")
Back to Journals » Journal of Inflammation Research » Volume 17
The Combined Effect of the Systemic Immune-Inflammation Index and Aortic Valve Calcification on Major Adverse Cardiovascular Events in Patients with Coronary Heart Disease
Authors Li M, Li M, Wang Z , Zhang Y
Received 29 August 2024
Accepted for publication 26 October 2024
Published 7 November 2024 Volume 2024:17 Pages 8375—8384
DOI https://doi.org/10.2147/JIR.S493735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tara Strutt
Miaomiao Li,1,2,* Mengchun Li,3,* Zhenwei Wang,4 Yongbo Zhang1,2
1Department of Cardiology, Chest Hospital of Zhengzhou University, Zhengzhou, 450008, People’s Republic of China; 2Department of Cardiology, Henan Province Chest Hospital, Zhengzhou, 450008, People’s Republic of China; 3Department of Pediatrics, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, 450052, People’s Republic of China; 4Department of Cardiology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhenwei Wang; Yongbo Zhang, Email [email protected]; [email protected]
Background: The combined effect of systemic immune-inflammation index (SII) and aortic valve calcification (AVC) on the risk of major adverse cardiovascular events (MACE) in patients with coronary heart disease (CHD) remains unclear. This study aimed to investigate their combined association with MACE in CHD.
Methods: This retrospective cohort study included 846 CHD patients. SII was calculated as platelet count × neutrophil count / lymphocyte count, and AVC status was determined by echocardiography. Patients were divided into four groups based on median SII and AVC presence: Low SII + AVC (-), High SII + AVC (-), Low SII + AVC (+), and High SII + AVC (+). Cox regression, subgroup and sensitivity analyses assessed the association between SII + AVC and MACE.
Results: Multivariate Cox regression revealed that, compared to the Low SII + AVC (-), MACE risk increased 6.542-fold in the High SII + AVC (+) group and 1.605-fold in the High SII + AVC (-) group (P < 0.05). Subgroup analysis indicated that, compared to the Low SII + AVC (-), MACE risk was significantly elevated in the High SII + AVC (-) group for patients over 60, both genders, with hypertension, hyperlipidemia, or without diabetes (P < 0.05). In the Low SII + AVC (+) group, MACE risk was elevated only in males (P < 0.05). The High SII + AVC (+) group had increased MACE risk in all subgroups except those with diabetes (P < 0.05). After excluding patients with estimated glomerular filtration rate < 60 mL/min/1.73m², the high SII + AVC (+) group remained significantly associated with increased MACE risk (P = 0.001), as did the High SII + AVC (-) group (P = 0.031).
Conclusion: The combination of SII and AVC is significantly associated with MACE risk in patients with CHD.
Keywords: systemic immune-inflammation index, aortic valve calcification, coronary heart disease, major adverse cardiovascular events, combined effect
Introduction
Coronary heart disease (CHD) is a leading cause of death and disability worldwide, posing a significant public health challenge and severely threatening human health.1 In recent years, with advances in medical technology and the deepening of clinical research, an increasing number of biomarkers have been used to predict the risk, severity, and prognosis of CHD, aiming to improve the effectiveness of clinical interventions.2–4 However, the prognosis of CHD patients is influenced by multiple factors, among which the systemic immune-inflammation index (SII) and aortic valve calcification (AVC) have gradually attracted the attention of researchers.
The SII is a comprehensive inflammation marker based on the counts of neutrophils, platelets, and lymphocytes in peripheral blood.5 In recent years, SII has been shown to be closely associated with the occurrence and development of various cardiovascular diseases (CVD).6–8 SII not only reflects the body’s immune and inflammatory status but may also play a critical role in the process of atherosclerosis.9 Aortic valve calcification (AVC), a common comorbidity in CHD patients, is closely related to the occurrence of atherosclerosis and cardiovascular events.10,11 Existing studies have shown that AVC is not only closely associated with heart valve disease but may also increase the risk of major adverse cardiovascular events (MACE).12,13
Although SII and AVC are each associated with poor prognosis in CHD patients, studies on the combined impact of these two factors on the risk of MACE in CHD patients are currently limited. Therefore, this study aimed to explore the predictive value of the combined effect of SII and AVC on MACE in CHD patients, with the goal of providing new insights and evidence for clinical risk assessment and personalized treatment.
Methods
Study Population and Design
This retrospective cohort study included a total of 846 patients diagnosed with CHD who were treated at the Henan Province Chest Hospital between September 1, 2016, and September 1, 2022. The inclusion criteria were as follows: (1) age ≥ 18 years; (2) a confirmed diagnosis of CHD; and (3) willingness to participate in follow-up. The exclusion criteria were: (1) loss to follow-up; (2) missing data on neutrophil count, lymphocyte count, or platelet count; (3) missing data on AVC; (4) significant missing data on other clinical parameters; (5) presence of malignancies; (6) severe inflammatory or autoimmune diseases (such as rheumatoid arthritis, systemic lupus erythematosus, or active infections); (7) severe hematological disorders (such as aplastic anemia, leukemia, or lymphoma); (8) severe hepatic or renal failure (such as Child-Pugh class C or chronic kidney disease stage 5); and (9) severe psychiatric or neurological disorders (including schizophrenia or bipolar disorder requiring antipsychotic treatment, as well as severe neurological disorders such as Parkinson’s disease or Alzheimer’s disease). The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. The protocol was reviewed and approved by the Henan Provincial Chest Hospital Ethics Committee. Informed consent was obtained from all participants, or from their legal guardians, prior to inclusion in the study.
Assessment and Definition of SII and AVC
The SII was calculated using the formula: platelet count × neutrophil count / lymphocyte count.5 AVC status was determined via echocardiographic evaluation, with patients classified as AVC positive (+) or negative (-) based on the presence or absence of AVC. Patients were then stratified into four groups based on their median SII and AVC status: Low SII + AVC (-), High SII + AVC (-), Low SII + AVC (+), and High SII + AVC (+).
Follow-Up and Definition of Outcome Variables
The primary outcome was the occurrence of MACE, which included cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, unplanned revascularization, rehospitalization due to worsening heart failure, and rehospitalization due to recurrent angina. Follow-up began at the time of discharge and continued until either the patient’s death or July 31, 2024, whichever occurred first.
Covariate Collection and Definition
Covariates for this study included a range of demographic, clinical, and biochemical parameters. Age and sex were recorded for all participants, along with smoking status, hypertension, diabetes, and hyperlipidemia, which were defined based on clinical diagnoses or the use of corresponding medications. Medication use, including antihypertensive, lipid-lowering, and antidiabetic drugs, was documented as binary variables. Anthropometric and hemodynamic measures included body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate. Biochemical parameters collected included triglycerides, total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and lipoprotein(a). LDL-C was measured directly, and lipoprotein(a) was assessed using the immunoturbidimetric method. Uric acid levels, fasting blood glucose (FBG), and glycated hemoglobin A1c (HbA1c) were measured, along with high-sensitivity C-reactive protein (Hs-CRP) as an indicator of systemic inflammation. Renal function was assessed using creatinine levels and estimated glomerular filtration rate (eGFR). Coagulation status was evaluated through fibrinogen and D-dimer levels, while albumin levels were also recorded. Cardiac function was assessed by measuring left ventricular ejection fraction (LVEF). The diagnosis of CHD was based on the patient’s medical history, symptoms, electrocardiogram (ECG), and coronary angiography results. Specifically, CHD was confirmed by evidence of ischemic changes on the ECG (such as ST-segment elevation or depression, T-wave inversion, etc). or by coronary angiography showing ≥ 50% stenosis in the coronary arteries.14 In this study, CHD patients included both stable CHD patients and acute coronary syndrome patients.
Statistical Analysis
Firstly, the normality of continuous variable data distribution was verified using the Kolmogorov–Smirnov test. Baseline characteristics were presented as means ± standard deviations for normally distributed continuous variables, medians (interquartile ranges) for non-normally distributed continuous variables, and frequencies (percentages) for categorical variables. Differences between groups were assessed using the chi-square test for categorical variables, one-way ANOVA for normally distributed continuous variables, and the Kruskal–Wallis test for non-normally distributed continuous variables. The association between the combination of SII and AVC and the risk of MACE was evaluated using univariate and multivariate Cox proportional hazards regression models. Univariate analysis was initially performed to identify potential predictors, and variables with a P-value < 0.05 were considered for inclusion in the multivariate models. Three multivariate models were constructed: Model 1 was unadjusted, Model 2 was adjusted for age, and Model 3 was adjusted for age, hyperlipidemia, BMI, heart rate, uric acid, eGFR, fibrinogen, albumin, and LVEF. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated. Subgroup analyses were conducted to explore the effect of SII and AVC on MACE across different strata, including age, sex, hypertension, hyperlipidemia, and diabetes status. Sensitivity analyses were performed to confirm the robustness of the results by excluding patients with eGFR < 60 mL/min/1.73m2 and adjusting for all potential confounders included in Model 3. Survival curves were generated using the Kaplan-Meier method, and the Log rank test was used to compare differences in cumulative event rates between groups. All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and R version 4.1.4 (R Foundation for Statistical Computing, Vienna, Austria). A P-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
As shown in Table 1, when comparing the clinical characteristics across different SII and AVC groupings, the study found that the incidence of hyperlipidemia was significantly higher in the high SII with AVC-negative group compared to the low SII with AVC-negative group (P = 0.039), and the heart rate was also higher (P = 0.045). Additionally, the high SII with AVC-positive group exhibited higher levels of inflammation, with significantly elevated Hs-CRP and fibrinogen levels (P = 0.003 and P < 0.001, respectively), and a notable increase in D-dimer levels (P = 0.043). Most importantly, the incidence of MACE was significantly higher in the high SII with AVC-positive group compared to the other groups (P < 0.001).
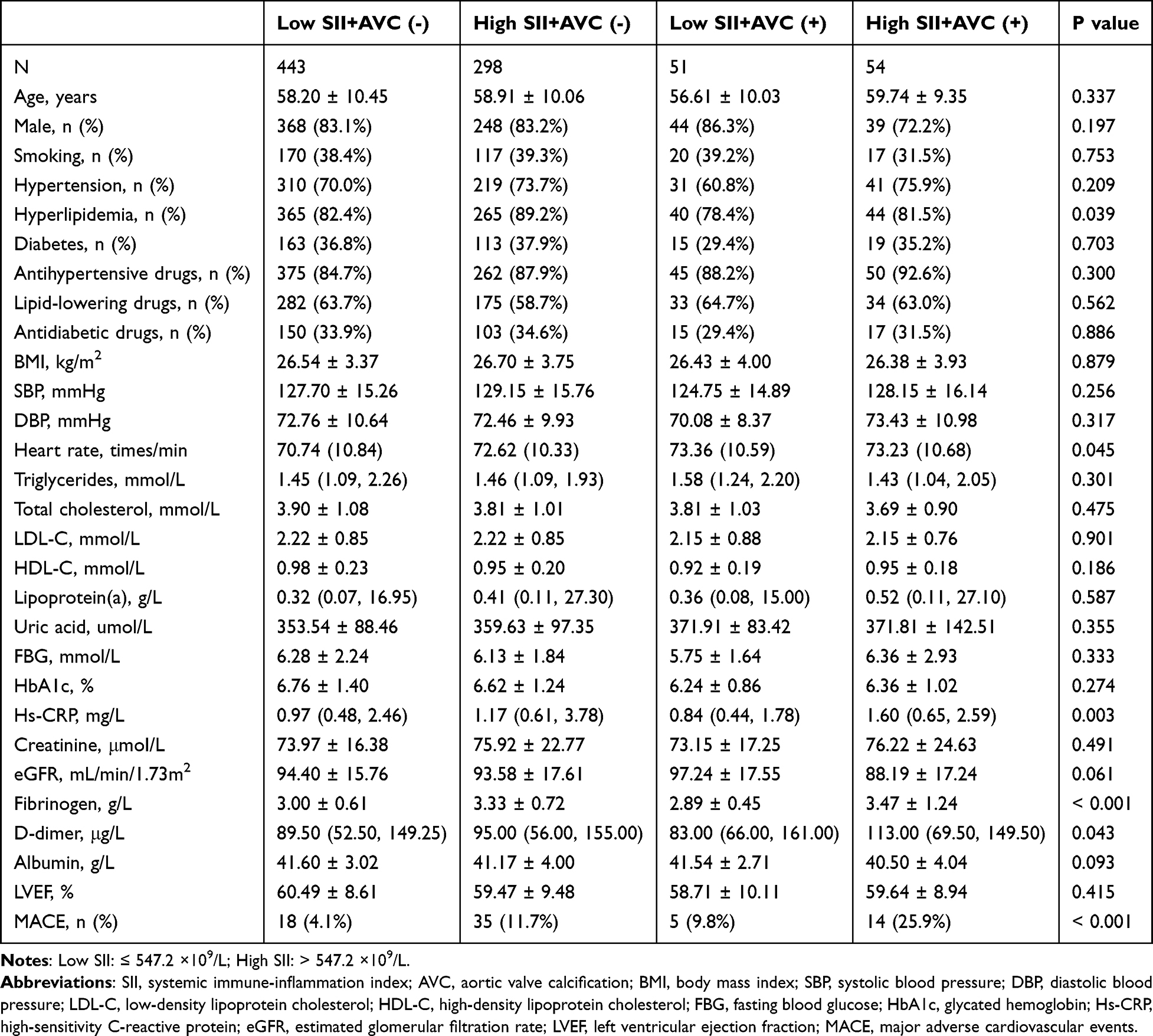 |
Table 1 Comparison of Clinical Characteristics Based on SII and AVC Groupings |
Association Between the Combination of SII and AVC with MACE
During the median follow-up period of 51 months, a total of 72 MACE events occurred. In the univariate Cox regression analysis presented in Table 2, the variables significantly associated with MACE include age (HR = 1.028, P = 0.022), hyperlipidemia (HR = 2.649, P = 0.023), BMI (HR = 0.928, P = 0.036), heart rate (HR = 1.022, P = 0.040), uric acid (HR = 1.003, P = 0.002), creatinine (HR = 1.016, P < 0.001), eGFR (HR = 0.976, P < 0.001), fibrinogen (HR = 1.321, P = 0.044), albumin (HR = 0.916, P = 0.004), and LVEF (HR = 0.947, P < 0.001). In the multivariate Cox regression analysis presented in Table 3, both the high SII without AVC group and the high SII with AVC group significantly increased the risk of MACE in the unadjusted model (Model 1) and the age-adjusted model (Model 2). In the fully adjusted model (Model 3), compared to the reference group with low SII and no AVC, individuals with high SII and no AVC had an approximately 1.6-fold increased risk of MACE (HR = 2.605, P = 0.001), while those with high SII and AVC had a significantly increased risk of about 6.5-fold (HR = 7.542, P < 0.001).
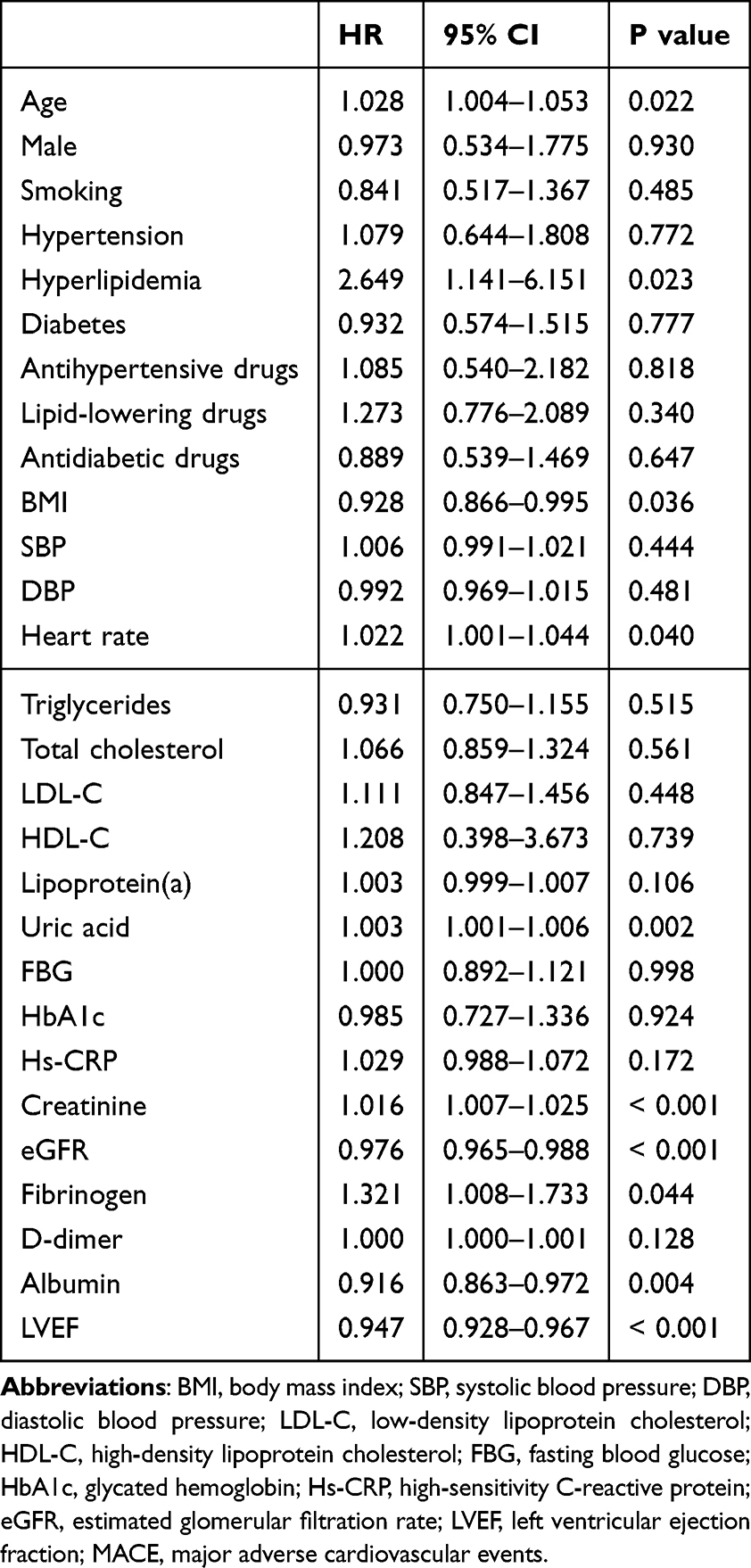 |
Table 2 Univariate Cox Regression Analysis for MACE |
 |
Table 3 Multivariate Cox Regression Analysis of the Association Between the Combination of SII and AVC with MACE |
Subgroup Analysis
Subgroup analysis indicated that (Table 4), compared to the reference group (Low SII+AVC (-)), the MACE risk in the High SII + AVC (-) group was significantly elevated in subgroups of patients over 60 years, males, females, those with hypertension, hyperlipidemia, and those without diabetes (P < 0.05). In contrast, in the Low SII + AVC (+) group, the MACE risk was significantly elevated only among male patients (P < 0.05). Additionally, patients in the High SII + AVC (+) group had a higher MACE risk in all subgroups except for those with diabetes (P < 0.05).
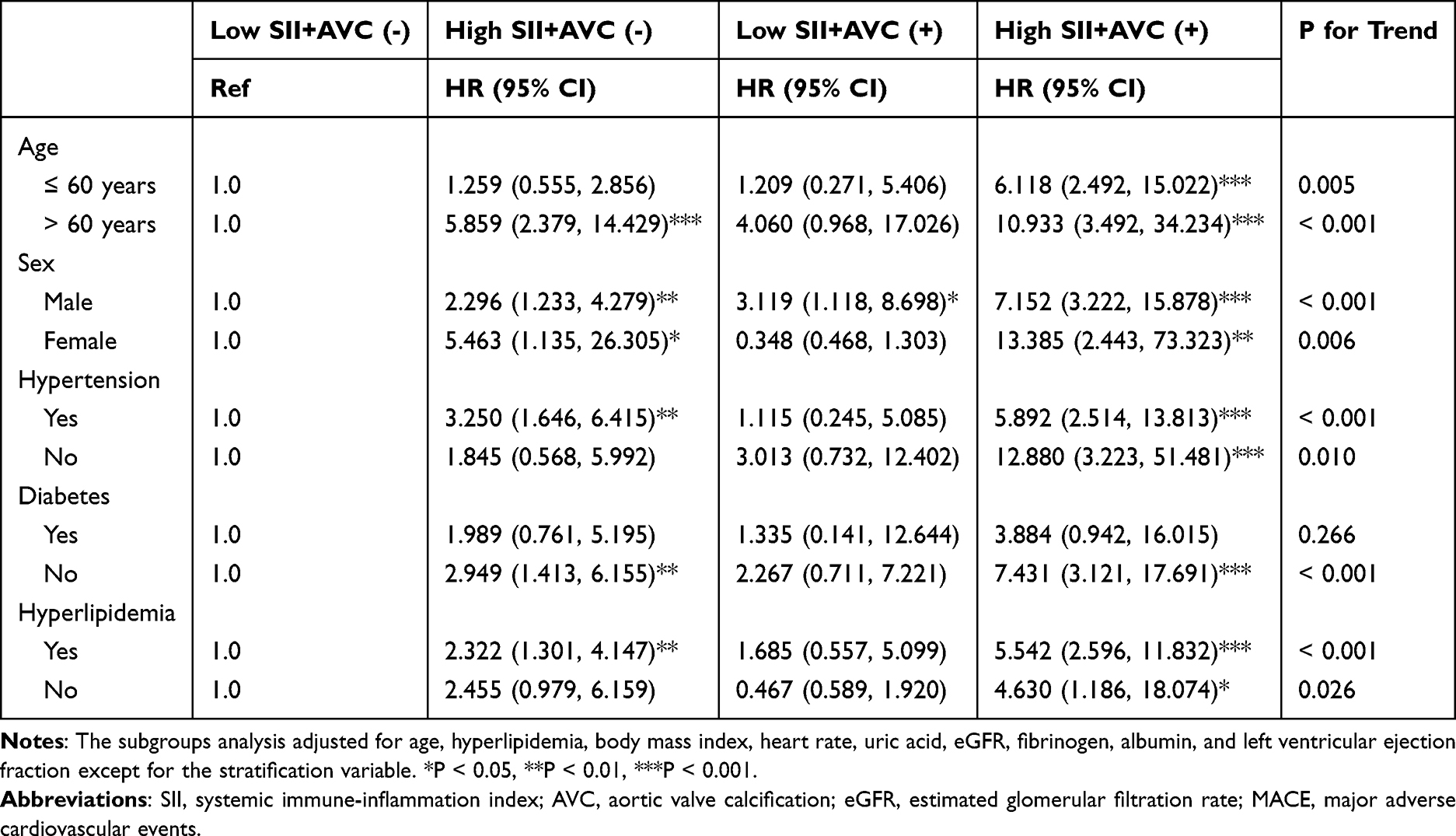 |
Table 4 The Stratified Association Between the Combination of SII and AVC with MACE |
Sensitivity Analysis
As shown in Table 5, after excluding patients with eGFR < 60 mL/min/1.73m², sensitivity analysis adjusted for all confounding factors confirmed that the High SII + AVC (+) group remained significantly associated with an increased risk of MACE (HR: 4.711, 95% CI: 1.967, 11.282, P = 0.001). Additionally, the High SII + AVC (-) group also continued to show a significant association (HR: 2.065, 95% CI: 1.070, 3.984, P = 0.031). Kaplan-Meier survival analysis also showed that patients with both High SII and AVC (+) have the highest risk of MACE, with significant differences in cumulative event rates across all groups (P < 0.001) (Figure 1).
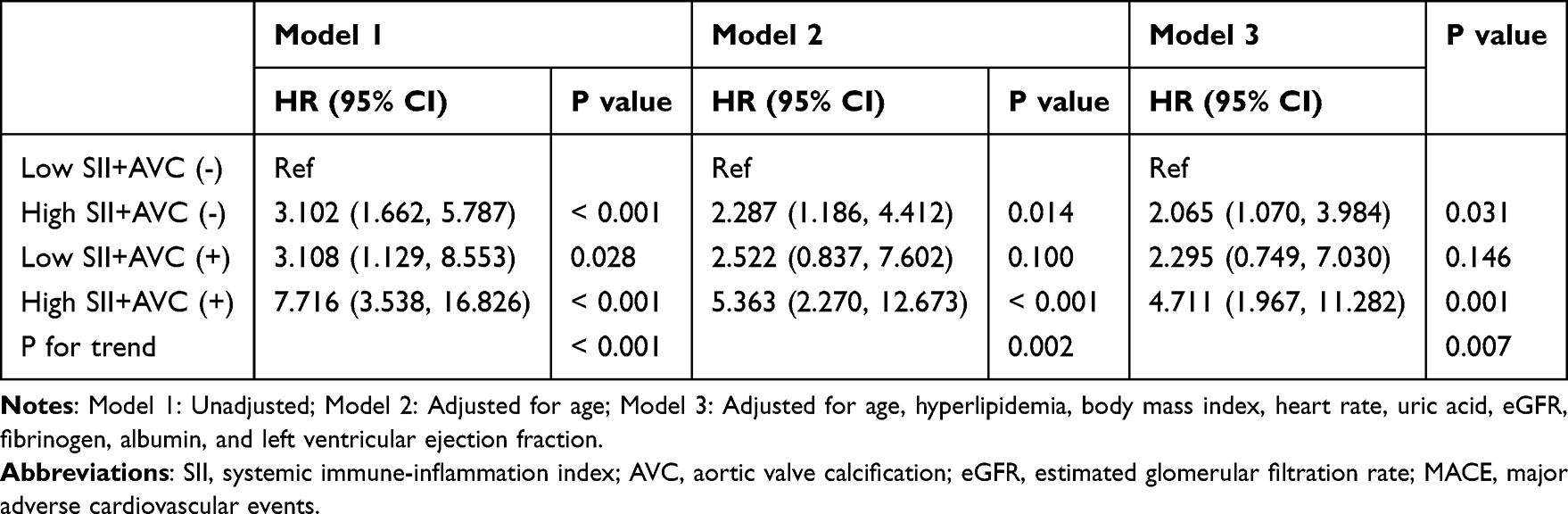 |
Table 5 Multivariate Association Between the Combination of SII and AVC with MACE After Excluding Patients with eGFR < 60 mL/min/1.73m2 |
 |
Figure 1 Kaplan-Meier survival curve for the association between the combination of SII and AVC with MACE. |
Discussion
In this study, we conducted a detailed analysis of the combined effect of the SII and AVC on the risk of MACE in patients with CHD. Multivariable Cox regression analysis revealed that, compared to the reference group (low SII + AVC(-)), the MACE risk was significantly increased by 6.542 times in the high SII + AVC(+) group, and by 1.605 times in the high SII + AVC(-) group. Subgroup analysis further demonstrated the impact of SII and AVC on different patient populations. In the high SII + AVC(-) group, the MACE risk was significantly elevated in patients aged over 60, male, female, hypertensive, hyperlipidemic, and non-diabetic, compared to the reference group. In the low SII + AVC(+) group, only male patients showed a significant increase in MACE risk. In the high SII + AVC(+) group, MACE risk was significantly increased in all subgroups except diabetic patients. Sensitivity analyses also supported the robustness of the main results. After excluding patients with an eGFR of less than 60 mL/min/1.73m2, the MACE risk remained significantly elevated in the high SII + AVC(+) group, and the significant association persisted in the high SII + AVC(-) group. These findings further validate the reliability of the combined SII and AVC as a predictive marker for MACE risk and emphasize the variability in MACE risk assessment across different populations. By jointly assessing SII and AVC, clinicians can more accurately identify high-risk subgroups of CHD patients for MACE. This combined assessment approach not only aids in better understanding individual patient risk levels but also provides a strong basis for developing personalized treatment strategies.
In recent years, residual lipid risk and residual inflammatory risk have been widely utilized in the risk prediction, early screening, and prognostic evaluation of CVD and mortality.15–21 The SII, as an emerging inflammatory marker within the context of residual inflammatory risk, has also been extensively studied in the prognostic evaluation of various CVD.22,23 For instance, several studies have shown that SII is closely associated with the severity of coronary artery disease and the occurrence of adverse cardiovascular events.24–26 Additionally, AVC, as a key marker of atherosclerosis and cardiovascular calcification, has been demonstrated to be significantly associated with the incidence of cardiovascular events.27,28 These studies suggest that both SII and AVC may be independent predictors of cardiovascular events in patients with CHD. However, most existing studies have focused on the prognostic value of a single indicator, and no studies have yet explored the combined effects of SII and AVC. Consequently, these studies may underestimate the actual risk in patients by failing to comprehensively consider the joint impact of SII and AVC. In contrast to previous studies, the innovation of this study lies in its first-time systematic assessment of the combined impact of SII and AVC on the risk of MACE in CHD patients. This not only fills a current research gap but also aids in better predicting the prognosis of CHD patients and provides guidance for the development of individualized treatment strategies.
This study revealed the synergistic effect of the SII and AVC on the risk of MACE in patients with CHD, which may be influenced by the following mechanisms. First, as a marker of systemic inflammatory response, elevated SII typically indicates the progression of atherosclerosis and an increased risk of cardiovascular events.24,25 Inflammation directly contributes to the pathogenesis of atherosclerosis by promoting endothelial damage, lipid deposition, and plaque formation.29,30 On the other hand, AVC is a key feature of atherosclerosis, with calcified plaques leading to valve stiffness and hemodynamic alterations, thereby increasing the burden on the heart.31 Furthermore, studies have shown that the echocardiographic calcium score (eCS) independently predicts cardiac events in patients without known coronary artery disease, with findings indicating that both eCS > 0 and stress-induced ischemia are independent predictors of cardiac events, and outcomes are worse when both are abnormal.32 Similarly, in patients with mild to moderate aortic stenosis, exercise stress echocardiography assessments show that those with an elevated E/e’ ratio (≥ 15) during exercise are at a higher risk of cardiac events, serving as an independent predictor.33 These studies suggest that AVC significantly contributes to the progression of atherosclerosis by increasing cardiac workload, and the use of stress echocardiography further supports this link. Combined with our findings on the synergistic effects of SII and AVC, these results indicate that a multi-level assessment of systemic inflammatory markers and cardiac structural changes can more comprehensively identify high-risk CHD patients, providing a solid basis for early intervention and targeted management. Besides, the synergistic effect of SII and AVC may increase the risk of MACE through multiple pathways. An elevated SII might accelerate the formation of AVC, and the presence of AVC further exacerbates the inflammatory response and cardiac burden, creating a vicious cycle that accelerates the progression of CHD and increases the incidence of cardiovascular events.34–36 Overall, this combination may reflect multiple pathological processes of the disease, exacerbating the prognostic risk for patients.
This study, although it revealed the predictive capability of the SII and AVC for MACE in patients with CHD, had several limitations. Firstly, as a retrospective cohort study, there may be selection bias, and the inherent flaws of this design could affect the generalizability and reliability of the results. Secondly, the assessment of AVC relies on imaging examinations, where measurement errors and inter-observer variability might influence the accuracy of the results. Additionally, while the overall sample size is relatively large, some subgroup analyses may suffer from insufficient sample sizes, limiting the statistical significance of the findings. Lastly, although this study uncovers the association between SII, AVC, and MACE, it does not delve deeply into the specific biological mechanisms. Future research should further explore these mechanisms to gain a more comprehensive understanding of the role of SII and AVC in the occurrence of cardiovascular events.
Conclusions
In conclusion, this study demonstrates that the combined assessment of the SII and AVC can effectively predict the risk of MACE in patients with CHD, indicating significant clinical value. Future research should further explore the application value of SII and AVC in different populations and validate their clinical utility through multicenter, large-sample prospective studies. Additionally, in-depth studies on the mechanisms by which SII and AVC influence MACE will contribute to a better understanding of the pathophysiological processes underlying cardiovascular events, ultimately aiding in the development of more effective interventions.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval and Informed Consent
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. The protocol was reviewed and approved by the Henan Provincial Chest Hospital Ethics Committee. Informed consent was obtained from all participants, or from their legal guardians, prior to inclusion in the study.
Consent for Publication
Not applicable.
Author Contributions
Miaomiao Li and Mengchun Li contributed equally to this work and share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing interests.
References
1. Aminorroaya A, Yoosefi M, Rezaei N. et al. Global, regional, and national quality of care of ischaemic heart disease from 1990 to 2017: a systematic analysis for the Global Burden of Disease Study 2017. Eur J Prev Cardiol. 2022;29(2):371–379. doi:10.1093/eurjpc/zwab066
2. Wang Z, Xiao S, Liu N. Association of lipoprotein(a) with coronary severity in patients with new-onset acute myocardial infarction: a large cross-sectional study. Clin Chim Acta. 2023;540:117220. doi:10.1016/j.cca.2023.117220
3. Wallentin L, Eriksson N, Olszowka M, et al. Plasma proteins associated with cardiovascular death in patients with chronic coronary heart disease: a retrospective study. PLoS Med. 2021;18(1):e1003513. doi:10.1371/journal.pmed.1003513 Published 2021 Jan 13.
4. Wang Z, Li M, Liu N. The nonlinear correlation between lipoprotein (a) and the prevalence of aortic valve calcification in patients with new-onset acute myocardial infarction. Acta Cardiol. 2022;77(10):950–959. doi:10.1080/00015385.2022.2129183
5. Zhao Y, Shao W, Zhu Q, et al. Association between systemic immune-inflammation index and metabolic syndrome and its components: results from the National Health and Nutrition Examination Survey 2011-2016. J Transl Med. 2023;21(1):691. doi:10.1186/s12967-023-04491-y Published 2023 Oct 4.
6. Xie R, Liu X, Wu H, Liu M, Zhang Y. Associations between systemic immune-inflammation index and abdominal aortic calcification: results of a nationwide survey. Nutr, Metab Cardiovasc Dis. 2023;33(7):1437–1443. doi:10.1016/j.numecd.2023.04.015
7. Yang YL, Wu CH, Hsu PF, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
8. Zheng H, Yin Z, Luo X, Zhou Y, Zhang F, Guo Z. Associations between systemic immunity-inflammation index and heart failure: evidence from the NHANES 1999-2018. Int J Cardiol. 2024;395:131400. doi:10.1016/j.ijcard.2023.131400
9. Candemir M, Kiziltunç E, Nurkoç S, Şahinarslan A. Relationship between Systemic Immune-Inflammation Index (SII) and the Severity of Stable Coronary Artery Disease. Angiology. 2021;72(6):575–581. doi:10.1177/0003319720987743
10. Nasir K, Katz R, Al-Mallah M, et al. Relationship of aortic valve calcification with coronary artery calcium severity: the Multi-Ethnic Study of Atherosclerosis (Mesa). J Cardiovasc Comput Tomogr. 2010;4(1):41–46. doi:10.1016/j.jcct.2009.12.002
11. Di Minno MND, Poggio P, Conte E, et al. Cardiovascular morbidity and mortality in patients with aortic valve calcification: a systematic review and meta-analysis. J Cardiovasc Comput Tomogr. 2019;13(4):190–195. doi:10.1016/j.jcct.2019.06.006
12. Dai C, Liu M, Zhou Y, et al. Aortic valve calcification predicts poor outcomes after primary percutaneous coronary intervention. Eur J Clin Invest. 2022;52(10):e13828. doi:10.1111/eci.13828
13. Moncla LM, Briend M, Bossé Y, Mathieu P. Calcific aortic valve disease: mechanisms, prevention and treatment. Nat Rev Cardiol. 2023;20(8):546–559. doi:10.1038/s41569-023-00845-7
14. Fihn SD, Blankenship JC, Alexander KP, et al. ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64(18):1929–1949. doi:10.1016/j.jacc.2014.07.017
15. Wang ZW, Li M, Li JJ, Liu NF. Association of lipoprotein(a) with all-cause and cause-specific mortality: a prospective cohort study. Eur J Intern Med. 2022;106:63–70. doi:10.1016/j.ejim.2022.09.010
16. Hoogeveen RC, Ballantyne CM. Residual Cardiovascular Risk at Low LDL: remnants, Lipoprotein(a), and Inflammation. Clin Chem. 2021;67(1):143–153. doi:10.1093/clinchem/hvaa252
17. Wang ZW, Xiao SJ, Liu NF. Association of lipoprotein(a) with left ventricular hypertrophy in patients with new-onset acute myocardial infarction: a large cross-sectional study. Clin Chim Acta. 2023;540:117226. doi:10.1016/j.cca.2023.117226
18. Ridker PM, Bhatt DL, Pradhan AD, et al. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lancet. 2023;401(10384):1293–1301. doi:10.1016/S0140-6736(23)00215-5
19. Wang Z, Yan X, Fang L, Tang J, Zhang J. Association between lipoprotein(a), fibrinogen and their combination with all-cause, cardiovascular disease and cancer-related mortality: findings from the NHANES. BMC Public Health. 2024;24(1):1927. doi:10.1186/s12889-024-19443-4 Published 2024 Jul 18.
20. Han L, Zhang L, Hu W, Lu Y, Wang Z. Association of C-reactive protein with all-cause and cause-specific mortality in people with gout. Eur J Med Res. 2024;29(1):320. doi:10.1186/s40001-024-01923-3 Published 2024 Jun 10.
21. Wang Z, Tang J, Shi Q, Fang L, Liu N, Zhang J. Synergistic effect of lipoprotein(a) and high-sensitivity C-reactive protein on the risk of all-cause and cardiovascular death in patients with acute myocardial infarction: a large prospective cohort study. Front Endocrinol (Lausanne). 2024;15:1392859. doi:10.3389/fendo.2024.1392859 Published 2024 May 15.
22. Zhao Z, Zhang X, Sun T, et al. Prognostic value of systemic immune-inflammation index in CAD patients: systematic review and meta-analyses. Eur J Clin Invest. 2024;54(2):e14100. doi:10.1111/eci.14100
23. Zhang C, Li M, Liu L, et al. Systemic immune-inflammation index as a novel predictor of major adverse cardiovascular events in patients undergoing percutaneous coronary intervention: a meta-analysis of cohort studies. BMC Cardiovasc Disord. 2024;24(1):189. doi:10.1186/s12872-024-03849-4 Published 2024 Apr 1.
24. Wang W, Guo XL, Qiu XP, Yu YJ, Tu M. Systemic immune-inflammation index mediates the association between metabolic dysfunction-associated fatty liver disease and sub-clinical carotid atherosclerosis: a mediation analysis. Front Endocrinol (Lausanne). 2024;15:1406793. doi:10.3389/fendo.2024.1406793 Published 2024 Jun 18.
25. Liu Y, Ye T, Chen L, et al. Systemic immune-inflammation index predicts the severity of coronary stenosis in patients with coronary heart disease. Coron Artery Dis. 2021;32(8):715–720. doi:10.1097/MCA.0000000000001037
26. Luo J, Qin X, Zhang X, et al. Prognostic implications of systemic immune-inflammation index in myocardial infarction patients with and without diabetes: insights from the NOAFCAMI-SH registry. Cardiovasc Diabetol. 2024;23(1):41. doi:10.1186/s12933-024-02129-x Published 2024 Jan 22.
27. Ye Z, Scott CG, Gajjar RA, et al. Prognostic value of aortic valve calcification in nonsevere aortic stenosis with preserved ejection fraction. Eur Heart J Cardiovasc Imaging. 2024:jeae145. doi:10.1093/ehjci/jeae145.Published online June 4, 2024.
28. Moore MK, Jones GT, Whalley G, Prendergast B, Williams MJA, Coffey S. Outcomes of patients with early calcific aortic valve disease detected by clinically indicated echocardiography. Eur Heart J Cardiovasc Imaging. 2024;25(3):356–364. doi:10.1093/ehjci/jead259
29. Kong P, Cui ZY, Huang XF, Zhang DD, Guo RJ, Han M. Inflammation and atherosclerosis: signaling pathways and therapeutic intervention. Signal Transduct Target Ther. 2022;7(1):131. doi:10.1038/s41392-022-00955-7 Published 2022 Apr 22.
30. Wolf D, Ley K. Immunity and Inflammation in Atherosclerosis. Circ Res. 2019;124(2):315–327. doi:10.1161/CIRCRESAHA.118.313591
31. Pawade T, Sheth T, Guzzetti E, Dweck MR, Clavel MA. Why and how to measure aortic valve calcification in patients with aortic stenosis. JACC Cardiovasc Imaging. 2019;12(9):1835–1848. doi:10.1016/j.jcmg.2019.01.045
32. Gaibazzi N, Porter TR, Agricola E, et al. Prognostic value of echocardiographic calcium score in patients with a clinical indication for stress echocardiography. JACC Cardiovasc Imaging. 2015;8(4):389–396. doi:10.1016/j.jcmg.2014.10.014
33. Sonaglioni A, Lombardo M, Baravelli M, Trotta G, Sommese C, Anzà C. Exercise stress echocardiography with tissue Doppler imaging in risk stratification of mild to moderate aortic stenosis. Int J Cardiovasc Imaging. 2015;31(8):1519–1527. doi:10.1007/s10554-015-0724-9
34. Erdoğan M, Öztürk S, Kardeşler B, et al. The relationship between calcific severe aortic stenosis and systemic immune-inflammation index. Echocardiography. 2021;38(5):737–744. doi:10.1111/echo.15044
35. Yoon D, Choi B, Kim JE, et al. Autotaxin inhibition attenuates the aortic valve calcification by suppressing inflammation-driven fibro-calcific remodeling of valvular interstitial cells [published correction appears in BMC Med. 2024 Apr 29;22(1):178. doi: 10.1186/s12916-024-03403-1]. BMC Med. 2024;22(1):122. doi:10.1186/s12916-024-03342-x Published 2024 Mar 14.
36. Abdelbaky A, Corsini E, Figueroa AL, et al. Early aortic valve inflammation precedes calcification: a longitudinal FDG-PET/CT study. Atherosclerosis. 2015;238(2):165–172. doi:10.1016/j.atherosclerosis.2014.11.026
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Machine Learning Model Integrating Tongue Image Features and Myocardial Injury Markers Predicts Major Adverse Cardiovascular Events in Patients with Coronary Heart Disease
Zhou M, Li J, Lim J, Xiao X, Xia Y, Wang Q, Xu Z
International Journal of General Medicine 2025, 18:3739-3765
Published Date: 5 July 2025