")
Back to Journals » Clinical Ophthalmology » Volume 19
The Effect of Eyedrop Size on Pupillary Dilation Using the Nanodropper Bottle Adapter
Authors Chow A , Choi J , Bacharach J
Received 3 November 2024
Accepted for publication 12 February 2025
Published 6 April 2025 Volume 2025:19 Pages 1217—1221
DOI https://doi.org/10.2147/OPTH.S504416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Audrey Chow,1 Jin Choi,1 Jason Bacharach1,2
1Department of Ophthalmology, California Pacific Medical Center, San Francisco, CA, USA; 2North Bay Eye Associates, Petaluma, CA, USA
Correspondence: Jin Choi, Department of Ophthalmology, California Pacific Medical Center, 711 Van Ness Ave, Suite 250, San Francisco, CA, 94102, USA, Email [email protected]
Introduction: Ophthalmic medications administered via standardized eyedrop bottles have an average drop size of 40 μL, but absorption is limited to the conjunctival sac volume of 7– 10 μL. The Nanodropper is a commercially available eyedrop bottle adapter capable of consistently delivering 10 μL aliquots. We hypothesized that the Nanodropper would supply a sufficient medication dose for mydriasis that is non-inferior to the standard eyedrop bottle.
Material and methods: Adult patients scheduled for routine bilateral eye dilation were selected. Exclusion criteria included anisocoria, use of mydriatic agents, and unilateral pseudoexfoliation. One eye was randomly selected and dilated with the Nanodropper, and the fellow eye dilated with the standard bottle with a 50/50 mixture of 1% tropicamide and 2.5% phenylephrine. Pre- and post-dilation pupil sizes were objectively measured with a pupillometer and compared between fellow eyes with a noninferiority margin of 0.5mm.
Results: A total of 54 patients (108 eyes, 54 pairs) were included in the study. Pre-dilation pupil sizes were similar in the Nanodropper eye compared to the fellow eye. There was no difference in post-dilation pupil size between fellow eyes with a noninferiority margin of 0.5mm (95% CI [− 0.09, 0.15], p = 0.67).
Discussion: This study demonstrates that small volume eye drops using the Nanodropper adapter are as efficacious as standard volume drops for mydriasis. This may provide many clinical, practical, and economic advantages such as reducing medication excess, toxicity, and material costs.
Conclusion: The Nanodropper is non-inferior to the standard eyedrop bottle for pupillary dilation. Small volume eyedrops may reduce medication waste and side effects and improve affordability and patient compliance.
Plain Language Summary: Efficacy of small volume drops using a Nanodropper adapter for pupil dilation compared to a standard volume was studied. The Nanodropper mechanism was non-inferior to standard volume drops for mydriasis.
Keywords: medications, mydriatics
Introduction
Ophthalmic medications are commercially available and administered via standardized eyedrop bottles with an average drop size of 40 µL.1 The surface of the human eye and conjunctival sac is capable of retaining 7–10 µL, with the remainder of the overflowing fluid lost as runoff.2,3 Despite the deliverance of topical medications in 40 µL aliquots, in actuality the ophthalmic absorption is limited to the medication available within this smaller reservoir. This excess leads to unintentional pharmaceutical waste, increased medication costs and adherence issues due to more frequent refills, and greater risk of medication toxicity due to higher volumes delivered.4,5
Mydriatic agents such as tropicamide and phenylephrine are frequently administered in the ophthalmology clinical setting for dilated fundus examinations as well as in surgical centers prior to intraocular surgery. One cost analysis investigating multi-use of mydriatic agents versus single-bottle use for pre-operative or pre-intravitreal injection dilation estimated a 97.1% reduction in number of bottles used with a predicted 5-year cost savings of $240,000 USD per institution.6 Therefore, reducing medication waste and excess during routine exams and procedures offers an opportunity for major cost savings and minimizing potential patient harm from medication toxicity or intolerance.
Additional prior studies have demonstrated comparable efficacy of various topical ophthalmic pharmaceutical agents including beta blockers and mydriatic agents with smaller doses. These studies primarily investigated smaller volumes (<20 µL) compared to larger volumes (>30 µL).7,8 The Nanodropper (Nanodropper, Inc) is a commercially available, FDA listed (class 1 medical device, 510(k) exempt) eyedrop bottle adapter that is capable of consistent delivery of 10 µL drops.9,10 Given the limited reservoir for medication absorption, we hypothesized that the Nanodropper would supply a sufficient medication dose for mydriasis that is non-inferior to the standard eyedrop bottle.
Methods
This study was approved by the Sutter Health IRB at the California Pacific Medical Center (CPMC), San Francisco, California, and followed the tenets of the Declaration of Helsinki. Informed consent was obtained from all subjects and HIPAA regulations were followed.
A prospective, comparative, matched-pairs study consisting of adults scheduled for routine bilateral eye dilation was conducted at the Lions Eye Clinic of CPMC in January 2022. Exclusion criteria included contraindications to pharmacologic mydriasis such as high-risk angle closure suspects, allergies to phenylephrine or tropicamide, concurrent use of any mydriatic or miotic agents (eg, atropine, cyclopentolate, brimonidine), anisocoria (>1 mm), traumatic pupil, surgical pupil, and unilateral pseudoexfoliation. A power analysis was conducted to determine the required sample size based on a non-inferiority margin of 0.5mm. With a significant level of alpha 0.025 and a desired power of 0.90, a minimum sample size of 42 per study group was determined.
All patients were pharmacologically dilated in both eyes with a 50/50 mixture of 1% tropicamide and 2.5% phenylephrine. For each patient, one eye was randomly selected and dilated with the Nanodropper, while the fellow eye was dilated with the standard bottle. Pupillary diameters were objectively measured using a pupillometer (NeurOptics VIP-300 pupillometer) before and 30 minutes after medication administration. A paired t-test was conducted to compare post-dilation pupil sizes between fellow eyes within a given patient. Additionally, paired t-test for non-inferiority was performed with a non-inferiority margin of 0.5 mm. Subgroup analyses were performed for patients with a history of bilateral intraocular surgery and diabetes.
Statistical analyses were performed using SAS 9.4 software (SAS Institute Inc., Cary, NC, USA).
Results
A total 108 eyes of 54 patients were included in this study. Pre- and post-dilation pupil sizes (diameter) of the control eye were compared to that of the fellow Nanodropper eye within the same subject. Baseline pre-dilation pupil size between the control and Nanodropper eyes were similar (mean difference 0.05 ± 0.28 mm, 95% CI [−0.03, 0.13], p = 0.20) (Table 1). Of the 54 patients, 12 (22%) patients had a history of bilateral intraocular surgery and 38 (70%) patients had a history of diabetes. Baseline pre-dilation pupil sizes of the control eye and Nanodropper eye were comparable in both subgroups as listed in Table 1.
 |
Table 1 Pre-Dilation Pupil Size as Measured in Millimeters |
Post-dilation pupil sizes are shown in Table 2. The mean post-dilation pupil size of the control eye and the Nanodropper eye was 7.31 ± 0.89 mm and 7.28 ± 0.96 mm, respectively. There was no statistically significant difference in post-dilation pupil size between the control and Nanodropper eyes (mean difference 0.03 ± 0.44 mm, 95% CI [−0.09, 0.15], p = 0.67), as seen in Figure 1. The mean difference in post-dilation pupil size was well within the non-inferiority margin of 0.5mm, with the upper limit of the 95% confidence interval of 0.15mm.
 |
Table 2 Post-Dilation Pupil Size as Measured in Millimeters |
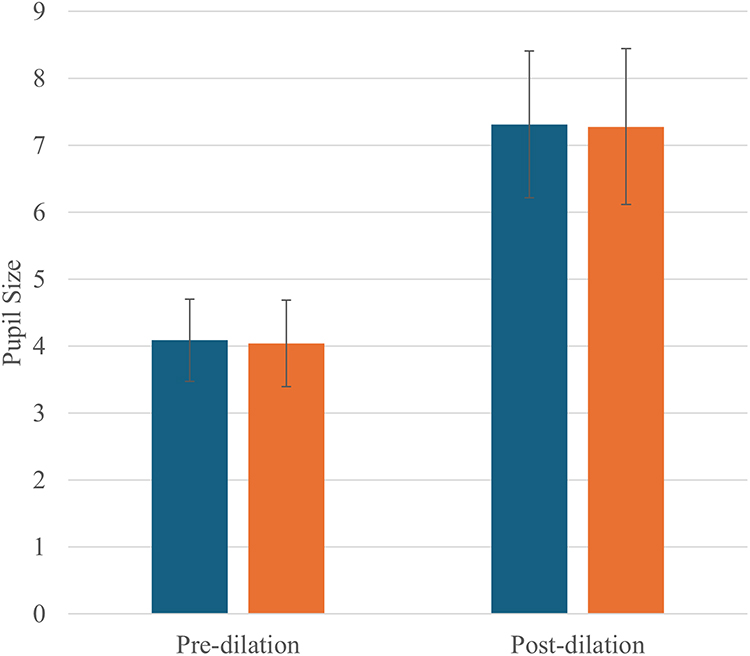 |
Figure 1 Mean differences between pupil sizes of the control eye and Nanodropper eye, pre- and post-dilation. Blue: Control eye. Orange: Nanodropper eye. |
Subgroup analyses of patients with a history of bilateral intraocular surgery and patients with diabetes were similarly conducted. Post-dilation pupil sizes of patients with bilateral intraocular surgery were 6.57 ± 0.64 mm in the control eye and 6.62 ± 0.99 mm in the Nanodropper eye. There was no statistically significant difference between eyes, with a mean difference of 0.06 ± 0.51 mm (95% CI [−0.45, 0.34], p = 0.75). Similarly, there was no statistically significant difference for the subgroup with diabetes (mean difference 0.10 ± 0.43 mm (95% CI [−0.04, 0.24], p = 0.17)).
Non-inferiority analysis with a 0.5 mm margin was conducted, which demonstrated that the Nanodropper eye was non-inferior to the control eye for pupil dilation (mean difference 0.03 ± 0.44 mm, 95% upper confidence limit 0.13 mm, p = <0.01). The statistically significant non-inferiority was maintained for the subgroups with a history of bilateral intraocular surgery and history of diabetes (Table 3).
 |
Table 3 Non-Inferiority Testing of Post-Dilation Pupil Size as Measured in Millimeters |
Discussion
This study demonstrates that small volume eye drops using the Nanodropper adapter (approximately 10 µL) are as efficacious as standard volume drops (approximately 40 µL) for mydriasis using tropicamide and phenylephrine. Another study similarly showed non-inferiority of the Nanodropper for dilation in the pediatric population.10 Using smaller volume drops while maintaining pharmacologic efficacy can provide many clinical, practical, and economic advantages. These benefits include reducing medication excess, waste, and material cost for both patients and clinicians. Additionally, this would potentially minimize adverse effects from local irritation (eg, ocular surface irritation, benzalkonium chloride contact dermatitis) and systemic absorption.
The strengths of this study include the prospective and matched-pairs study design which allowed for more controlled data collection and minimized confounding variables by comparing fellow eyes within the same patient. Limitations of this study include the relatively small sample size and study conduct at a single institution, which limits the power of statistical analysis and generalizability of results. The subject population in this study is almost entirely of Latino or Asian descent with dark brown irides. Darker irides can have reduced effectiveness to different dilating combinations than lighter iridies.11 However, the study sufficiently demonstrated statistically significant non-inferiority of the Nanodropper adapter for mydraisis, which has widespread applicability for medical providers and patients.
Further research is needed to investigate the efficacy of small volume drops using the Nanodropper for other pharmacologic agents. Many vision-threatening ophthalmic pathologies rely on frequent topical drop administration including glaucoma, infectious keratitis, uveitis, and post-operative inflammation. A recent study showed non-inferiority of topical beta-blocker delivered through the Nanodropper adapter compared to the standard eyedrop bottle.12 This would reduce the risk of systematic absorption, which can have dose-dependent adverse effects such as heart block and bronchospasm.13 Smaller volume drops of other medications such as costly compounded antibiotics for bacterial keratitis, or intraocular pressure-lowering agents with topical toxicity (eg, prostaglandin analogues, rho kinase inhibitors) or preservatives (eg, benzalkonium chloride) may offer additional patient benefits by reducing out-of-pocket costs and improving tolerance.14–16 Medication costs are strongly associated with medication non-adherence and lowering costs can potentially improve visual outcomes.17
In conclusion, small volume (10 µL) drops using the Nanodropper bottle adapter was as effective as the standard bottle drops for mydriasis. Small volume drops may reduce medication waste and side effects and improve affordability and patient compliance.
Acknowledgments
Nanodropper devices were provided by Nanodropper, Inc, which did not have a role in the study design or execution.
Disclosure
The authors have no funding sources or relevant financial/proprietary interests to report.
Presented as a poster at ASCRS May 5–8, 2023 in San Diego, CA.
References
1. Van Santvliet L, Ludwig A. Determinants of eye drop size. Surv Ophthalmol. 2004;49(2):197–213. doi:10.1016/j.survophthal.2003.12.009
2. Kumar S, Karki R, Meena M, Prakash T, Rajeswari T, Goli D. Reduction in drop size of ophthalmic topical drop preparations and the impact of treatment. J Adv Pharm Technol Res. 2011;2(3):192–194. doi:10.4103/2231-4040.85540
3. Mishima S, Gasset A, Kylce S, Baum J. Determination of tear volume and tear flow. Inv Ophthalmol. 1966;5:264–276.
4. Jaenen N, Baudouin C, Pouliquen P, Manni G, Figueiredo A, Zeyen T. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur J Ophthalmol. 2007;17(3):341–349. doi:10.1177/112067210701700311
5. Farkouh A, Frigo P, Czejka M. Systemic side effects of eye drops: a pharmacokinetic perspective. Clin Ophthalmol. 2016;10:2433–2441. doi:10.2147/OPTH.S118409
6. Berkowitz ST, Finn A, Sternberg P, Patel S. Potential Cost Savings Associated With a Multiuse Preoperative and Preinjection Eyedrop Protocol. Ophthalmology. 2022;129(11):1305–1312. doi:10.1016/j.ophtha.2022.06.023
7. Charap AD, Shin DH, Petursson G, et al. Effect of varying drop size on the efficacy and safety of a topical beta blocker. Ann Ophthalmol. 1989;21(9):351–357.
8. Gray RH. The influence of drop size on pupil dilatation. Eye (Lond). 1991;5(Pt 5):615–619. doi:10.1038/eye.1991.107
9. St Peter DM, Steger JS, Patnaik JL, Davis N, Kahook MY, Seibold LK. Reduction of Eyedrop Volume for Topical Ophthalmic Medications with the Nanodropper Bottle Adaptor. Med Devices. 2023;16:71–79. doi:10.2147/MDER.S397654
10. Hoppe CB, Yonamine S, Kao BW, et al. Randomized Trial to Evaluate the Efficacy of the Nanodropper Device for Pupillary Dilation and Cycloplegia in Children. Ophthalmology. 2023;130(3):324–330. doi:10.1016/j.ophtha.2022.10.016
11. Anderson HA, Bertrand KC, Manny RE, Hu YS, Fern KD. Comparison of two drug combinations for dilating dark irides. Optom Vis Sci. 2010;87(2):120–124. doi:10.1097/OPX.0b013e3181cc8da3
12. Steger JS, Durai I, Odayappan A, et al. An Evaluation of the Efficacy and Safety of Timolol Maleate 0.5% Microdrops Administered with the Nanodropper. Ophthalmology. 2024;131(9):1045–1055. doi:10.1016/j.ophtha.2024.03.012
13. Vander Zanden JA, Valuck RJ, Bunch CL, Perlman JI, Anderson C, Wortman GI. Systemic adverse effects of ophthalmic beta-blockers. Ann Pharmacother. 2001;35(12):1633–1637. doi:10.1345/aph.18464
14. Hedengran A, Kolko M. The molecular aspect of anti-glaucomatous eye drops - are we harming our patients? Mol Aspects Med. 2023;93:101195. doi:10.1016/j.mam.2023.101195
15. Gedde SJ, Vinod K, Wright MM, et al. American Academy of Ophthalmology Preferred Practice Pattern Glaucoma Panel. Primary Open-Angle Glaucoma Preferred Practice Pattern®. Ophthalmology. 2021;128(1):P71–P150. doi:10.1016/j.ophtha.2020.10.022
16. Lee S, Kim MK, Choi HJ, Wee WR, Kim DM. Comparative cross-sectional analysis of the effects of topical antiglaucoma drugs on the ocular surface. Adv Ther. 2013;30(4):420–429. doi:10.1007/s12325-013-0021-8
17. Gupta D, Ehrlich JR, Newman-Casey PA, Stagg B. Cost-Related Medication Nonadherence in a Nationally Representative US Population with Self-Reported Glaucoma. Ophthalmol Glaucoma. 2021;4(2):126–130. doi:10.1016/j.ogla.2020.08.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.