus. 2005;13(4):163–168. doi:10.1080/09273970500455436
2. Farrar R, Call M, Maples WC. A comparison of the visual symptoms between ADD/ADHD and normal children. Optometry. 2001;72(7):441–451.
3. Mezer E, Wygnanski-Jaffe T. Do children and adolescents with attention deficit hyperactivity disorder have ocular abnormalities? Eur J Ophthalmol. 2012;22(6):931–935. doi:10.5301/ejo.5000145
4. Aghai G, Dibajnia P, Ashkesh E, Nazari M, Falavarjani KG. Behavior disorders in children with significant refractive errors. J Curr Ophthalmol. 2016;28(4):223–225. doi:10.1016/j.joco.2016.07.007
5. Reimelt C, Wolff N, Hölling H, Mogwitz S, Ehrlich S, Roessner V. The underestimated role of refractive error (Hyperopia, Myopia, and Astigmatism) and strabismus in children with ADHD. J Atten Disord. 2021;25(2):235–244. doi:10.1177/1087054718808599
6. Rouse M, Borsting E, Mitchell GL, et al. Academic behaviors in children with convergence insufficiency with and without parent-reported ADHD. Optom Vis Sci. 2009;86(10):1169–1177. doi:10.1097/OPX.0b013e3181baad13
7. Fabian ID, Kinori M, Ancri O, Spierer A, Tsinman A, Ben Simon GJ. The possible association of attention deficit hyperactivity disorder with undiagnosed refractive errors. J AAPOS. 2013;17(5):507–511. doi:10.1016/j.jaapos.2013.06.005
8. Conners CK. Conners’ Rating Scales—Revised. New York: Multi Health Systems; 1997.
9. Conners CK, Sitarenios G, Parker JD, Epstein JN. The revised Conners’ Parent Rating Scale (CPRS-R): factor structure, reliability, and criterion validity. J Abnorm Child Psychol. 1998;26(4):257–268. doi:10.1023/a:1022602400621
10. Conners CK. Rating scales for use in drug studies with children. Psychopharmacol Bull. 1973;9:24–29.
11. Oesterheld JR, Haber J. Acceptability of the Conners parent rating scale and child behavior checklist to Dakotan/Lakotan parents. J Am Acad Child Adolesc Psychiatry. 1997;36(1):55–63. discussion 63-64. doi:10.1097/00004583-199701000-00018
12. Parker JDA, Sitarenios G, Conners CK. Abbreviated Conners’ rating scales revisited: a confirmatory factor analytic study. Autism Dev Disord. 1996;1:55–62.
13. Egger HL, Angold A. Common emotional and behavioral disorders in preschool children: presentation, nosology, and epidemiology. J Child Psychol Psychiatr. 2006;47(3–4):313–337. doi:10.1111/j.1469-7610.2006.01618.x
14. Shankar S, Evans MA, Bobier WR. Hyperopia and emergent literacy of young children: pilot study. Optom Vis Sci. 2007;84(11):1031–1038. doi:10.1097/OPX.0b013e318157a67a
15. van Rijn LJ, Krijnen JSM, Nefkens-Molster AE, Wensing K, Gutker E, Knol DL. Spectacles may improve reading speed in children with hyperopia. Optom Vis Sci. 2014;91(4):397–403. doi:10.1097/OPX.0000000000000206
16. Kulp MT, Ciner E, Maguire M, et al. Uncorrected hyperopia and preschool early literacy: results of the vision in preschoolers-hyperopia in preschoolers (VIP-Hip) study. Ophthalmology. 2016;123(4):681–689. doi:10.1016/j.ophtha.2015.11.023
17. Narayanasamy S, Vincent SJ, Sampson GP, Wood JM. Impact of simulated hyperopia on academic-related performance in children. Optom Vis Sci. 2015;92(2):227–236. doi:10.1097/OPX.0000000000000467
18. Dusek W, Pierscionek BK, McClelland JF. A survey of visual function in an Austrian population of school-age children with reading and writing difficulties. BMC Ophthalmol. 2010;10:16. doi:10.1186/1471-2415-10-16
19. Saw SM, Tan SB, Fung D, et al. IQ and the association with myopia in children. Invest Ophthalmol Vis Sci. 2004;45(9):2943–2948. doi:10.1167/iovs.03-1296
20. Hoogman M, Bralten J, Hibar DP, et al. Subcortical brain volume differences in participants with attention deficit hyperactivity disorder in children and adults: a cross-sectional mega-analysis. Lancet Psychiatry. 2017;4(4):310–319. doi:10.1016/S2215-0366(17)30049-4
21. Gehricke JG, Kruggel F, Thampipop T, et al. The brain anatomy of attention-deficit/hyperactivity disorder in young adults - a magnetic resonance imaging study. PLoS One. 2017;12(4):e0175433. doi:10.1371/journal.pone.0175433
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.