")
Back to Journals » Journal of Inflammation Research » Volume 17
The Correlation Between Uric Acid, Urinary Protein and Umbilical Artery Blood Flow Related Parameters and Maternal and Infant Prognosis in Patients with Gestational Hypertension
Received 15 July 2024
Accepted for publication 2 November 2024
Published 9 December 2024 Volume 2024:17 Pages 10651—10661
DOI https://doi.org/10.2147/JIR.S476334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Mingxing Yan, Jinji Wang, Liying Li
Fujian Maternity and Child Health Hospital, Fujian Medical University, Fuzhou, 350000, People’s Republic of China
Correspondence: Liying Li, Fujian Maternity and Child Health Hospital, Fujian Medical University, 18 Daoshan Road, Gulou District, Fuzhou, 350000, People’s Republic of China, Tel +86-0591-87279624, Email [email protected]
Objective: To investigate the correlation between uric acid (UA), urinary protein (UP) and umbilical artery blood flow related parameters and maternal and infant prognosis in patients with hypertensive disorder complicating pregnancy (HDP).
Methods: A total of 110 hDP patients who underwent prenatal examination and delivered in our hospital from June 2018 to May 2023 were selected as the HDP group. According to the prognosis of mother and infant, they were divided into normal prognosis group (n=80) and poor prognosis group (n=30). In addition, 110 healthy pregnant women who received prenatal examination in the same hospital during the same period were randomly selected as healthy control group. The maternal and infant outcomes, UA, 24-h-UP level, umbilical artery blood flow pulsation index (PI), resistance index (RI) and systolic and diastolic blood flow velocity ratio (S/D) were compared between the two groups. Logistic regression analysis was used to analyze the factors related to the above probability and maternal and infant prognosis.
Results: The total incidence of adverse maternal and infants outcome in the HDP group was higher than that of HC (37.5% VS16.65%) (P < 0.05). The HDP group UA, 24-h-UP and PI, RI, and S / D higher than HC (P < 0.05). Logistic regression analysis shows that the age of pregnant women and 24-h-UP, PI, RI, S / D are related factors that affect the prognosis of adverse maternal and infants outcome (P < 0.05).
Conclusion: The UA and UP levels and umbilical artery blood flow-related parameters in HDP patients were significantly increased. Maternal age and 24-h-UP, RI, and S/D are all relevant factors that affect the adverse maternal and fetal prognosis of HDP patients.
Keywords: uric acid, urinary protein, umbilical artery blood flow, pregnancy-induced hypertension
Introduction
Hypertensive disorder of pregnancy (HDP) is a systemic disease unique to pregnant women, mainly characterized by hypertension, edema and proteinuria. HDP seriously threatens the health and life of mother and child and is one of the common obstetric diseases. At present, pregnancy-induced hypertension is summarized into four categories: preeclampsia-eclampsia syndrome, chronic hypertension, chronic hypertension superimposed preeclampsia, and gestational hypertension. The above conditions may cause complications such as heart disease, kidney damage, cerebral hemorrhage, and abnormal coagulation function.1,2 One of the complications is obstruction of umbilical cord blood flow, which may lead to neonatal hypoxic-ischemic encephalopathy or intrauterine distress, resulting in adverse perinatal outcomes.3 In the past, 24-h urine protein (24-h-UP) quantification was used as a measure of renal injury, but this indicator has major limitations. On the one hand, it is affected by subjective factors such as the patient’s diet and exercise. On the other hand, the prediction of kidney damage has a lag that cannot be ignored, which is not conducive to early disease intervention.4 Therefore, finding reliable prognostic predictors has important clinical significance for patients with hypertensive disorders during pregnancy.
Uric acid is produced by the breakdown of purines and is excreted through the kidneys. A normal body has a balance between the production and excretion of uric acid. The imbalance of HDP uric acid metabolism leads to an increase in uric acid. The mechanism of HDP is mainly divided into two stages. The first stage is the preclinical stage, which is the disorder of trophoblast remodeling in the uterine spiral arteries in early pregnancy, leading to placental ischemia and hypoxia, and the release of a variety of placental factors. In the second stage, placental factors enter the maternal blood circulation and promote the activation of systemic inflammatory response and damage to vascular endothelial cells, causing a variety of clinical manifestations. At the same time, placental factors enter the blood, promote inflammatory response, and cause damage to vascular endothelial cells. Cell damage and hypoxia lead to increased glycolysis and increased lactic acid production, which competitively inhibits the acid excretion ability of the proximal renal tubules and reduces uric acid excretion.5 Studies have shown6 that elevated blood uric acid levels in early pregnancy are related to HDP and can predict the occurrence of HDP.
In the past, renal function was reflected clinically through creatinine and urea, but glomeruli have substantial functional reserves. Creatinine and urea only increase significantly when the glomerular filtration rate reaches below 50%.7 The levels of creatinine and urea are easily affected by age, gender, muscle mass, blood lipids, inflammation, etc. Some literature shows that8 the occurrence of preeclampsia is positively correlated with the increase in cholesterol in blood lipids. Blood lipid peroxides cause endothelial cell damage, lead to atherosclerosis, form thrombus, affect placental vascular function, thereby increasing the risk of HDP.9
The pathophysiological mechanism of HDP is systemic arteriolar spasm. Hemodynamic monitoring is often performed on such patients to determine the intrauterine status of the fetus. Determining the timing of pregnancy termination can be a challenge in patients with fetal hemodynamic abnormalities. Gestational age is the main determinant of premature neonatal death (death within 28 days of birth), and neonatal mortality increases significantly with decreasing gestational age.10 However, continued prolongation of gestational age conflicts with fetal intrauterine hypoxia, which may delay treatment and affect pregnancy outcomes. Clinically, domestic and foreign studies mostly describe the gestational weeks, neonatal admission rates and the incidence of certain diseases in childhood in such patients. It is very important to study the significance of changes in fetal hemodynamic parameters.
Therefore, early preventive screening and diagnostic intervention for HDP using various monitoring indicators can effectively avoid the occurrence of various adverse maternal and infant prognosis caused by the disease, and is of great significance in improving the pregnancy outcomes of HDP patients.11,12 Uric acid (UA) is mainly excreted through various transporters in renal tissue, and is often used together with 24-h-UP quantitative detection for clinical assessment of early renal injury and severity.13 Umbilical artery blood flow is an important factor affecting uteroplacental circulation. It can assess fetal intrauterine hypoxia and HDP syndrome tendencies, which is beneficial to promoting prenatal and postnatal care.14 Previous studies have reported the correlation between UA and albumin and the severity of HDP.15 However, there are currently relatively few reports on the correlation between UA, UP and umbilical artery blood flow-related parameters and maternal and fetal prognosis in HDP patients. This study mainly explores and analyzes the changes in UA, UP and umbilical artery blood flow-related parameters in patients with HDP and their relationship with maternal and fetal prognosis, aiming to provide a theoretical basis for the clinical diagnosis and treatment of HDP.
Information and Methods
Normal Information
A total of 110 hDP patients who underwent antenatal examination and delivery in our hospital from June 2018 to May 2023 were selected as the HDP group. They were divided into a normal prognosis group (n=80) and a adverse prognosis group (n=30) according to the maternal and infant prognosis. Among them, adverse outcomes were defined as: fetal growth restriction, intrauterine distress, postpartum haemorrhage, placental abruption, neonatal asphyxia or macrosomia. Normal outcome was defined as: If the mother and fetus are healthy.In addition, 110 healthy pregnant women who underwent prenatal examination in the same hospital during the same period were randomly selected as the healthy control (HC) group.
Inclusion Criteria
(1) Meets HDP diagnostic criteria: After 20 weeks of pregnancy, systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg (1 mmHg=0.133 kPa). And accompanied by any of the following: urine protein ≥0.3 g/24 h, or urine protein/creatinine ratio ≥0.3, or random urine protein ≥ (+). No proteinuria but accompanied by any of the following organs or systems involved, including damage to important organs such as the heart, lungs, liver, and kidneys, abnormal changes in the blood system, digestive system, and nervous system, and placenta and fetal involvement.16
(2) Natural conception and singleton pregnancy.
(3) Complete clinical data.
Exclusion Criteria
(1) Essential hypertension.
(2) Combined with diabetes and chronic nephritis.
(3) Have a history of urinary tract infection in the past.
(4) Combined with other pregnancy complications.
(5) Multiple pregnancy.
(6) Suffering from other diseases that cause blood pressure to rise.
Treatment Method
The 110 hDP patients included all received routine HDP treatment and nursing measures.17 Including antispasmodic, antihypertensive, sedative and diuretic support and symptomatic treatment. Strictly prevent eclampsia and complications. The patient is urged to rest in the left lateral decubitus position, which can relieve venous compression of the lower limbs. Uterine artery perfusion was maintained, and diazepam 5 mg was administered at bedtime to maintain sedation. Administer oxygen intermittently and closely monitor the status of mother and child. Oral treatment was given with labetalol tablets (Jiangsu Desano Pharmaceutical Co., Ltd., national drug approval number H32026119, specification: 100 mg), 100 mg/time, 2 times/d.
Determination of Indicates
The age, parity, and pre-pregnancy body mass index (BMI) of the research subjects were collected. Family history of maternal hypertension and serum UA, 24-h-UP levels and umbilical artery blood flow pulsatility index (PI) after 12 weeks of pregnancy. Umbilical artery blood flow parameters such as resistance index (RI) and systolic to diastolic flow velocity ratio (S/D). The follow-up period will be until the end of the patient’s pregnancy, as of May 2023. If the pregnancy ends with fetal growth restriction, intrauterine distress, postpartum hemorrhage, placental abruption, neonatal asphyxia or macrosomia, the prognosis for maternal and neonatal is adverse. If the mother and fetus are healthy, the prognosis for maternal and neonatal is normal.
Statistical Analysis
The data were analyzed by SPSS21.0. Measurement data were measured using t-test and expressed as mean ± standard deviation (x ± s). Count data were analyzed using χ2 test and expressed as frequency (percentage) [n (%)]. The data that does not meet the normal distribution is tested by non -parameters. Pairwise comparison was carried out by LSD method, and the correlation coefficient was obtained by linear regression analysis.
Results
Comparison of Clinical Data
We compared general maternal clinical data between groups (Table 1). The results showed that the two groups were comparable in age, pre-pregnancy BMI, parity and gestational age (P>0.05).
 |
Table 1 Comparison of General Clinical Data of Patients |
Comparison of Adverse Maternal and Infant Outcomes Between HDP Group and HC Group
We tracked the adverse maternal and infant prognosis of the two groups of mothers (Table 2 and Figure 1). As of May 30, 2023, 30 of the 80 patients with HDP (37.5%) had a prognosis of adverse maternal and infants outcome (37.5%). The number of fetal growth in the two groups, fetal growth restriction, fetal distress, postpartum bleeding, placental abruption, neonatal asphyxia, and fetal macrosomia are shown in Table 2 for specific details. The total incidence of adverse maternal and infants outcome in the HDP group was higher than that of HC (37.5% vs16.65%) (P <0.05).
 |
Table 2 Comparison of Each Index Among 2 Groups [n(%)] |
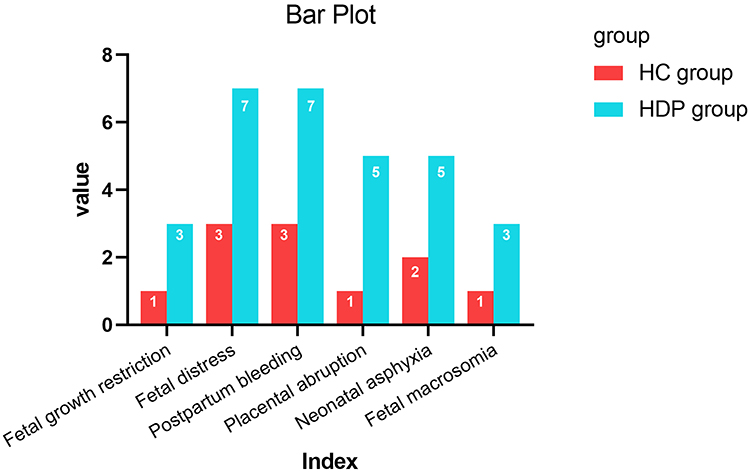 |
Figure 1 Comparison of each index among 2 groups. |
Comparison of the Two Groups of UA, 24-h-UP Levels and Umbilical Artery Blood Flow Parameters
We also compare the levels of UA and 24-h-UP and umbilical artery blood flow parameters of the two groups of puerperas. The results showed (Table 3 and Figure 2) that HDP group UA, 24-h-UP levels and PI, RI, S / D are higher than HC group and p<0.05.
 |
Table 3 Comparison of the Two Groups of UA, 24HPRO Levels and Umbilical Artery Blood Flow Parameters (x ± s) |
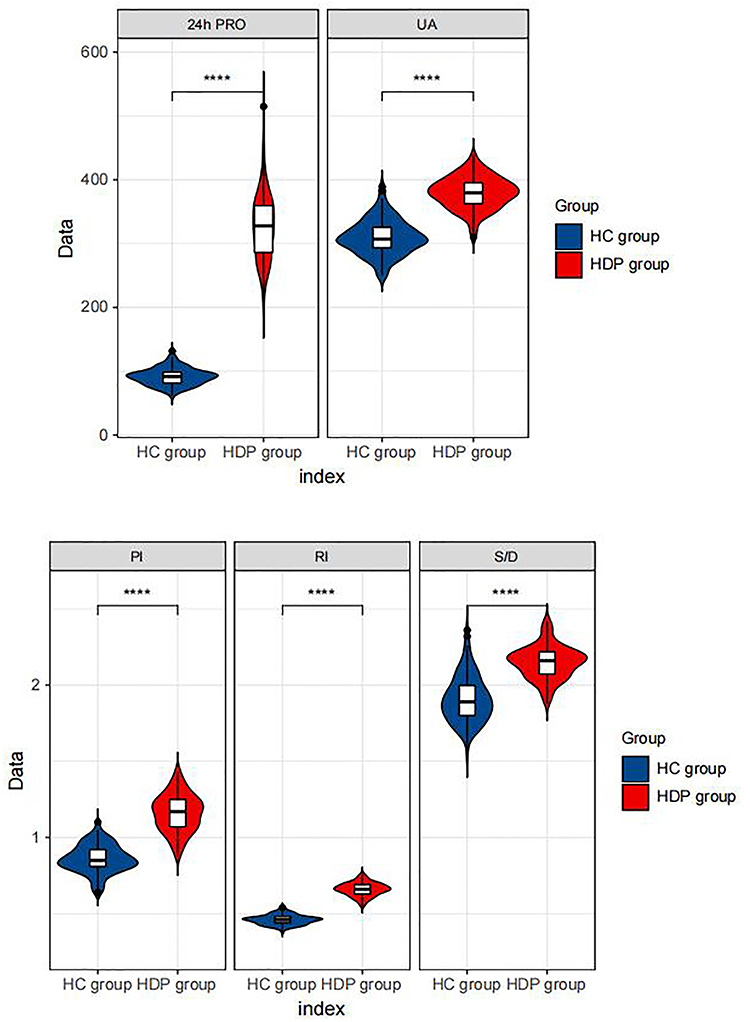 |
Figure 2 Violin plot for Comparison of the two groups of UA, 24HPRO levels and umbilical artery blood flow parameters, **** represents P<0.001. |
Analysis of Single Factors Affecting Maternal and Neonatal Outcome of HDP Patients
The prognosis of adverse maternal and infants outcome in HDP patients is related to the age of pregnant women, BMI before pregnancy, family history of hypertension and UA, 24-h-UP level, and PI, RI, S/D (P <0.05) (Table 4).
 |
Table 4 Analysis of Single Factors Affecting Maternal and Neonatal Outcome of HDP Patients [n(%)], (x ± s) |
Logistic Regression Analysis That Affects the Prognosis of HDP Maternal and Neonatal
Taking maternal and infant prognosis as the outcome variable, we set relevant assignments (Table 5). Then perform logistic analysis. The results showed that maternal age (OR=2.066, P<0.05), 24-h-UP (OR=1.882, P<0.05), PI (OR=2.045, P<0.05), RI (OR=2.315, P<0.05) and S/ D (OR=2.741, P<0.05) is a relevant factor affecting adverse maternal and infant prognosis in patients with HDP.
 |
Table 5 Set Relevant Assignments of the Factors |
Discussion
Hypertension is the most common medical disease during pregnancy, accounting for 5% to 10% of all pregnancies. Maternal age over 40, pre pregnancy obesity, excessive weight gain during pregnancy and pregnancy diabetes are all related to the increased risk of maternal hypertension.18 HDP often leads to reduced maternal renal tubular reabsorption capacity, resulting in abnormal UA and 24-h-UP, causing placental hypoperfusion and ischemia and hypoxia, adversely affecting maternal and fetal prognosis.19 Although there are differences between subtypes of HDP, Veerbeek et al’s study20 suggests that all types of HDP appear to be associated with high risk. According to reports, gestational hypertension can increase the risk of future chronic hypertension, cardiovascular disease, coronary heart disease, and heart failure.21,22
Urinary microalbumin is a negatively charged macromolecule protein that cannot pass through the glomerular filtration membrane. Therefore, trace amounts are present in the urine of healthy people. When renal parenchymal damage or capillary permeability increases due to various reasons, urinary microalbumin may enter the urine through the glomerular filtration membrane. Some scholars have pointed out in the past that during renal injury, changes in urinary microalbumin occur earlier than 24-h urine protein quantification.23,24
The supply of nutrients and the elimination of metabolites required for fetal growth require the blood circulation of the umbilical cord to be completed. Stable blood perfusion is the basis for ensuring healthy fetal development.25 During pregnancy, the uterine blood flow velocity gradually increases from the original 50 mL/min to 500 ~ 750 mL/min. Accompanied by the orderly remodeling of the branches of the uterine arteries at all levels, the uterine cavity is enlarged and the elasticity is reduced. To maintain a stable high flow velocity and low resistance state of the umbilical artery to meet the needs of fetal growth and development. This process is completed with the help of trophoblast cells and can continue until 37 weeks of pregnancy. In patients with gestational hypertension, arterial remodeling is hindered due to trophoblast damage, and the extent of remodeling in some patients is limited to the decidual segment. This causes the umbilical artery resistance of pregnant women to increase and the flow velocity to decrease, which has been confirmed by domestic and foreign scholars.26,27
The increase in uric acid levels indicates an increase in adverse pregnancy outcomes. Studies28,29 have shown that high uric acid levels during pregnancy are related to adverse pregnancy and childbirth outcomes, and high uric acid levels are an independent risk factor for delivery of low-birth-weight babies. Literature reports30 When the uric acid content is >400 μ mol/L, the incidence of intrauterine growth retardation is 46.92%, and perinatal mortality is significantly increased.
HDP found that blood uric acid concentration increased at 10 weeks of pregnancy, and in vitro experiments suggested31 that high concentrations of uric acid inhibit the apoptosis of uterine spiral artery smooth muscle cells and endothelial cells. Interfering with changes in extravillous trophoblast cells within blood vessels, leading to impairment of uterine spiral artery remodeling. Uric acid can initiate an immune response and lead to an inflammatory response at the maternal-fetal interface.32 Uric acid produces oxygen free radicals that affect trophoblast function and lead to shallow placental implantation.33 It causes placental ischemia and hypoxia, which leads to restriction of maternal-fetal interface exchange, affects intrauterine growth and development of the fetus, and leads to an increase in adverse pregnancy outcomes such as fetal distress, FGR, premature birth, and placental abruption.
Therefore, using simple and highly sensitive indicators to conduct early assessment of maternal and infant prognosis in HDP patients is beneficial to the formulation and implementation of clinical treatment decisions, and is of great significance in preventing and treating adverse maternal and infant outcomes. PI and RI are commonly used in clinical practice as the main parameters of placental hemodynamics and are closely associated with the risk of gestational hypertension.34,35 Doppler derived vascular patterns are closely associated with normal and adverse perinatal outcomes, and the description of uterine and umbilical S/D ratios should be included as part of the clinical evaluation of all hypertensive pregnant women.36
The results of this study show that the total incidence of adverse maternal and infants outcome in the HDP group is higher than that of HC (37.5% VS16.65%). UA, 24-h-UP levels and PI, RI, S / D are significantly higher than the HC group. Research with37 is basically the same. It shows that patients with HDP are manifested as abnormal renal function, abnormal umbilical artery blood flow parameters, and the incidence of adverse maternal and infants outcome is higher. Significant increases in systolic and diastolic blood pressure in HDP patients cause systemic small vessel spasm, reduce renal blood flow, and significantly increase UA and 24-h-UP levels.38 High UA can cause oxidative stress disorders in pregnant women, causing serious damage to vascular endothelial function and placental implantation and perfusion, inhibiting fetal growth and development, and increasing the risk of adverse pregnancy outcomes.39 Placental blood flow with high blood flow and low impedance is the key to ensuring the normal exchange of nutrients and metabolites during fetal growth and development, and can maintain normal fetal growth and development through blood perfusion in the placental villous space.40 The increased distal vascular pressure in HDP patients causes abnormal umbilical artery blood flow, which is manifested in that umbilical artery blood flow parameters such as PI, RI, and S/D are higher than those in normal pregnancies.41 Abnormal placental blood perfusion leads to fetal ischemia and hypoxia, increasing the incidence of adverse pregnancy outcomes. In this study, the return analysis of the LOGISTIC regression showed that age and 24-h-UP, PI, RI, S / D are related factors that affect the adverse maternal and neonatal in patients with HDP. Similar to the results of the42 research results. This shows that UA, UP levels, and PI, RI, S / D have a good predictive effect on the prognosis of adverse mother and infants in patients with HDP.
The limitation of this study is that there was no follow-up analysis of the long-term prognosis of neonates with UA, UP levels and umbilical artery blood flow-related parameters in HDP patients, and further in-depth research and verification with extended observation time are still needed. The clinical sample size is insufficient to serve as a practical reference value. A larger sample size is needed to conduct the experiment. The number of measurements of umbilical artery blood flow, UA, and 24-h-UP was less than three times. We have not yet analyzed the impact of gestational age on the research results. More detailed research is needed in the future. It aims to avoid risk factors in the future or prevent adverse reactions in maternal and infant prognosis in advance. Provide a solid foundation for clinical targeted therapy.
In summary, UA, UP levels and umbilical artery blood flow-related parameters were significantly increased in patients with HDP. Maternal age and 24-h-UP, RI, and S/D are related factors that affect adverse maternal and infant prognosis in HDP patients. The monitoring and evaluation of these parameters may help reduce the risk of adverse outcomes for both mother and infant.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Fujian Maternity and Child Health Hospital (No. 2023KY194). Written informed consent was obtained from all participants.
Funding
Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics Gynecology and Pediatrics Fujian Medical University. Fujian Clinical Research Center for Maternal-fetal Medicine. National Key Obstetric Clinical Specialty Construction Institution of China. Innovation Platform Project of Science and Technology, Fujian province (2021Y2012) National Key Clinical Specialty Construction Program of China (Obstetric).
Disclosure
The authors declare no conflict of interest.
References
1. Hou LH. The significance of ambulatory blood pressure monitoring during pregnancy in predicting the outcome of hypertensive disorders in pregnancy. J Clin Ration Drug Use. 2018;11(04):53–54+57.
2. Wang L, Wang YL. Application of combined detection of CysC, HCY and mALB in the early diagnosis of patients with renal function damage due to hypertension during pregnancy. Chin Maternal Child Health Res. 2017;28(12):1675–1677.
3. Holmquist E, Brantsæter AL, Meltzer HM, et al. Maternal selenium intake and selenium status during pregnancy in relation to preeclampsia and pregnancy-induced hypertension in a large Norwegian Pregnancy Cohort Study. Sci Total Environ. 2021;1(798):149271. doi:10.1016/j.scitotenv.2021.149271
4. Gui Y. The value of serum cystatin C and urinary microalbumin in early diagnosis of hypertensive disease during pregnancy. Chin Maternal Child Health Care. 2017;32(04):709–711.
5. Yokokawa H, Fukuda H, Suzuki A, et al. Association Between Serum Uric Acid Levels/Hyperuricemia and Hypertension Among 85,286 Japanese Workers. J Clin Hypertens. 2016;18(1):53–59. doi:10.1111/jch.12627
6. Zhao Y, Zhao Y, Fan K, et al. Serum uric acid in early pregnancy and risk of gestational diabetes mellitus: a cohort study of 85,609 pregnant women. Diabetes Metab. 2022;48(3):101293. doi:10.1016/j.diabet.2021.101293
7. Lu DH, Shi ZY, Wang YN. Clinical significance of serum cholesterol, total bilirubin, uric acid and urinary microprotein in patients with gestational diabetes. China Maternal Child Health Care. 2015;30(07):1034–1036.
8. Retnakaran R, Shah BR. The adverse cardiovascular risk factor profile of women with pre-eclampsia develops over time in the years before pregnancy. BJOG. 2022;129(9):1512–1520. doi:10.1111/1471-0528.17084
9. Hart PMB, Stephenson NL, Scime NV, et al. Second trimester cytokine profiles associated with gestational diabetes and hypertensive disorders of pregnancy. PLoS One. 2022;17(12):e0279072. doi:10.1371/journal.pone.0279072
10. Cnattingius S, Johansson S, Razaz N. Apgar Score and Risk of Neonatal Death among Preterm Infants. N Engl J Med. 2020;383(1):49–57. doi:10.1056/NEJMoa1915075
11. Benschop L, Duvekot JJ, Roeters Van Lennep JE. Future risk of cardiovascular disease risk factors and events in women after a hypertensive disorder of pregnancy. Heart. 2019;105(16):1273–1278. doi:10.1136/heartjnl-2018-313453
12. Kamińska J, Dymicka-Piekarska V, Tomaszewska J, et al. Diagnostic utility of protein to creatinine ratio (P/C ratio) in spot urine sample within routine clinical practice. Crit Rev Clin Lab Sci. 2020;57(5):345–364. doi:10.1080/10408363.2020.1723487
13. Shapiro J, Ray JG, McArthur E, et al. Risk of Acute Kidney Injury After Hypertensive Disorders of Pregnancy: a Population-Based Cohort Study. Am J Kidney Dis. 2022;79(4):561–569. doi:10.1053/j.ajkd.2021.07.017
14. Li WT. Analysis of fetal umbilical artery hemodynamics and neonatal related indicators in pregnant women with hypertensive disease during pregnancy. China Maternal Child Health Care. 2020;35(04):674–677.
15. Xu YY. Correlation analysis between serum uric acid and albumin levels and the severity of hypertensive disease during pregnancy. Air Force Medl J. 2019;35(02):143–145+163.
16. HDP subgroup. Chinese Society of Obstetrics and Gynecology CMA. Guidelines for diagnosis and treatment of hypertension during pregnancy (2015). Honghua Obstet Gynecol J. 2020;50:721–728.
17. Hypertension in pregnancy group of the Obstetrics and Gynecology Branch of the Chinese Medical Association. Chinese expert consensus on blood pressure management during pregnancy (2021). Chin J ObstetrGynecol. 2021;2021:737–745.
18. Khedagi AM, Bello NA. Hypertensive Disorders of Pregnancy. Cardiol Clin. 2021;39(1):77–90. doi:10.1016/j.ccl.2020.09.005
19. Magee LA, Smith GN, Bloch C, et al. Guideline No. 426: hypertensive Disorders of Pregnancy: diagnosis, Prediction, Prevention, and Management. J Obstet Gynaecol Canada. 2022;44(5):547–571. doi:10.1016/j.jogc.2022.03.002
20. Veerbeek JH, Hermes W, Breimer AY, et al. Cardiovascular disease risk factors after early-onset preeclampsia, late-onset preeclampsia, and pregnancy-induced hypertension. Hypertension. 2015;65(3):600–606. doi:10.1161/HYPERTENSIONAHA.114.04850
21. Watanabe M, Sairenchi T, Nishida K, et al. Gestational hypertension as risk factor of hypertension in middle-aged and older women. Int J Environ Res Public Health. 2020;17(11):4052. doi:10.3390/ijerph17114052
22. CCW L, ACQ L, Leow SH, et al. Future cardiovascular disease risk for women with gestational hypertension: a systematic review and meta-analysis. J Am Heart Assoc. 2020;9(13):e013991. doi:10.1161/JAHA.119.013991
23. Ayansina D, Black C, Hall SJ, et al. Long term effects of gestational hypertension and pre-eclampsia on kidney function: record linkage study. Pregnancy Hypertens. 2016;6(4):344–349. doi:10.1016/j.preghy.2016.08.231
24. Yan Q, Wang H, Liu R, et al. Influence of random urine albumin-creatinine ratio of pregnant women with hypertension during the gestation period on perinatal outcome. Exp Ther Med. 2016;12(4):2521–2526. doi:10.3892/etm.2016.3620
25. Gupta S, Chauhan M, Sen J, et al. Effect of Transdermal Nitroglycerine on Doppler Velocity Waveforms of the Uterine, Umbilical and Fetal Middle Cerebral Arteries in Patients with Chronic Placental Insufficiency: a Prospective RCT. J Clin Diagn Res. 2017;11(7):QC13–QC17. doi:10.7860/JCDR/2017/21438.10282
26. Ma B, Wang YX, Li TG. The value of three-dimensional power Doppler ultrasound in monitoring placental blood perfusion in hypertensive disease during pregnancy. Chin Maternal Child Health Care. 2018;10(09):48–51.
27. Zhao S, Jiang F, Li L. Ultrasound Doppler multi-parameter evaluation of intrauterine conditions in patients with pregnancy-induced hypertension. J Anhui Med Univ. 2017;52(08):1183–1187.
28. Gurung SD, Shrestha J, Gauchan E, et al. Correlation of Maternal Serum Uric Acid Level and Feto-maternal Outcome in Hypertensive Disorder of Pregnancy: a Prospective Study. Nepal J Med Sci. 2022;7(2):13–18. doi:10.3126/njms.v7i2.47207
29. Kumar N, Singh AK. Maternal Serum Uric Acid as a Predictor of Severity of Hypertensive Disorders of Pregnancy: a Prospective Cohort Study. Curr Hypertens Rev. 2018;15(2):154–160. doi:10.2174/1573402114666181112141953
30. Ryu A, Cho NJ, Kim YS, et al. Predictive value of serum uric acid levels for adverse perinatal outcomes in preeclampsia. Medicine. 2019;98(18):e15462. doi:10.1097/MD.0000000000015462
31. Zhao X, Frempong ST, Duan T. Uric acid levels in gestational hypertensive women predict preeclampsia and outcome of small-for-gestational-age infants. J Matern Fetal Neonatal Med. 2021;34(17):2825–2831. doi:10.1080/14767058.2019.1671339
32. Stødle GS, Silva GB, Tangerås LH, et al. Placental inflammation in pre-eclampsia by Nod-like receptor protein (NLRP)3 inflammasome activation in trophoblasts. Clin Exp Immunol. 2018;193(1):84–94. doi:10.1111/cei.13130
33. Sánchez-Lozada LG. The Pathophysiology of Uric Acid on Renal Diseases. Contrib Nephrol. 2018;192:17–24.
34. Baschat AA, Hecher K. Fetal growth restriction due to placental disease. Semin Perinatol. 2004;28(1):67–80. doi:10.1053/j.semperi.2003.10.014
35. Gaillard R, Arends LR, Steegers EA, et al. Second‐ and third‐trimester placental hemodynamics and the risks of pregnancy complications: the Generation R Study. Am J Epidemiol. 2013;177(8):743–754. doi:10.1093/aje/kws296
36. Ducey J, Schulman H, Farmakides G, et al. A classification of hypertension in pregnancy based on Doppler velocimetry. Am J Obstet Gynecol. 1987;157(3):680–685. doi:10.1016/S0002-9378(87)80028-5
37. Sun FG, Han B, Chen YG. Establishing and verification of the end prediction model of hypertension diseases during pregnancy. Peking Union Med Coll J. 2022;13(05):837–844.
38. Sun XW, Li XH, Zhang C, Meng F-Q, Xing Y-G, Ding Y. Correlation analysis of serum placental growth factor, pregnancy-related plasma protein-A and disease severity in patients with hypertensive disorder in pregnancy. Eur Rev Med Pharmacol Sci. 2021;25(4):1788–1795. doi:10.26355/eurrev_202102_25072
39. Lu L, Ai L, Ping ZP. Analysis of the correlation between serum uric acid levels in pregnant women and the severity of hypertensive disease during pregnancy. China Maternal Child Health Care. 2021;36(24):5469–5651.
40. Pang J, Nie HY, Chen WW. The clinical value of ultrasonic parameters of maternal uterine artery and fetal umbilical artery in pregnancy-induced hypertension in predicting pregnancy outcome. China Family Planning Obstetrics Gynecol. 2019;11(01):77–80+97.
41. Chen CQ, Huang L, Zhong FJ. Monitoring of uterine artery and umbilical artery hemodynamic parameters during pregnancy and pregnancy and analysis of maternal and fetal outcomes. Hainan Med. 2022;33(06):747–750.
42. Wu RX, Gong JJ, Jiang JW. The relationship between maternal age and adverse pregnancy outcomes. Guangdong Med. 2020;41(12):1276–1279.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.