")
Back to Journals » Clinical Ophthalmology » Volume 19
The Demodex Expert Panel on Treatment and Eyelid Health (DEPTH) Consensus Regarding the Preferred Treatment for Demodex Blepharitis
Authors Donnenfeld E , Nichols KK , Ayres BD , Farid M, Gupta PK , Lindstrom RL , Pflugfelder S, Starr CE, Venkateswaran N, Gaddie IB , Karpecki PM , Koetting C , McGee S, Periman LM , Yeu E
Received 25 March 2025
Accepted for publication 5 June 2025
Published 18 June 2025 Volume 2025:19 Pages 1893—1904
DOI https://doi.org/10.2147/OPTH.S525681
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eric Donnenfeld,1 Kelly K Nichols,2 Brandon D Ayres,3 Marjan Farid,4 Preeya K Gupta,5,6 Richard Lyndon Lindstrom,7 Stephen Pflugfelder,8 Christopher E Starr,9 Nandini Venkateswaran,10 Ian Benjamin Gaddie,11 Paul M Karpecki,12 Cecelia Koetting,13 Selina McGee,14 Laura M Periman,15 Elizabeth Yeu16
1Ophthalmic Consultants of Long Island, Long Island, NY, USA; 2School of Optometry, University of Alabama at Birmingham, Birmingham, AL, USA; 3Wills Eye Hospital, Philadelphia, PA, USA; 4Gavin Herbert Eye Institute, UC-Irvine, Irvine, CA, USA; 5Triangle Eye Consultants, Raleigh, NC, USA; 6Department of Ophthalmology, Tulane University, New Orleans, LA, USA; 7Department of Ophthalmology and Visual Neurosciences, University of Minnesota, Minneapolis, MN, USA; 8Department of Ophthalmology, Baylor College of Medicine, Houston, TX, USA; 9Department of Ophthalmology, Weill Cornell Medicine, New York, NY, USA; 10Massachusetts Eye and Ear, Harvard Medical School, Boston, MA, USA; 11Gaddie Eye Centers, Louisville, KY, USA; 12Kentucky Eye Institute, Lexington, KY, USA; 13Department of Ophthalmology, University of Colorado Medical School, Aurora, CO, USA; 14BeSpoke Vision, Edmond, OK, USA; 15Periman Eye Institute, Seattle, WA, USA; 16Virginia Eye Consultants, Norfolk, VA, USA
Correspondence: Elizabeth Yeu, Cornea, Cataract, External Disease and Refractive Surgery, Virginia Eye Consultants/EyeCare Partners, 241 Corporate Blvd, Norfolk, VA, 23502, USA, Tel +1 757 622 2200, Fax +1 757 622 4866, Email [email protected]
Purpose: To reach consensus on Demodex blepharitis (DB) treatment approaches using a modified Delphi process involving 15 ocular surface disease experts.
Methods: The Demodex Expert Panel on Treatment and Eyelid Health (DEPTH) consisted of 15 well-published ocular surface disease experts. Panelists completed two online surveys, a live consensus meeting, and a follow-up survey. The surveys consisted of scaled and multiple-choice questions related to the clinical and patient-reported outcomes of DB and its treatment. For the scaled questions using a 1 to 9 Likert scale, consensus was defined as weighted mean scores of 1– 3 and 7– 9, whereas for multiple-choice questions, consensus was achieved when a minimum of 10 of 15 panelists agreed.
Results: The DEPTH panel reached consensus that lotilaner ophthalmic solution, 0.25% should be the first-line treatment for DB. Experts agreed no additional clinical findings are needed to prompt treatment with lotilaner ophthalmic solution, 0.25% for patients with > 10 collarettes (12/15), while one additional clinical finding is needed for patients with 0– 2 (11/15) or 3– 10 collarettes (10/15). In the absence of allergies, panelists would consider first-line treatment for DB in a patient with eyelid itching but without collarettes (weighted mean: 7.47; range: 2– 9). Panelists agreed that blepharoexfoliation (weighted mean: 8.27; range: 3– 9) or intense pulsed light (IPL) therapy (weighted mean: 8.4; range: 6– 9) could supplement first-line treatment with lotilaner ophthalmic solution, 0.25%. The DEPTH panelists agreed that topical (10/15) and systemic ivermectin (14/15) are not their preferred treatment for DB. Experts did not reach consensus about the use of tea tree oil to treat DB.
Conclusion: Experts achieved consensus on the use of lotilaner ophthalmic solution, 0.25% as the first-line treatment for patients with DB. Panelists also agreed that blepharoexfoliation or IPL therapy could serve supplementally to lotilaner ophthalmic solution, 0.25%, if needed.
Keywords: blepharitis, Demodex, treatment, Delphi
Introduction
Blepharitis is a chronic inflammatory condition of the eyelid margin that often leads to conjunctivitis, functional tear deficiency, and keratitis.1 The condition is especially challenging to manage due to its chronicity and variable etiologies, which includes Demodex mite infestation, Staphylococcus bacterial infection, and seborrheic dermatitis.2,3 Two species of Demodex mites inhabit the human body: Demodex folliculorum within the lash follicle and Demodex brevis within the sebaceous gland.4 Demodex mite overgrowth (ie, demodicosis) can lead to Demodex blepharitis (DB).4 A retrospective study of 1032 sequential patients at multiple eye care centers revealed that 69.1% of patients with blepharitis were specifically diagnosed with DB.5 This disease is highly prevalent, as it is estimated that roughly 25 million US eye care patients have DB.6 Due to frequent co-occurrence with other ocular surface conditions, such as ocular rosacea, dry eye disease (DED), and meibomian gland dysfunction (MGD), DB is underdiagnosed.7 Patients with this condition commonly experience itching of the eyelid, dry eye, blurred vision, and ocular irritation, all of which negatively impact quality of life.7
The absence of a previous gold standard for treating DB, along with poor patient adherence to existing treatment options, precipitated the need to establish consensus and raise awareness regarding preferred management strategies to improve treatment outcomes.8 To this end, a panel of ophthalmologists and optometrists, including 11 of the authors in this manuscript, convened to form the Demodex Expert Panel on Treatment and Eyelid Health (DEPTH).1 The group used a modified Delphi methodology to reach consensus on the pathophysiology, patient profile, clinical and patient-reported outcomes, diagnosis, and comorbidities associated with DB. The Delphi method allows a group of experts to reach agreement through anonymous participation in an iterative series of questionnaires.9 Various groups, including the DEPTH panelists, have since modified the Delphi strategy to include a live consensus meeting.1,8,10–12 The modified Delphi process has been used across ophthalmology and optometry to establish consensus regarding a variety of topics, including the management of ocular diseases, such as DED, vernal keratoconjunctivitis, and glaucoma.10–12 In their inaugural assembly, the DEPTH panel reached consensus on several statements regarding DB, such as collarettes—cylindrical coatings at the base of the eyelashes—are the most common sign of DB and pathognomonic for the disease, epilation and visualization of mites are not necessary for diagnosis, and itching in the eyelid margin is the most common symptom.1
The same cohort of panelists reconvened to obtain consensus on DB treatment, once again using the modified Delphi method.8 DEPTH panelist agreed that patients should be treated if clinicians observe collarettes on >10 lashes per upper eyelid during a standard slit lamp examination, regardless of other signs or symptoms. Experts also reached consensus that reducing collarettes should be the primary goal of treatment. Regarding treatment options at the time, advisors agreed that tea tree oil and terpinene-4-ol-containing products were the most effective over-the-counter therapeutics, although there are drawbacks to their use, and limitations to their efficacy. Additionally, experts reached consensus that the lack of an FDA-approved treatment in 2021 warranted the use of mechanical interventions such as lid scrubs.
The first two iterations of the DEPTH panel indicated that the treatment options for DB that were available then did not negate the necessity of an FDA-approved product for the treatment of the disease. In 2023, lotilaner ophthalmic solution, 0.25% (XDEMVY®, Tarsus Pharmaceuticals, Inc., Irvine, CA) was approved for the treatment of DB.13 Lotilaner ophthalmic solution, 0.25% is an ectoparasiticide indicated for the treatment of DB through the eradication of Demodex mites. The product is available as a multidose formulation with a recommended dose of 1 drop per eye every 12 hours for 6 weeks.14 Regulatory approval was based on the results from two clinical trials, SATURN-1 (NCT04475432) and SATURN-2 (NCT04784091), both of which were sponsored by Tarsus Pharmaceuticals, Inc. The peer-reviewed articles reporting results from SATURN-1 and SATURN-2 include two and four of the authors in this publication, respectively.15,16
In view of the FDA approval of lotilaner ophthalmic solution, 0.25%, the DEPTH panel reconvened in early 2024 to reach consensus on the treatment of DB. The expanded DEPTH III panel, which comprised the 15 authors of this article, aimed to establish consensus and provide guidelines on the minimum criteria of treatment for DB now that an FDA-approved treatment is available and to assess signs and symptoms that warrant treatment. This paper describes the outcomes of the third modified Delphi process undertaken by the DEPTH panel.
Materials and Methods
The methodology used in this study was consistent with that described previously.1,8,10 Panelist selection and the modified Delphi process were conducted by an independent, third-party medical communications company (i2Vision, Inc., San Diego, CA, USA) and funded by Tarsus Pharmaceuticals, Inc. (Irvine, CA, USA). Panelists, who are also authors in this publication, were selected based on expertise in blepharitis and ocular surface diseases. Expertise was evaluated by considering the number of publications, history of podium presentations, and membership and involvement in organizations and committees related to these conditions. Ultimately, the panel selected comprised ten ophthalmologists and five optometrists, all of whom are well-published experts in ocular surface diseases.
The modified Delphi process used in this study was designed, conducted, and analyzed by i2Vision, Inc. Involvement from expert panelists and authors was strictly limited to completion of the surveys, attendance of the live consensus meeting, data interpretation, and review of this manuscript. This modified Delphi process consisted of 3 iterative electronic surveys and a live virtual consensus meeting that was held between surveys 2 and 3 (Figure 1). The surveys consisted of scaled and multiple-choice questions related to the clinical and patient-reported outcomes of DB treatment. For the scaled questions using a 1 (strongly disagree) to 9 (strongly agree) Likert scale, consensus was defined as weighted mean scores of 1–3 and 7–9. A weighted mean score of 4 to 6 signified that consensus was not reached. For other question types, consensus was achieved when a minimum of 10 of 15 panelists agreed. Where consensus was not achieved, the questions were amended according to feedback, and another Delphi survey was initiated. Blank responses were not permitted, and all panelists were required to complete all three surveys. Interim results were masked from panelists to minimize bias, and the study sponsor was masked to the study results.
 |
Figure 1 Demodex Expert Panel on Treatment and Eyelid Health (DEPTH) Delphi process flowchart. (A) The panel addressed scaled and multiple-choice questions regarding DB management. If consensus was not achieved, the statements were amended according to feedback, and another Delphi survey round was conducted. (B) Consensus was achieved when the weighted average was above 7 or below 3 using a 9-point Likert scale. For non-scaled questions, consensus was achieved when 10 of 15 panelists agreed. |
Panelist were provided with 8 articles along with a summary inclusive of pertinent methodology and high-level study design details prior to survey 1.1,7,8,15–19 Questions in survey 1 were related to panelist demographics (n=4), current approaches to the treatment of DB (n=13), considerations and treatment options for determining a first-line treatment for DB (n=64), and minimum diagnostic criteria to trigger treatment for DB (n=124). Treatment options explored were topical ivermectin, systemic ivermectin, tea tree oil, lotilaner ophthalmic solution, 0.25%, and two in-office procedures: intense pulsed light (IPL) therapy and blepharoexfoliation. To identify minimum diagnostic criteria to trigger treatment, panelists were presented with various patient scenarios that covered the presence or absence of collarettes, number of collarettes present, and need for and severity of additional (or alternative) symptoms. Results from survey 1 were compiled and analyzed for consensus.
A second survey was conducted to confirm consensus from survey 1 and move toward alignment on topics after amending questions based on panelist feedback. In survey 2, advisors were asked questions regarding determinants of finding a first-line treatment for DB (n=10), use of treatments independent of other options (n=32), use of IPL therapy or blepharoexfoliation (n=17), and the minimum diagnostic criteria to prompt treatment for DB for patients with collarettes (n=44), itching (n=40), or eyelid margin erythema (n=40). Following completion of survey 2, and prior to the live virtual consensus meeting, panelists were provided with 3 articles as pre-read material.20–22 The goal of the live consensus meeting was to facilitate discussion among the panelists to confirm areas where consensus was yet to be achieved for preparation of the third and final survey. After the consensus meeting, panelists completed survey 3, which was composed of multiple-choice and Likert-scaled questions regarding treatment of DB patients with facial rosacea (n=5), use of lid hygiene (n=5), treating mites specifically in the eyelid (n=6), patient cases with varying numbers of collarettes present (n=15), and diagnosing itching (n=1) or eyelid margin erythema (n=1) in the absence of collarettes and allergies. Result of this survey were compiled and analyzed.
Several steps were taken to minimize bias. The interim results were masked from the panelists until the end of the process, and there was a firewall between i2Vision and the study sponsor (Tarsus Pharmaceuticals, Inc) until the manuscript of study results was written. The i2Vision team was also masked to survey respondents, as the results were collected anonymously. Additionally, consensus in both scaled and non-scaled questions was predefined.
Results
In the following results, values in parentheses are the weighted mean and the range for scaled questions or how many of the 15 panelists agreed on multiple-choice questions (Table 1).
 |
Table 1 Reported Results from 3 DEPTH Surveys |
Demographic Information of the Expert Panelists
Fifteen panelists completed each survey. Twelve of the 15 panelists attended the live meeting, which was hosted and led by representatives from i2Vision. Due to scheduling conflicts, the remaining 3 panelists met with i2Vision representatives in one-on-one meetings. The panel comprised ten ophthalmologists and five optometrists in different types and durations of clinical practice. Eight panelists were women (53.3%), and 7 were men (46.7%). The participant’s mean age (standard deviation [SD]; range) was 52.5 years (11.2 years; 34–76 years) and mean number of years in practice (SD; range) was 22.9 (11.2; 3–45 years). Seven of the participants practiced in an academic setting, with the remainder in private practice. All panelists were from the United States (33.3% Southeast [n=5], 26.7% Northeast [n=4], 20.0% West [n=3],13.3% Southwest [n=2], 6.7% Midwest [n=1]).
Recommendations for a First-Line Treatment
Experts agreed that an ideal treatment for DB should have an FDA-approved indication for the condition (mean: 7.67; range: 4–9). Panelists recognized that as of 2024, lotilaner ophthalmic solution, 0.25% was the only product that fits this requirement and, therefore, should be considered as a first-line treatment for patients with DB (mean: 8.93; range: 8–9). Fourteen of 15 panelists recommended lotilaner ophthalmic solution, 0.25% as first-line treatment for this condition (Figure 2). For patients who also exhibited facial rosacea, all 15 experts recommended lotilaner ophthalmic solution, 0.25% for the treatment of DB.
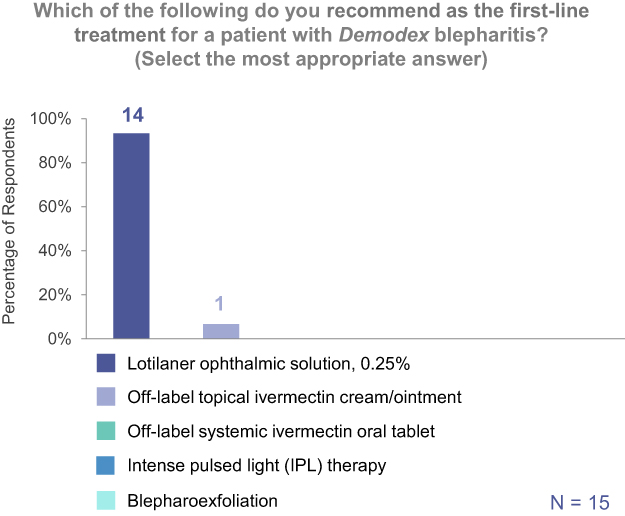 |
Figure 2 DEPTH panelists reach consensus on lotilaner ophthalmic solution, 0.25% as the first-line treatment for DB. |
Minimum Diagnostic Criteria to Trigger Treatment
Experts agreed that no additional clinical findings would be required to prompt treatment with lotilaner ophthalmic solution, 0.25% for patients with Grade 2 (>10 but <1/3 of lashes per eyelid with collarettes; 12/15 panelists), Grade 3 (≥1/3 but <2/3 of lashes per eyelid with collarettes; 15/15), or Grade 4 (≥2/3 of the lashes per eyelid with collarettes; 15/15) collarettes. For patients with less severe collarettes, panelists agreed that they would require 1 additional clinical finding to prompt treatment with lotilaner ophthalmic solution, 0.25% (Grade 0 [0–2 lashes per eyelid with collarettes], 11/15; Grade 1 [3–10 lashes per eyelid with collarettes], 10/15) (Figure 3). Additional clinical findings could include eyelid itching or eyelid margin erythema, as experts agreed they would consider using lotilaner ophthalmic solution, 0.25% to treat patients with either issue in the absence of visible collarettes after diagnostically ruling out allergies (eyelid itching [mean: 7.47; range: 2–9], eyelid margin erythema [mean: 7.20; range: 2–9]). Importantly, panelists also agreed that they would use lotilaner ophthalmic solution, 0.25% (12/15) to treat a patient presenting with eyelid itching in the absence of collarettes for DB, provided additional clinical findings, patient-reported outcomes, comorbidities, or other medication considerations, which reflects previous consensus that eyelid itching is the most common symptom in patients with DB.1 Panelists achieved consensus against the use of topical (10/15) or systemic ivermectin (14/15), and nearly reached consensus against the use of tea tree oil (9/15) in the same scenario.
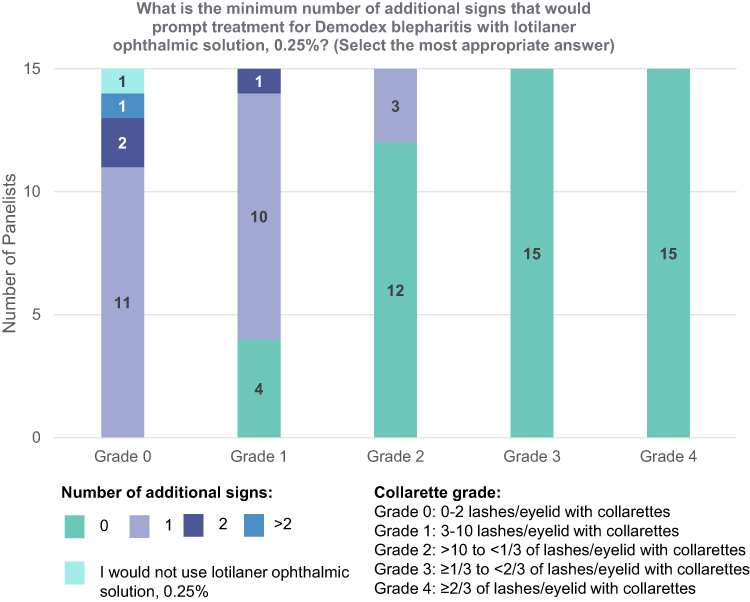 |
Figure 3 Collarette grade determines number of signs required to prompt treatment with lotilaner ophthalmic solution, 0.25%. DEPTH panelists agreed that no additional signs are necessary to prompt treatment with lotilaner ophthalmic solution, 0.25% for DB patients with Grade 2 collarettes or worse. |
Supplementary Treatments
In-Office Procedures
DEPTH panelists agreed that blepharoexfoliation could be used as a supplement with a first-line treatment (13/15), and that this in-office procedure can reduce the severity of clinical and patient-reported outcomes of DB, but should be paired with lotilaner ophthalmic solution, 0.25% to eradicate Demodex mites in the eyelid (mean: 8.27; range: 3–9). This recommendation likely reflects consensus from the panel that mechanical reduction of the pathology associated with DB can improve patient outcomes when coupled with a first-line treatment that addresses the underlying cause (mean: 7.73; range: 5–9) and that blepharoexfoliation can debulk the collarette load at the lash margin in patients (mean: 7.93; range: 6–9), but it is not sufficient to reliably eradicate Demodex mites (mean: 8.13; range: 6–9). During the live consensus meeting, panelists noted that there is limited published evidence to date that concomitant treatments have benefit for this patient population.
The panel arrived at a similar recommendation for the use of IPL therapy, albeit with the same hesitation due to the lack of published evidence for its combined use with lotilaner ophthalmic solution, 0.25%. This in-office procedure is insufficient to eradicate Demodex mites (mean: 7.13; range: 2–9) but could be used supplementally with a first-line treatment (12/15) that targets the cause of DB, such as lotilaner ophthalmic solution, 0.25% (mean: 8.40; range: 6–9). Panelists recommended the use of IPL therapy as a supplement to lotilaner ophthalmic solution, 0.25% for patients with collarettes and concomitant facial rosacea (mean: 8.20; range: 6–9; 12/15). There was agreement that IPL therapy is also an appropriate second-line therapy for patients with DB who failed to respond to first-line treatment (11/15).
Tea Tree Oil and Ivermectin
Although all advisors had used tea tree oil-based products to treat patients with DB, they did not reach consensus on how it should be used in the current treatment landscape. However, they did agree that products containing tea tree oil are defined as cosmetic products and do not require FDA approval for consumer use, and that this difference in safety and regulatory standards between cosmetics and drugs should be considered when recommending treatments to patients (mean 7.53; range: 4–9).
The panel agreed that a patient case that includes collarettes along with additional reported symptoms, observed signs, comorbid conditions, or other medication considerations would not warrant recommendation of off-label use of topical (10/15) or systemic (14/15) ivermectin. This reflects their belief that eye care providers are unfamiliar with prescribing topical (mean: 7.47; range: 2–9) and systemic (mean: 8.13; 5–9) ivermectin, and that systemic ivermectin does not fully address the clinical and patient-reported outcomes of DB (mean: 7.47; range: 4–9) while exposing patients to potential adverse effects that warrant concern (mean: 8.0; range: 2–9).
Discussion
Previous DEPTH studies deliberated on the proper treatment for DB before an FDA-approved medication that eradicates Demodex mite infestation was available.1,8 These studies concluded that the approval of an effective drug that eradicates mites would warrant a reexamination of the treatment landscape. As such, the DEPTH group reconvened to achieve consensus regarding first-line treatment of DB considering the FDA approval of lotilaner ophthalmic solution, 0.25%. Prior to the availability of lotilaner ophthalmic solution, 0.25%, the most common approaches to manage the disease were products containing tea tree oil or its effective component 4-terpinol, and topical or systemic broad-spectrum parasiticide ivermectin. In-office procedures such as IPL therapy and blepharoexfoliation were used as adjuncts to treatment.7 This current modified Delphi study aimed to reach consensus on a definitive treatment regimen for DB and the minimum diagnostic criteria to trigger treatment.
The DEPTH experts previously indicated that an FDA-approved medication that eradicates Demodex mites is needed. Lotilaner ophthalmic solution, 0.25% became the first and only FDA-approved treatment for DB in 2023. SATURN-1 (NCT04475432) and SATURN-2 (NCT04784091), two pivotal randomized, placebo-controlled clinical trials, illustrated the efficacy and safety of lotilaner ophthalmic solution, 0.25% for patients with DB. The primary endpoint (≤2 upper eyelid collarettes at day 43 of treatment) was met by 44.0% and 56.0% of patients in the lotilaner ophthalmic solution, 0.25% group in SATURN-1 and SATURN-2, respectively, versus 7.4% and 12.5% of those in the control group (both P<0.0001).15,16 These trials also recorded the percentage of patients that achieved a collarette cure, which was defined as a reduction in collarettes to ≤10 lashes per eyelid. In SATURN-1 and SATURN-2, respectively, 81.3% and 89.1% of patients in the lotilaner ophthalmic solution, 0.25% group versus 23.0% and 33.0% in the control group achieved a reduction in collarettes (both P<0.0001).15,16
The SATURN-1 and SATURN-2 trials also examined the efficacy of lotilaner ophthalmic solution, 0.25% to eradicate mites and cure eyelid margin erythema, as well as the potential ocular adverse reactions. Mite eradication was defined as the percentage of patients who achieved a Demodex density of 0 per eyelash. In SATURN-1, 67.9% of the patients in the lotilaner ophthalmic solution, 0.25% group achieved mite eradication versus 17.6% of patients in the control group (P<0.0001).15 In SATURN-2, 51.8% of patients in the lotilaner ophthalmic solution, 0.25% group achieved mite eradication versus 14.6% of patients in the control group (P<0.0001).16 These trials also examined eyelid margin erythema using a grading scale of 0–3, where 0 represented an erythema cure. In SATURN-1, significantly more patients in the lotilaner ophthalmic solution, 0.25% group achieved an erythema cure than patients in the control group (19.1% vs 6.9%, respectively; P=0.0001).15 Similarly, in SATURN-2, a higher proportion of patients in the lotilaner ophthalmic solution, 0.25% group achieved an erythema cure than those in the control group (31.1% vs 9.0%, respectively; P<0.0001).16 In both trials, lotilaner ophthalmic solution, 0.25% was rated as neutral to very comfortable by ≥90% of patients. In SATURN-1 and SATURN-2, respectively, the most common ocular treatment-emergent adverse event (TEAE) was instillation site pain in 11.8% and 7.9% of study patients versus 7.7% and 6.7% of control patients.15,16
The consensus reached in this report reflects the unmet need for patients with DB prior to FDA-approval of lotilaner ophthalmic solution, 0.25%. The panelists agreed that they would choose lotilaner ophthalmic solution, 0.25% to treat patients with Grade 2 collarettes (>10 lashes per eyelid with collarettes) or worse in the absence of any other clinical findings. In cases where patients exhibit a less severe collarette grade, panelists agreed that one more clinical finding would be needed to trigger treatment (Figure 3). Importantly, panelists agreed that they would consider using lotilaner ophthalmic solution, 0.25% to treat patients with reported eyelid itching or eyelid margin erythema in the absence of visible collarettes so long as allergies have been ruled out, suggesting a high level of confidence in treating patients with the FDA-approved medication. These findings reflect the efficacy of lotilaner ophthalmic solution, 0.25% in eradicating Demodex mites, and the reported limitations of other treatment options.7,15,16
An interesting finding from this study was the consensus reached regarding the most appropriate use of IPL therapy and blepharoexfoliation. Panelists agreed that both treatments best serve as supplements to a first-line treatment (ie, lotilaner ophthalmic solution, 0.25%). This consensus reflects prior use of these in-office procedures as adjunct therapies.7 During the live consensus meeting, panelists noted their reluctance to formally recommend IPL therapy or blepharoexfoliation layered on top of lotilaner ophthalmic solution, 0.25% to treat DB. This is due to lack of published evidence supporting the concomitant use of either treatment with the FDA-approved therapeutic to treat Demodex infestation in the eyelid. Future studies should aim to determine the benefits of coupling lotilaner ophthalmic solution, 0.25% with IPL therapy or blepharoexfoliation to treat patients with DB. The confirmation of benefits should lead to additional studies to delineate an ideal, layered treatment regimen.
Previous DEPTH studies have cautioned that the results may not be repeatable with different experts, as a limited sample size is not guaranteed to reflect the thoughts and opinions of all clinicians. This concern also applies to the third DEPTH study results. That said, a recent study from the United Kingdom suggests that findings from the first two DEPTH studies and the study discussed here may be widely applicable. In the UK study, a group of 11 experts (2 ophthalmologists, 8 optometrists, and 1 contact lens optician) used the Delphi process to reach consensus on a diagnostic algorithm and management guidelines for DB.23 This study did not include lotilaner ophthalmic solution, 0.25%, as it is currently unavailable in Europe. Consistent with the first DEPTH study,1 Sharma et al agreed that collarettes are pathognomonic for DB, and that eyelid margin itching was the most common symptom.23 In general alignment with the second DEPTH study,8 the UK panel also agreed that tea tree oil was the most appropriate preferred treatment after performing lid hygiene to remove collarettes.23 Furthermore, the panel recommended switching to second-line treatments including in-office application of high concentrations of tea tree oil, IPL therapy, eyelid debridement, oral drugs such as azithromycin and doxycycline, or additional pharmacological treatment such as antibiotics when improvement in clinical and patient-reported outcomes were not evident by 4–6 weeks of treatment.23 The results of this study suggest that the findings from the first two DEPTH publications are generalizable. Currently, lotilaner ophthalmic solution, 0.25% is not available outside of the United States. It will be interesting to see if the potential availability of lotilaner ophthalmic solution, 0.25% in the UK will lead to additional Delphi studies that change the treatment algorithm proposed by Sharma et al to reflect the findings in this article.
In conclusion, this third DEPTH study proved effective in establishing consensus on the first-line treatment for DB and the minimum diagnostic criteria to prompt treatment. With increased awareness and expert-recommended guidelines, eye care practitioners can offer patients with DB an evidence-based approach to treatment and better clinical outcomes.
Acknowledgments
The authors would like to thank the i2Vision team. The team at i2Vision selected the panelists, completed the literature review, developed the survey questions and methods, determined the reading material for panelists, administered the face-to-face meeting, analyzed the data following each survey to develop the subsequent surveys, and supported the authors in the writing of this paper. The authors would also like to thank Tarsus Pharmaceuticals, Inc., for funding this study. Employees of Tarsus Pharmaceuticals, Inc. did not participate in these activities; they did have the opportunity to read this paper prior to its submission.
Funding
This study was funded by Tarsus Pharmaceuticals, Inc. Medical writing support for this manuscript was provided by i2Vision, Inc. and funded by Tarsus Pharmaceuticals, Inc.
Disclosure
E. Donnenfeld is a consultant to Aeon, Allegro, Allergan, Alcon, Aurion, Avellino Labs, Bausch & Lomb, CorneaGen, Covalent, CRST, Crystilex, BVI, Blephex, Dompe, ELT Sight, EyePoint Pharma, Foresight, Glaukos, Horizon Surgical Systems, Inversa, Ivantis, Johnson & Johnson, Kala, Katena, Lacripen, LayerBio, LensGen, Mati Pharmaceuticals, Melt Pharmaceuticals, MDBackline, Merck, Mimetogen, MOA, Nanowafer, Nordic Pharma, Novabay, Novartis, Novaliq, Ocular Innovations, Oculis, Odyssey, Omega Ophthalmics, Pfizer, Ocuhub, Omeros, PRN, Rayner, ReTear, RPS, Shire, Strathspey Crown, SUN, Surface, Tarsus, Tearscience, Thea, Trukera, Veracity, Versant Ventures, Visionary Venture, Visus, and Zeiss; has held leadership or committee positions at MOA, Oculis, and Ten Point; and has stock or stock options in Aeon, Aurion, Avedro, CorneaGen, Covalent, Crystilex, ELT Sight, EyePoint Pharma Glaukos, Horizon Surgical Systems, Inversa, Ivantis, Lacripen, LayerBio, LensGen, Mati Pharmaceuticals, Melt Pharmaceuticals, MDBackline, Mimetogen, MOA, Novabay, Ocuhub, Ocular Innovations, Oculis, Rayner, ReTear, RPS, Strathspey Crown, Surface, Tarsus, TenPoint, Veracity, Versant Ventures, and Visionary Ventures. K. K. Nichols discloses grants or contacts paid to her institution by Aramis, Kowa, Science Based Health, Sylentis, and TearScience; and is a consultant to Abbvie, Alcon, Alderya, Azura, Bausch & Lomb, Bruder, Cavalry, Cloudbreak, Dompe, HanAll Bio, Harrow, Novartis, Novaliq, Oyster Point Pharma/Viatris, Santec, Sight Sciences, Sydnexis, Tarsus, TearSolutions, Thea, Topcon, Trukera, and Visus. B. D. Ayres is a consultant to and has received honoraria from Tarsus. M. Farid is a consultant to Abbvie, Alcon, Bausch & Lomb, Biotissue, CorneaGen, Glaukos, Harrow, Johnson and Johnson Vision, Tarsus, Viatris, and Zeiss. P. K. Gupta is a consultant to Azura, Alcon, Aldeyra, Abbvie, Bausch + Lomb, Dompe, Expert Opinion, HanAll Biopharma, J&J Vision, Kala, Mazado, Inc, Nordic Pharma, Ocular Science, Oculis, Orasis, Sight Sciences, Science Based Health, Spyglass, Surface Ophthalmics, Tarsus, Tear Clear, Thea, Tissue Tech, Inc, Trukera, Viatris, Visionology, Vital Tears, and Zeiss, and has stock or stock options in Azura, Expert Opinion, Orasis, Tarsus, Tear Clear, Surface, Spyglass, and Visionology. R. L. Lindstrom is a consultant to and has stock or stock options in Tarsus. S. Pflugfelder discloses grants or contracts paid to his institution by Alcon; is a consultant to Alcon, Dompe, Kala, Kowa, and Tarsus; and was an advisor for AstraZeneca. C. E. Starr is a consultant to Aesculus, Alcon, Aldeyra, Allgenesis, Allergan/Abbvie, Amgen, Azura, Bausch & Lomb, BlephEx, Bruder, CSI Dry Eye, Dompe, Essiri LLC, Eyebiotech Limited, Eye Care International, Glaucos, i2Vision, Johnson & Johnson Vision, Lumenis, Kala, Novaliq, Novartis, Nuvissa, Oculis, Olivio & Co., Oyster Point, Quidel, Sight Sciences, Sofia Biologics, Sun Pharma, Tarsus, Thea, Trukera, Versea, and Visionology; and has stock or stock options in CSI Dry Eye, Essiri LLC, Nuvissa, Sofia Biologics, and Visionology. N. Venkateswaran is a consultant to Abbvie, Alcon, Bausch & Lomb, Glaukos, Johnson and Johnson, Ocular Therapeutix, Sight Sciences, Tarsus, and Thea. I. B. Gaddie is a consultant to Alcon, Bausch & Lomb, Harrow, i2Vision, and Tarsus; has received honoraria from Bausch & Lomb, Harrow, and Tarsus; and has stock or stock options in Harrow and Tarsus. P. M. Karpecki is a consultant to Abbvie, Alcon, Aldeyra, Aramis, Atlas, Azura, Bausch & Lomb, BioTissue, Bruder, Bruno Vision Care, Dompe, Essilor, Eyedetec, Harrow, Healthe, Nordic Pharma, Oasis Medical, Oculis, Ocuphire, Oculus, OcuSoft, Orasis, RxSight, Science Based Health, Scope, Sentiss, Sight Sciences, Silk Tears, Sun Pharmaceuticals, Surface, Sydnexis, Tarsus, Thea, Topcon, Viatris, Vital Tears, and Zeiss; has received honoraria from Bausch & Lomb, Dompe, Mallinckrodt, and Tarsus; and has stock or stock options in AdOM, AI Optics, Azura, Barti, Danelli Ocular Creations, Eyedaptic, Eyedetec, Eyesafe, Hui.AI, iOR Holdings, Iveena, LacriSciences, LeGrande, LenTechs, Lubris, Mati Therapeutics, New Sight Reality, Ocular Science, OcuMedic, Omega Ophthalmics, Omera Medical, Ophthalmic Resources, Orasis, Percept Health, Cambium, Olympic Ophthalmics, RegenerEyes, Silk Technologies, Stuart Therapeutics, TearClear, TearSolutions, TecLens, Visant Medical, and Vision Path. C. Koetting is a consultant to Abbvie, Alcon, Bausch & Lomb, Dompe, and Tarsus; and has received honoraria from Alcon, Bausch & Lomb, Dompe, and Tarsus. S. McGee is a consultant to Aldeyra, Abbvie, Alcon, Avellino, Lumenis, Bausch & Lomb, Bruder, Cynosure, Horizon, Optovue, Novartis, Sun, Versant, Kala, Dompe, RVL, Tarsus, Science Based Health, Thea, Oyster Point, Topcon, and Zeiss. L. Periman is a consultant to Alcon, Aldeyra, Allergan/Abbvie, Amgen, Azura, B&L, Bruder, Dompe, Eyedetec, Kala, Lumenis, Mallinckrodt, Myze, Nordic Pharma, Novartis, Nusight Medical, Olympic Ophthalmics, Quench Method, Science Based Health, Scope, Sun, Tarsus, Thea, Verséa, Viatris, and Visant. E. Yeu was an employee of Virginia Eye Consultants and a board member, consultant, and stockholder of Tarsus Pharmaceuticals, Inc. (“Tarsus”) at the time of the study. She was also a consultant for Abbvie, AcuFocus, Adaptilens, Advanced Vision Group, Alcon, Aldeyra, Aurion, Avellino, Bausch & Lomb, BioTissue, BVI, Blephex, Bruder, Centricity, Dompe, Elios, Expert Opinion, Eyenovia, Foresight, Glaukos, Guidepoint, Iveric, Johnson & Johnson Vision, Kala, LayerBio, LensAR, Melt, New World Medical, OSRX, Oculis, Ocusoft, Samsara, Science Based Health, Sight Sciences, STAAR, Surface, Thea, Tarsus, Visus, and Zeiss. Dr. Yeu is now an employee of Tarsus Pharmaceuticals, Inc. The authors report no other conflicts of interest in this work.
References
1. Ayres BD, Donnenfeld E, Farid M, et al. Clinical diagnosis and management of Demodex blepharitis: the Demodex Expert Panel on Treatment and Eyelid Health (DEPTH). Eye. 2023;37(15):3249–3255. doi:10.1038/s41433-023-02500-4
2. Teo A, Rosenberg E, Jacobson A. Prevalence of Demodex colonization in patients presenting to an outpatient clinic. Invest Ophthalmol Vis Sci. 2021;62(8):1236.
3. Amescua G, Akpek EK, Farid M, et al. American academy of ophthalmology preferred practice pattern cornea and external disease panel. blepharitis preferred practice pattern. Ophthalmology. 2019;126(1):P56–P93. doi:10.1016/j.ophtha.2018.10.019
4. Luo X, Li J, Chen C, Tseng S, Liang L. Ocular demodicosis as a potential cause of ocular surface inflammation. Cornea. 2017;1(Suppl 1):S9–S14. doi:10.1097/ICO.0000000000001361
5. Trattler W, Karpecki P, Rapoport Y, et al. The prevalence of Demodex blepharitis in US eye care clinic patients as determined by collarettes: a pathognomonic sign. Clin Ophthalmol. 2022;16:1153–1164. doi:10.2147/OPTH.S354692
6. O’Dell L, Dierker DS, Devries DK, et al. Psychosocial impact of Demodex blepharitis. Clin Ophthalmol. 2022;16:2979–2987. doi:10.2147/OPTH.S374530
7. Rhee MK, Yeu E, Barnett M, et al. Demodex blepharitis: a comprehensive review of the disease, current management, and emerging therapies. Eye Contact Lens. 2023;49(8):311–318. doi:10.1097/ICL.0000000000001003
8. Farid M, Ayres BD, Donnenfeld E, et al. Delphi panel consensus regarding current clinical practice management options for Demodex blepharitis. Clin Ophthalmol. 2023;17:667–679. doi:10.2147/OPTH.S399989
9. Dalkey NC. The Delphi Method: An Experimental Study of Group Opinion. Santa Monica, CA: RAND Corporation; 1969.
10. Aragona P, Giannaccare G, Mencucci R, et al. The management of dry eye disease: proceedings of Italian dry eye consensus group using the delphi method. J Clin Med. 2022;11(21):6437. doi:10.3390/jcm11216437
11. Ghiglioni DG, Bruschi G, Chiappini E, et al. Seeing eye to eye: a modified Delphi method-based multidisciplinary expert consensus on the diagnosis and treatment of vernal keratoconjunctivitis. Eur J Pediatr. 2024;183(11):5053–5061. doi:10.1007/s00431-024-05776-0
12. Iorio-Aranha F, de Freitas C, Rocha-Sousa A, Azevedo A, Barbosa-Breda J. Nationwide consensus on quality indicators to assess glaucoma care: a modified Delphi approach. Eur J Ophthalmol. 2024;34(1):217–225. doi:10.1177/11206721231170033
13. Page MR. Multidisciplinary perspectives in Demodex blepharitis: a new view of treatment from clinical, payer, and patient perspectives. J Manag Care Spec Pharm. 2024;30(10–a Suppl):S1–S8. doi:10.18553/jmcp.2024.30.10-a.s1
14. XDEMVY. Highlights of prescribing information. Available from: https://tarsusrx.com/wp-content/uploads/XDEMVY-Prescribing-Information-24JUL23.pdf.
15. Yeu E, Wirta DL, Karpecki P, Baba SN, Holdbrook M, Saturn I Study Group. Lotilaner ophthalmic solution, 0.25%, for the treatment of Demodex blepharitis: results of a prospective, randomized, vehicle-controlled, double-masked, pivotal trial (Saturn-1). Cornea. 2023;42(4):435–443. doi:10.1097/ICO.0000000000003097
16. Gaddie IB, Donnenfeld ED, Karpecki P, et al. Saturn-2 Study Group. Lotilaner ophthalmic solution 0.25% for Demodex blepharitis: randomized, vehicle-controlled, multicenter, Phase 3 trial (Saturn-2). Ophthalmology. 2023;130(10):1015–1023. doi:10.1016/j.ophtha.2023.05.030
17. Koo H, Kim TH, Kim KW, Wee SW, Chun YS, Kim JC. Ocular surface discomfort and Demodex: effect of tea tree oil eyelid scrub in Demodex blepharitis. J Korean Med Sci. 2012;27(12):1574–1579. doi:10.3346/jkms.2012.27.12.1574
18. Choi Y, Eom Y, Yoon EG, Song JS, Kim IH, Kim HM. Efficacy of topical ivermectin 1% in the treatment of Demodex blepharitis. Cornea. 2022;41(4):427–434. doi:10.1097/ICO.0000000000002802
19. Hirsch-Hoffmann S, Kaufmann C, Bänninger PB, Thiel MA. Treatment options for Demodex blepharitis: patient choice and efficacy. Klin Monbl Augenheilkd. 2015;232(4):384–387. doi:10.1055/s-0035-1545780
20. Akhtar SMM, Fareed A, Sohaib Asghar M, Mumtaz M, Kaur S. Efficacy and safety of lotilaner ophthalmic solution 0.25% for the treatment of Demodex blepharitis: a meta-analysis of randomized controlled trials. Cont Lens Anterior Eye. 2024;47(3):102148. doi:10.1016/j.clae.2024.102148
21. Talha M, Haris Ali M, Fatima E, Nadeem A, Ahmed A, Nashwan AJ. Efficacy and safety of lotilaner ophthalmic solution (0.25%) for the treatment of Demodex blepharitis: a GRADE assessed systematic review and meta-analysis of observational & experimental studies. Am J Ophthalmol. 2024;264:8–16. doi:10.1016/j.ajo.2024.03.019
22. Abo Zeid M, Elrosasy A, Abbas AW, Elganady A, Rhab AE, Abu Serhan H. Efficacy and safety of lotilaner ophthalmic solution 0.25% in the treatment of Demodex blepharitis: a systematic review and meta-analysis. Ocul Immunol Inflamm. 2024;32(10):2494–2505. doi:10.1080/09273948.2024.2309552
23. Sharma N, Martin E, Pearce EI, Hagan S. A delphi approach to establishing consensus on best practice for the diagnosis and treatment of Demodex blepharitis. Cont Lens Anterior Eye. 2024;47(1):102080. doi:10.1016/j.clae.2023.102080
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.