")
Back to Journals » Journal of Inflammation Research » Volume 17
The Effect of Systemic Immune-Inflammatory Index (SII) and Prognostic Nutritional Index (PNI) in Early Gastric Cancer
Authors Jing Y, Ren M, Li X, Sun X, Xiao Y, Xue J, Liu Z
Received 3 October 2024
Accepted for publication 26 November 2024
Published 4 December 2024 Volume 2024:17 Pages 10273—10287
DOI https://doi.org/10.2147/JIR.S499094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yaoyao Jing,1 Minghan Ren,2 Xiaoxiao Li,1 Xiaoyuan Sun,1 Yan Xiao,3 Juan Xue,2 Zimin Liu1
1Center for GI Cancer Diagnosis and Treatment, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, People’s Republic of China; 2Department of Gastroenterology, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, People’s Republic of China; 3Department of Clinical Laboratory, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, People’s Republic of China
Correspondence: Zimin Liu, Email [email protected]
Background: In recent years, the systemic immune-inflammatory index (SII) and prognostic nutritional index (PNI) have been considered potential predictors of survival outcomes in various solid tumors, including gastric cancer. However, there is a notable lack of research focusing on their prognostic implications specifically in the early stage of gastric cancer. This study aims to investigate the prognostic indicators of early gastric cancer (EGC), including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), SII, PNI, and lymph node metastasis (LNM).
Methods: In this retrospective analysis, we examined 490 patients diagnosed with EGC (pT1Nx). The peripheral blood indices of interest were SII, PNI, PLR, and NLR. The receiver operating characteristic (ROC) curves and the area under the ROC curve (AUC) were used to determine optimal cutoff values and prognostic efficacy for each parameter. Additionally, Kaplan-Meier survival curves and multivariate Cox regression models were utilized to delineate independent prognostic factors.
Results: The optimal cutoff values for SII and PNI were determined as 613.05 and 42.21, respectively. Patients in the low SII (SII-L) group demonstrated significantly higher 5-year Disease-Free Survival (DFS) and Overall Survival (OS) rates of 94.7% and 96.2%, compared to the high SII (SII-H) group (DFS: 78.7%; OS: 81.9%), with both differences proving statistically significant (P < 0.001, P < 0.001). Similarly, patients in the high PNI (PNI-H) group showed superior 5-year DFS (93.3%) and OS rates (95.1%) versus the low PNI (PNI-L) group (DFS: 71.4%; OS: 74.3%), also demonstrating statistical significance (P < 0.001, P < 0.001). Multivariate analysis identified SII, PNI, and LNM as independent prognostic factors for EGC. A combined analysis of SII, PNI, and LNM yielded a C-index of 0.723 (P = 0.008).
Conclusion: SII, PNI, and LNM are effective markers for predicting the survival outcomes of patients undergoing radical gastrectomy for EGC.
Keywords: early gastric cancer, systemic inflammatory response index, prognostic nutritional index, lymph node metastasis, prognosis
Introduction
Early gastric cancer (EGC) is defined by cancer cells invading the mucosa (T1a) or submucosa (T1b) of the gastric wall, regardless of regional lymph node metastasis (LNM). The advent of widespread endoscopic use has facilitated increased EGC detection. Data from the Chinese Surgical Alliance for Gastrointestinal Oncology indicates that EGC accounted for 19.7% of all gastric cancer cases, rising to 20.9% between 2014 and 2017.1 After radical resection, the 5-year overall survival (OS) rate for EGC can surpass 90%, yet recurrence and metastasis still occur in 1.1%–13.8% of patients.2–5 Hence, accurate prognostic assessment of individual outcomes is crucial for guiding treatment strategies and follow-up protocols in managing gastric cancer. In EGC, where tumor invasion is confined to the mucosal layer, special attention should be paid to LNM. Studies have shown that the 5-year OS rate of EGC patients with the N1 stage of LNM is significantly higher than that of patients with N2 and N3 stages of LNM.6
The Tumor, Node, Metastasis (TNM) Staging System is widely used in clinical practice to assess the biological characteristics of tumors. However, there exists a complex interplay between the tumor and the host involving inflammatory responses and nutrient metabolism. Recent investigations have underscored the prognostic significance of inflammatory markers, derived from peripheral blood counts, across diverse malignancies.7–10 Notably, NLR and PLR are extensively investigated prognostic indicators in gastric cancer.11–13 The SII, integrating NLR and PLR, provides a comprehensive assessment of systemic inflammatory status and holds potential for predicting both tumor response and prognosis in patients with gastric cancer.14 Concurrently, nutritional parameters such as albumin, body mass index (BMI), and prognostic nutritional index (PNI) are also linked to prognosis in gastric cancer patients following gastrectomy.15–17 This study aims to delve into the factors influencing prognosis among EGC patients post-radical surgery, encompassing immunoinflammatory and nutritional parameters alongside LNM.
Materials and Methods
Patient Sample
We retrospectively analyzed the clinicopathologic and follow-up data of 490 patients who were diagnosed with EGC and underwent gastrectomy and lymph node dissection at the Affiliated Hospital of Qingdao University between January 2013 and December 2018. The inclusion criteria of patients were as follows: (1) patients who underwent radical gastrectomy with R0 resection; (2) patients who received D2 lymph node dissection; (3) patients who had EGC limited to submucosal infiltration (pT1); (4) patients with complete clinicopathologic and follow-up data available. The exclusion criteria were as follows: (1) patients with distant metastases and/or other malignancies; (2) patients who received neoadjuvant chemotherapy and/or radiotherapy; (3) patients with R1 or R2 surgical margins; (4) patients with a history of autoimmune, inflammatory, or hematological disorders; (5) patients who received blood transfusions and nutritional supplements within one month before blood collection; (6) patients who died within 30 days after surgery.
Data Collection
A total of 490 patients meeting the inclusion / exclusion criteria were enrolled in this study. Postoperative outpatient review records, routine physical examination records, and yearly routine telephone follow-up were used to monitor the patients and gather data. The collected clinicopathological characteristics included age, sex, BMI, adjuvant chemotherapy, tumor location, gross type, lesion size, depth of invasion, Lymphovascular invasion (LVI), and perineural invasion. All patients underwent blood sample collection for routine laboratory tests within 7 days before surgery, with no disclosure of personal information during data collection. According to guidelines from the Japanese Gastric Cancer Association (JGCA), tumor locations were categorized as upper, middle, and lower stomach regions.18 The two classifications of gross types encompass elevated types, including EGC gross types I and IIa, and non-elevated types, which comprise EGC gross types IIb, IIc, and III.19 Depth of invasion and LNM status were assessed using the TNM staging system of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) for gastric cancer. Patients, with a mean age of 58.90 years, were stratified into ≤ 60 years and > 60 years age groups using a cutoff value of 60 years. Nutritional indicators such as the PNI and BMI were calculated as follows: PNI = albumin (g/L) + 5 × lymphocyte count (109/L), BMI = weight (kg) / height squared (m2). Patients were categorized into non-obese (BMI < 28 kg/m2) and obese (BMI ≥ 28 kg/m2) groups based on obesity criteria. Inflammation-based indices including NLR, PLR, and SII were calculated as follows: NLR = neutrophils (N) / lymphocytes (L); PLR = platelets (P) / L; SII = P × N / L.
Statistical Analysis
Statistical analyses were performed using SPSS statistical software for Windows, version 26.0 (IBM, Chicago, Illinois, USA). Receiver operating characteristic (ROC) curves were utilized to determine optimal cutoff values for inflammatory and nutritional indices. Continuous variables were assessed via t-tests, while categorical variables were analyzed using chi-square tests or Fisher’s exact tests. Survival disparities, such as 5-year disease-free survival (DFS) and OS, were evaluated using Kaplan-Meier analysis with Log rank tests. Additionally, multifactorial Cox proportional hazards modeling was applied to identify independent prognostic factors influencing 5-year DFS in EGC patients. Statistical significance was set at a two-sided P value < 0.05. The area under the ROCcurve (AUC) was employed to gauge the prognostic accuracy of each parameter for 5-year DFS. The goodness of fit was assessed using the Hosmer-Lemeshow test, where a P value > 0.05 indicated a well-fitted model.20 Decision curve analysis was conducted using R software (version 4.1.3) and various related packages to ascertain predicted net benefit thresholds and clinical effectiveness rates.21
Results
Baseline Characteristics
In this study, 490 patients diagnosed with EGC were analyzed, comprising 356 males and 134 females. The average age of the cohort was 58.90 years (range: 24 to 87 years), with 243 patients aged 60 years or older and 247 aged younger than 60 years. 409 patients (83.5%) had a BMI below 28 kg/m2, while 81 cases (16.5%) had a BMI over or equal to 28 kg/m2. The majority of tumors were located in the lower stomach (356 instances, 72.6%), followed by the middle (120 cases, 24.5%) and upper parts (14 cases, 2.9%). There were 394 cases (80.4%) of non-elevated type and 96 cases (19.6%) of elevated type. The depth of tumor invasion involved the mucosal layer in 229 cases (46.7%) and the submucosal layer in 261 cases (53.3%). 368 cases (78.8%) had a negative lymph node status, while 104 cases (21.2%) had metastases, including N1 (14.7%), N2 (4.9%), and N3 (1.6%). Based on lesion size, 298 patients (60.8%) had lesions ≤20 mm, 104 patients (21.2%) had lesions ≤30 mm, and 88 patients (18.0%) had lesions >30 mm. LVI was positive in 78 cases (15.9%) and negative in 412 cases (84.1%). Additionally, perineural invasion was present in 42 cases (8.6%), while 448 cases (91.4%) showed no invasive perineural elements. According to treatment, 151 patients (30.8%) had adjuvant chemotherapy after surgery, while 339 patients (69.2%) only had surgical resection. The specific information was displayed in Table 1.
 |
Table 1 Baseline Characteristics of 490 Patients with Early Gastric Cancer Post-Surgery |
The Optimal Cutoff Values for Inflammatory Index and Nutritional Index
ROC curve analysis was performed to ascertain the optimal cutoff values for each inflammatory and nutritional index, including NLR, PLR, SII, and PNI, which were identified as 1.88, 136.90, 613.05, and 42.21, respectively. Subsequently, patients were stratified into low and high groups according to these cutoff values. Values below 1.88 for NLR, 136.90 for PLR, 613.05 for SII, and 42.21 for PNI are categorized as the low-level group, while values equal to or above these thresholds are classified as the high-level group.
The Relationship Between SII, PNI, and Clinicopathologic Features
Among the 490 patients in the study, 401 (81.8%) were categorized into the low SII (SII-L) group, while 89 (18.2%) were placed in the high SII (SII-H) group. Analysis of clinicopathologic features revealed that the SII-H group exhibited a higher percentage of patients with tumor infiltration reaching the submucosal layer compared to the SII-L group (65.2% vs 50.6%, P = 0.013). Moreover, a greater occurrence of LNM was observed in the SII-H group (29.2% vs 19.5%, P = 0.042). However, no statistically significant differences were observed in other baseline characteristics such as sex, age, BMI, adjuvant chemotherapy, tumor location, lesion size, LVI, perineural invasion, and pathological N-staging between the SII-L and SII-H groups. Details were shown in Table 2.
 |
Table 2 The Relationship Between SII, PNI, and Clinicopathologic Features |
In this study, there were 455 patients (92.9%) in the low PNI (PNI-L) group and 35 patients (7.1%) in the high PNI (PNI-H) group. A higher percentage of patients with elevated type was observed in the PNI-H group compared to the PNI-L group (37.1% vs 18.2%, P=0.007; Table 2). Nevertheless, no significant differences were observed between the two groups in terms of other baseline characteristics.
Risk Factors for Lymph Node Metastasis
In the univariate analysis, variables such as gross type, lesion size, depth of invasion, LVI, perineural invasion, and SII were associated with LNM (Table 3). Subsequent multivariate logistic regression revealed that only depth of invasion and LVI remained independent predictors of LNM. Notably, LVI exhibited the highest odds ratio among these predictors (Table 4).
 |
Table 3 Lymph Node Metastasis Risk According to Clinicopathologic Characteristics |
 |
Table 4 Multivariate Logistic Regression Analysis of Lymph Node Metastasis |
Analysis of Prognostic Factors in Patients with Early Gastric Cancer
In this study, patients diagnosed with EGC demonstrated a favorable prognosis, achieving a 5-year DFS of 91.8% and a 5-year OS of 93.7%. In terms of survival analysis, the 5-year DFS and OS rates were significantly higher in the SII-L group at 94.7% and 96.2%, respectively, compared to the SII-H group, which had rates of 78.7% and 81.9%, respectively (P < 0.001 for both; Figure 1). Similarly, patients in the PNI-H group exhibited superior 5-year DFS and OS rates of 93.3% and 95.1%, respectively, compared to the PNI-L group, which showed rates of 71.4% and 74.3%, respectively (P < 0.001 for both; Figure 1).
 |
Figure 1 Kaplan-Meier curves illustrating 5-year Disease-Free Survival (DFS) and Overall Survival (OS) comparisons for Prognostic Nutritional Index (PNI) (panels A and B) and Systemic Immune-Inflammation Index (SII) (panels C and D). |
Univariate and multivariate analyses were conducted to identify independent prognostic risk factors for EGC recurrence. In univariate analysis, factors such as age (P = 0.003), depth of invasion (P = 0.003), pathological N-staging (P = 0.001), NLR (P < 0.001), PLR (P = 0.001), SII (P < 0.001), and PNI (P < 0.001) significantly influenced 5-year DFS in EGC patients. Conversely, variables such as sex, BMI, gross type, tumor location, adjuvant chemotherapy, lesion size, LVI, and perineural invasion showed no association with tumor recurrence (details in Table 5).
 |
Table 5 Univariate Analysis of Prognostic Risk Factors for Early Gastric Cancer |
Multivariate analysis revealed that LNM (P = 0.025), SII (P = 0.030), and PNI (P < 0.001) independently predicted increased risk of postoperative recurrence in EGC patients (Figure 2).
 |
Figure 2 Forest plot depicting multivariate Cox proportional hazards regression analysis for postoperative recurrence in patients diagnosed with early gastric cancer. |
Predictive Ability of SII and PNI
ROC curve analysis was employed to evaluate the prognostic efficacy of preoperative SII and PNI in EGC. SII demonstrated superior predictive ability (AUC = 0.637, 95% CI 0.551–0.723, P = 0.001) compared to PNI (AUC = 0.595, 95% CI 0.507–0.684, P = 0.022) and LNM stage (AUC = 0.611, 95% CI 0.525–0.697, P < 0.001) (Figure 3). Combined analysis of SII, PNI, and LNM for integrated prediction yielded a sensitivity of 0.704, a specificity of 0.697, and a C-index of 0.723 (P = 0.008) (Table 6). The Hosmer-Lemeshow test indicated a good model fit (P = 0.200). The inclusion of SII and PNI significantly enhanced the predictive accuracy of 5-year DFS, detailed in Table 6. Decision curve analysis demonstrated that the combination of SII and PNI with lymph node status for prognostic assessment had high clinical efficacy and practicality (Figure 4).
 |
Table 6 Predictive Value of SII, PNI, Pathological N-Staging, and Their Combination for Prognosis in Early Gastric Cancer |
 |
Figure 3 Receiver operating characteristic (ROC) curves evaluating the predictive value of preoperative SII, PNI, N stage of lymph node metastasis, and their combined use for postoperative prognosis in gastric cancer patients. |
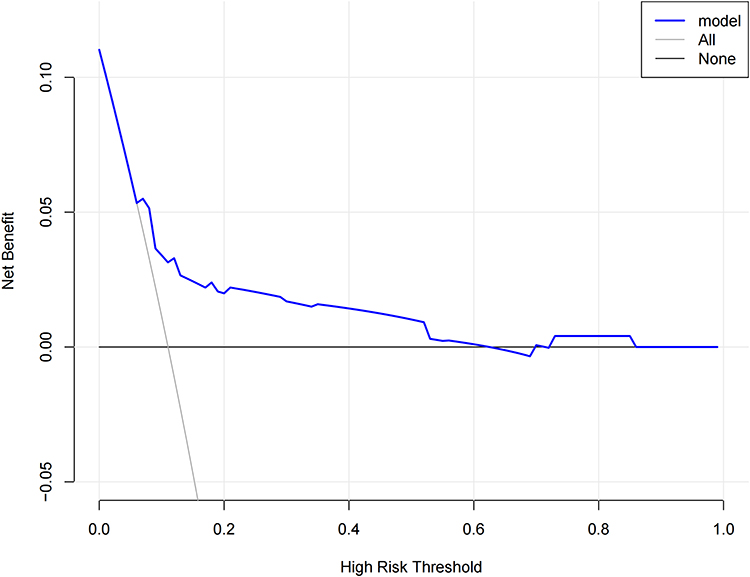 |
Figure 4 Decision curve analysis. The y-axis indicates net benefit, calculated as true benefit (gain) minus false benefit (harm). The gray line denotes the assumption where all patients progress or perish, while black horizontal lines signify the hypothesis of no patient progression or mortality. The x-axis represents threshold probability. |
Subgroup Analysis of the Prognostic Value of SII and PNI
In our subgroup analysis stratified by age, patients were categorized into non-elderly (< 60 years) and elderly (≥ 60 years) groups. Among elderly patients, the 5-year postoperative DFS rate was significantly lower in the PNI-L group compared to the PNI-H group (57.1% vs 91.3%, P < 0.001). Conversely, in the non-elderly group, there was no statistically significant difference observed in the 5-year DFS rates between the PNI-L and PNI-H groups (95.2% vs 92.9%, P = 0.280). Furthermore, within the elderly group, the 5-year DFS rate was markedly higher in the SII-L group compared to the SII-H group (92.6% vs 72.0%, P < 0.001). Similarly, in the non-elderly group, the 5-year DFS rate favored the SII-L group over the SII-H group (96.6% vs 87.2%, P = 0.004). Please refer to Figure 5 for additional details.
 |
Figure 5 5-year DFS curves comparing PNI-H group versus PNI-L group stratified by age: (A) Elderly group and (B) Non-elderly group. 5-year DFS survival curves comparing high SII-H group versus SII-L groups: (C) Elderly group and (D) Non-elderly group. |
Discussion
With the advancement of medical technology and the widespread use of endoscopy, an increasing number of gastric cancers are being detected in the early stages. According to data from the Chinese Surgical Alliance for Gastrointestinal Oncology, the proportion of EGC rose from 19.7% to 20.9% between 2014 and 2017.1 The tumor, lymph node, metastasis (TNM) staging system, developed by the American Joint Committee on Cancer (AJCC) and the International Union for Cancer Control (UICC), is widely employed by clinicians to predict prognosis and guide treatment decisions. However, the TNM staging system alone incompletely accounts for variations in patient survival outcomes. It primarily describes the tumor’s growth and metastatic potential, overlooking the intricate interplay between the tumor and the body’s environment. Therefore, there is a need for further investigation into better prognostic indicators for patients with EGC to complement TNM staging. To date, various inflammatory markers in peripheral blood, such as NLR, PLR, and SII, as well as nutritional status indicators like PNI, have been recognized as useful prognostic biomarkers for cancers, including gastric cancer.11,12,14,15 Our study aimed to investigate the clinical significance of peripheral blood inflammation and nutrition-related parameters (NLR, PLR, SII, PNI), along with clinicopathologic factors, in predicting survival outcomes for early gastric cancer.
Systemic inflammatory responses are closely linked to tumor development, especially in gastric cancer. Before cancer develops, there is a series of histological changes, beginning with persistent chronic active inflammation, followed by steps such as intestinal epithelial chemotaxis and heterogeneous hyperplasia that ultimately progress to cancer.22 Neutrophils, platelets, and lymphocytes are integral to systemic inflammation and immune responses, crucially influencing cancer development.
Tumor-associated neutrophils are a heterogeneous population characterized by plasticity, capable of displaying either anti-tumor (N1 type) or pro-tumor (N2 type) activities.23 The tumor microenvironment (TME) contains various cytokines, chemokines, and signals that can recruit. Tumor-associated neutrophils and polarize them into a pro-tumor phenotype once they enter the TME.24 This phenotypic shift can facilitate epithelial-mesenchymal transition (EMT) in gastric cancer cells through cytokine secretion,25 stimulate tumor angiogenesis,26,27 mediate immunosuppression and immune tolerance,28,29 and significantly influence tumor cell migration,30 invasion, and metastasis.31
Cancer patients often exhibit hypercoagulable blood, and cancer-related thrombocythemia is linked to adverse clinical outcomes.32 Platelets from gastric cancer patients can regulate the expression of genes involved in EMT, like matrix metalloproteinase 9 (MMP-9). This modulation subsequently increases malignant behaviors such as cancer cell proliferation, migration, invasion, and adhesion.33 Platelets can also inhibit T cell immunity through the GARP-TGFβ axis,34 contributing to cancer immune escape.35 Lymphocytes, as a fundamental component of cytotoxic immune response, play a critical role in inhibiting tumor cell growth and proliferation, as well as in killing tumor cells.36
Due to the rapid growth of the tumor, which competes for nutrients and occupies the gastrointestinal tract, along with patients experiencing gastrointestinal symptoms and other discomforts, cancer patients are susceptible to malnutrition and chronic wasting. Serum albumin, synthesized by the liver, is often used as a marker to reflect the nutritional status of the body. It is regulated by pro-inflammatory cytokines, which can be produced by both the host and the tumor and play a pivotal role in cancer progression and neovascularization.37
Therefore, a comprehensive hematologic profile incorporating these variables may serve as a prognostic indicator for survival in cancer patients.
In our investigation, we comprehensively evaluated the role of preoperative PLR, NLR, SII, PNI, and other clinicopathologic indicators in predicting LNM in EGC. Our findings revealed that PLR, NLR, SII, and PNI did not exhibit significant correlations with the occurrence of LNM. Nonetheless, previous research has suggested that PLR may possess significant predictive efficacy for LNM in EGC.38 The predictive roles of NLR and PLR in LNM among EGC patients remain subjects of ongoing debate.39
In our multifactorial logistic analysis, we identified that depth of invasion and LVI are independent risk factors for LNM in EGC, with particularly high odds ratios observed for LVI. Studies suggest that submucosal invasion strongly correlates with LNM in EGC,40 with lower rates observed in low-grade T1a compared to T1b tumors,41 attributable to the submucosa’s rich vascular and lymphatic network facilitating cancer cell dissemination. LVI positivity emerges as the most robust predictor of LNM in EGC.42 Furthermore, as LNM increases, the occurrence of LVI also elevates.43 Importantly, patients affected by LVI and LNM experience diminished survival outcomes.44 For patients with EGC showing LNM and LVI, targeted postoperative adjuvant chemotherapy significantly enhances the prognosis.45
In recent years, the SII has garnered attention as a potentially superior prognostic marker compared to other inflammatory indicators, yet its precise prognostic value in EGC remains unclear. Our study focused on patients with pT1Nx EGC, revealing both the prognostic significance of the prognostic nutritional PNI and SII as independent predictive factors. Kaplan-Meier curve analysis revealed that patients with elevated SII levels experienced reduced 5-year DFS and OS rates compared to those with lower levels. In contrast, patients with elevated PNI levels demonstrated higher 5-year DFS and OS rates. Furthermore, a separate study highlighted that among EGC patients undergoing endoscopic submucosal dissection (ESD), those with higher PNI levels experienced significantly better OS rates than their counterparts with lower PNI levels.46
In this study, the predictive capacity of SII was observed to surpass that of PNI and LNM. The combined use of these factors holds clinical relevance in prognosis prediction. These findings affirm the utility of PNI and SII in forecasting outcomes for EGC patients following radical gastric surgery. Moreover, PNI and SII could serve as valuable adjuncts to TNM staging, assessing gastric cancer patient survival, and guiding decisions regarding postoperative treatments.
In this study, subgroups of EGC patients were analyzed, revealing that elderly patients with lower PNI levels exhibited a poorer prognosis compared to those with higher PNI levels. Conversely, no statistically significant difference was observed between these groups in non-elderly patients. These findings suggest that PNI could serve as a potential prognostic indicator, specifically in elderly patients with EGC.
In addition, our study has several limitations. Firstly, it was conducted as a single-center retrospective analysis, which may introduce selection bias. Nevertheless, the substantial size of our study enhances the robustness of our evaluation regarding the prognostic significance of inflammation and nutrition indicators. Secondly, the absence of consensus on cutoff values for these indicators presents another challenge. In our investigation, we established optimal cutoff values for SII, NLR, PLR, ALI, and PNI using t-ROC curves. Therefore, future large-scale prospective studies are warranted to validate these findings comprehensively.
Conclusion
In conclusion, SII, PNI, and LNM emerge as robust predictors of survival outcomes following radical gastrectomy for EGC, demonstrating significant predictive efficacy.
Ethic Approval
The study was approved by the Ethics Committee of The Affiliated Hospital of Qingdao University (ethics approval number: QYFZWZLL29181) and informed consent was obtained from all participants. Our study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors reviewed and approved the final version of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; All authors took part in drafting, revising or critically reviewing the article; All authors gave final approval of the version to be published; All authors have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflict of interest in this work.
References
1. Miao RL, Li Z, Ji J. Current treatment status and trends of early gastric cancer in China: analyzed based on the data of China Gastrointestinal Cancer Surgery Union. Chinese J Pract Sur. 2019;39(05):419–423. doi:10.19538/j.cjps.issn1005-2208.2019.05.03
2. Lai JF, Kim S, Kim K, et al. Prediction of recurrence of early gastric cancer after curative resection. Ann Surg Oncol. 2009;16(7):1896–1902. doi:10.1245/s10434-009-0473-x
3. Kim JH, Kim HS, Seo WY, et al. External validation of nomogram for the prediction of recurrence after curative resection in early gastric cancer. Ann Oncol. 2012;23(2):361–367. doi:10.1093/annonc/mdr118
4. Saka M, Katai H, Fukagawa T, Nijjar R, Sano T. Recurrence in early gastric cancer with lymph node metastasis. Gastric Cancer. 2008;11(4):214–218. doi:10.1007/s10120-008-0485-4
5. Yuasa N, Nimura Y. Survival after surgical treatment of early gastric cancer, surgical techniques, and long-term survival. Langenbecks Arch Surg. 2005;390(4):286–293. doi:10.1007/s00423-004-0482-y
6. Wang J, Wang L, Li S, et al. Risk Factors of Lymph Node Metastasis and Its Prognostic Significance in Early Gastric Cancer: a Multicenter Study. Front Oncol. 2021;11:649035. doi:10.3389/fonc.2021.649035
7. Ma LX, Wang Y, Espin-Garcia O, et al. Systemic inflammatory prognostic scores in advanced pancreatic adenocarcinoma. Br J Cancer. 2023;128(10):1916–1921. doi:10.1038/s41416-023-02214-0
8. Golder AM, McMillan DC, Park JH, Mansouri D, Horgan PG, Roxburgh CS. The prognostic value of combined measures of the systemic inflammatory response in patients with colon cancer: an analysis of 1700 patients. Br J Cancer. 2021;124(11):1828–1835. doi:10.1038/s41416-021-01308-x
9. Rassouli A, Saliba J, Castano R, Hier M, Zeitouni AG. Systemic inflammatory markers as independent prognosticators of head and neck squamous cell carcinoma. Head Neck. 2015;37(1):103–110. doi:10.1002/hed.23567
10. Yodying H, Matsuda A, Miyashita M, et al. Prognostic Significance of Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio in Oncologic Outcomes of Esophageal Cancer: a Systematic Review and Meta-analysis. Ann Surg Oncol. 2016;23(2):646–654. doi:10.1245/s10434-015-4869-5
11. Miyamoto R, Inagawa S, Sano N, Tadano S, Adachi S, Yamamoto M. The neutrophil-to-lymphocyte ratio (NLR) predicts short-term and long-term outcomes in gastric cancer patients. Eur J Surg Oncol. 2018;44(5):607–612. doi:10.1016/j.ejso.2018.02.003
12. Zhang LX, Wei ZJ, Xu AM, Zang JH. Can the neutrophil-lymphocyte ratio and platelet-lymphocyte ratio be beneficial in predicting lymph node metastasis and promising prognostic markers of gastric cancer patients? Tumor maker retrospective study. Int J Surg. 2018;56:320–327. doi:10.1016/j.ijsu.2018.06.037
13. Hirahara T, Arigami T, Yanagita S, et al. Combined neutrophil-lymphocyte ratio and platelet-lymphocyte ratio predicts chemotherapy response and prognosis in patients with advanced gastric cancer. BMC Cancer. 2019;19(1):672. doi:10.1186/s12885-019-5903-y
14. Zhang Y, Lin S, Yang X, Wang R, Luo L. Prognostic value of pretreatment systemic immune-inflammation index in patients with gastrointestinal cancers. J Cell Physiol. 2019;234(5):5555–5563. doi:10.1002/jcp.27373
15. Migita K, Takayama T, Saeki K, et al. The prognostic nutritional index predicts long-term outcomes of gastric cancer patients independent of tumor stage. Ann Surg Oncol. 2013;20(8):2647–2654. doi:10.1245/s10434-013-2926-5
16. Yang Y, Gao P, Song Y, et al. The prognostic nutritional index is a predictive indicator of prognosis and postoperative complications in gastric cancer: a meta-analysis. Eur J Surg Oncol. 2016;42(8):1176–1182. doi:10.1016/j.ejso.2016.05.029
17. Han WX, Chen ZM, Wei ZJ, Xu AM. Preoperative pre-albumin predicts prognosis of patients after gastrectomy for adenocarcinoma of esophagogastric junction. World J Surg Oncol. 2016;14(1):279. doi:10.1186/s12957-016-1035-x
18. Japanese Gastric Cancer A. Japanese Classification of Gastric Carcinoma - 2nd English Edition. Gastric Cancer. 1998;1(1):10–24. doi:10.1007/s101209800016.
19. Nakamura K, Sugano H, Takagi K. Carcinoma of the stomach in incipient phase: its histogenesis and histological appearances. Gan. 1968;59(3):251–258.
20. Kramer AA, Zimmerman JE. Assessing the calibration of mortality benchmarks in critical care: the Hosmer-Lemeshow test revisited. Crit Care Med. 2007;35(9):2052–2056. doi:10.1097/01.Ccm.0000275267.64078.B0
21. Vickers AJ, Cronin AM, Elkin EB, Gonen M. Extensions to decision curve analysis, a novel method for evaluating diagnostic tests, prediction models and molecular markers. BMC Med Inform Decis Mak. 2008;8(1):53. doi:10.1186/1472-6947-8-53
22. Correa P, Piazuelo MB. The gastric precancerous cascade. J Dig Dis. 2012;13(1):2–9. doi:10.1111/j.1751-2980.2011.00550.x
23. Fridlender ZG, Sun J, Kim S, et al. Polarization of tumor-associated neutrophil phenotype by TGF-beta: “N1” versus “N2” TAN. Cancer Cell. 2009;16(3):183–194. doi:10.1016/j.ccr.2009.06.017
24. Zhang X, Shi H, Yuan X, Jiang P, Qian H, Xu W. Tumor-derived exosomes induce N2 polarization of neutrophils to promote gastric cancer cell migration. Mol Cancer. 2018;17(1):146. doi:10.1186/s12943-018-0898-6
25. Li S, Cong X, Gao H, et al. Tumor-associated neutrophils induce EMT by IL-17a to promote migration and invasion in gastric cancer cells. J Exp Clin Cancer Res. 2019;38(1):6. doi:10.1186/s13046-018-1003-0
26. Deryugina EI, Zajac E, Juncker-Jensen A, Kupriyanova TA, Welter L, Quigley JP. Tissue-infiltrating neutrophils constitute the major in vivo source of angiogenesis-inducing MMP-9 in the tumor microenvironment. Neoplasia. 2014;16(10):771–788. doi:10.1016/j.neo.2014.08.013
27. Li J, Xia Y, Sun B, et al. Neutrophil extracellular traps induced by the hypoxic microenvironment in gastric cancer augment tumour growth. Cell Commun Signal. 2023;21(1):86. doi:10.1186/s12964-023-01112-5
28. Wang TT, Zhao YL, Peng LS, et al. Tumour-activated neutrophils in gastric cancer foster immune suppression and disease progression through GM-CSF-PD-L1 pathway. Gut. 2017;66(11):1900–1911. doi:10.1136/gutjnl-2016-313075
29. Shan ZG, Zhao YL, Zhang JY, et al. FasL(+) PD-L2(+) Identifies a Novel Immunosuppressive Neutrophil Population in Human Gastric Cancer That Promotes Disease Progression. Adv Sci. 2022;9(5):e2103543. doi:10.1002/advs.202103543
30. Patel S, Fu S, Mastio J, et al. Unique pattern of neutrophil migration and function during tumor progression. Nat Immunol. 2018;19(11):1236–1247. doi:10.1038/s41590-018-0229-5
31. Swierczak A, Mouchemore KA, Hamilton JA, Anderson RL. Neutrophils: important contributors to tumor progression and metastasis. Cancer Metastasis Rev. 2015;34(4):735–751. doi:10.1007/s10555-015-9594-9
32. Wang YH, Kang JK, Zhi YF, et al. The pretreatment thrombocytosis as one of prognostic factors for gastric cancer: a systematic review and meta-analysis. Int J Surg. 2018;53:304–311. doi:10.1016/j.ijsu.2018.03.084
33. Saito R, Shoda K, Maruyama S, et al. Platelets enhance malignant behaviours of gastric cancer cells via direct contacts. Br J Cancer. 2021;124(3):570–573. doi:10.1038/s41416-020-01134-7
34. Rachidi S, Metelli A, Riesenberg B, et al. Platelets subvert T cell immunity against cancer via GARP-TGFβ axis. Sci Immunol. 2017;2(11). doi:10.1126/sciimmunol.aai7911
35. Metelli A, Wu BX, Riesenberg B, et al. Thrombin contributes to cancer immune evasion via proteolysis of platelet-bound GARP to activate LTGF-β. Sci Transl Med. 2020;12(525):4860. doi:10.1126/scitranslmed.aay4860
36. Ray-Coquard I, Cropet C, Van Glabbeke M, et al. Lymphopenia as a prognostic factor for overall survival in advanced carcinomas, sarcomas, and lymphomas. Cancer Res. 2009;69(13):5383–5391. doi:10.1158/0008-5472.Can-08-3845
37. Balkwill F. Tumour necrosis factor and cancer. Nat Rev Cancer. 2009;9(5):361–371. doi:10.1038/nrc2628
38. Wu H, Liu W, Yin M, et al. A nomogram based on platelet-to-lymphocyte ratio for predicting lymph node metastasis in patients with early gastric cancer. Front Oncol. 2023;13:1201499. doi:10.3389/fonc.2023.1201499
39. Zhu GS, Tian SB, Wang H, et al. Preoperative Neutrophil Lymphocyte Ratio and Platelet Lymphocyte Ratio Cannot Predict Lymph Node Metastasis and Prognosis in Patients with Early Gastric Cancer: a Single Institution Investigation in China. Curr Med Sci. 2018;38(1):78–84. doi:10.1007/s11596-018-1849-6
40. Milhomem LM, Milhomem-Cardoso DM, da Mota OM, et al. Risk of lymph node metastasis in early gastric cancer and indications for endoscopic resection: is it worth applying the east rules to the west? Surg Endosc. 2021;35(8):4380–4388. doi:10.1007/s00464-020-07932-7
41. Pokala SK, Zhang C, Chen Z, et al. Lymph node metastasis in early gastric adenocarcinoma in the United States of America. Endoscopy. 2018;50(5):479–486. doi:10.1055/s-0043-122379
42. Nustas R, Messallam AA, Gillespie T, et al. Lymph node involvement in gastric adenocarcinoma. Surg Endosc. 2022;36(6):3876–3883. doi:10.1007/s00464-021-08704-7
43. Zhang F, Chen H, Luo D, et al. Lymphovascular or perineural invasion is associated with lymph node metastasis and survival outcomes in patients with gastric cancer. Cancer Med. 2023;12(8):9401–9408. doi:10.1002/cam4.5701
44. Choi S, Song JH, Lee S, et al. Lymphovascular Invasion: traditional but Vital and Sensible Prognostic Factor in Early Gastric Cancer. Ann Surg Oncol. 2021;28(13):8928–8935. doi:10.1245/s10434-021-10224-6
45. Takeuchi A, Ojima T, Katsuda M, et al. Venous Invasion Is a Risk Factor for Recurrence of pT1 Gastric Cancer with Lymph Node Metastasis. J Gastrointest Surg. 2022;26(4):757–763. doi:10.1007/s11605-021-05238-0
46. Iwai N, Dohi O, Naito Y, et al. Impact of the Charlson comorbidity index and prognostic nutritional index on prognosis in patients with early gastric cancer after endoscopic submucosal dissection. Dig Endosc. 2018;30(5):616–623. doi:10.1111/den.13051
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Systemic Inflammatory Response Index and Pan-Immune-Inflammation-Value with Long-Term Adverse Cardiovascular Events in ST-Segment Elevation Myocardial Infarction Patients After Primary Percutaneous Coronary Intervention
Liu Y, Liu J, Liu L, Cao S, Jin T, Chen L, Wu G, Zong G
Journal of Inflammation Research 2023, 16:3437-3454
Published Date: 14 August 2023
Prognostic Nutritional Index (PNI) as a Predictor in Patients with Metabolic Syndrome and Heart Failure
Zhang X, Zhang J, Liu F, Li W, Zhang T, Fang B, Zhang Z, Xie Q, Yang Y, Li X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2503-2514
Published Date: 18 August 2023
Prognostic Value of Systemic Inflammatory Response Index for the Prognosis of Diabetic Maintenance Hemodialysis Patients: A Retrospective Observational Study
Yan Z, Li L
International Journal of General Medicine 2023, 16:3613-3622
Published Date: 21 August 2023
Role of the Systemic Inflammatory Response Index in Predicting Disease Severity and Prognosis in Idiopathic Pulmonary Arterial Hypertension
Gao L, Zhang S, Zhao Z, Zhao Q, Yang T, Zeng Q, Zhang Y, Li X, Huang Z, Duan A, Luo Q, Liu Z
Journal of Inflammation Research 2024, 17:447-460
Published Date: 22 January 2024
Correlation of Prognostic Nutritional Index and Systemic Immune-Inflammation Index with the Recurrence and Prognosis in Oral Squamous Cell Carcinoma with the Stage of III/IV
Ye M, Zhang L
International Journal of General Medicine 2024, 17:2289-2297
Published Date: 20 May 2024