")
Back to Journals » Clinical Interventions in Aging » Volume 19
The Effect of Two Somatic-Based Practices Dance and Martial Arts on Irisin, BDNF Levels and Cognitive and Physical Fitness in Older Adults: A Randomized Control Trial
Authors Hola V, Polanska H , Jandova T, Jaklová Dytrtová J, Weinerova J, Steffl M, Kramperova V, Dadova K , Durkalec-Michalski K, Bartos A
Received 7 August 2024
Accepted for publication 25 October 2024
Published 6 November 2024 Volume 2024:19 Pages 1829—1842
DOI https://doi.org/10.2147/CIA.S482479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Veronika Hola,1 Hana Polanska,1 Tereza Jandova,1 Jana Jaklová Dytrtová,1 Josefina Weinerova,2 Michal Steffl,1 Veronika Kramperova,1 Klara Dadova,1 Krzysztof Durkalec-Michalski,3 Ales Bartos2,4
1Faculty of Physical Education and Sport, Charles University, Prague, Czech Republic; 2University Hospital Kralovske Vinohrady, Department of Neurology, Prague, Czech Republic; 3Department of Sports Dietetics, Poznan University of Physical Education, Poznań, 61-871, Poland; 4Third Faculty of Medicine, Charles University, Department of Neurology, Prague, Czech Republic
Correspondence: Michal Steffl, Faculty of Physical Education and Sport Charles University, José Martího 31, Prague, 162 52, Czech Republic, Tel +420778701882, Email [email protected]
Background: Maintaining healthy brain function during ageing is of great importance, especially for the self-sufficiency of older adults. The main aim of this study was to determine the effects of dance and martial arts on exerkines Brain Derived Neurotrophic Factor (BDNF) and irisin blood serum levels.
Methods: This randomized controlled trial examined the effects of dance and martial arts on serum Brain-Derived Neurotrophic Factor (BDNF) and irisin levels, as well as cognitive function, mood, and physical measures in older adults. Seventy-seven independently living older adults (mean age 70.3± 3.8 years) were randomized into three groups: dance (DG), martial arts (MaG), and control (CG), followed over 12 weeks. Generalized linear models were used to assess the interventions’ effects.
Results: There was a significant increase in BDNF levels in both the DG (1.8 ± 4.9, p < 0.05) and MaG (3.5 ± 6.3, p < 0.05), while CG experienced a decrease (− 4.9 ± 8.2, p < 0.05). Between-group effects were significant for BDNF, with DG and MaG showing higher levels than CG (p < 0.05). No significant changes in irisin levels were found. Cognitive performance, particularly attention and mental flexibility (measured by the Trail Making Test A and B), significantly improved in the DG compared to CG (p < 0.05). Additionally, participants in DG showed improved mood based on the Geriatric Depression Scale (p < 0.05) compared to CG. Anthropometric T-scores were significantly associated with changes in irisin levels (p < 0.05) after intervention.
Conclusion: The study found that dance and martial arts upregulated BDNF levels, with dance showing notable improvements in cognitive function and mood in older adults. Changes in anthropometric measures were linked to increased irisin levels. These findings suggest that both dance and martial arts may promote healthy brain function in aging populations.
Trial Registration: NCT05363228.
Keywords: cognitive domains, ageing, cognitive performance, cognitive function, serum, biomarkers
Introduction
Physical activity (PA) has a positive effect on health and can ease some neurological conditions such as depression, epilepsy, stroke, Alzheimer’s (AD) and Parkinson’s disease (PD).1–4 The healthy older adult population has also demonstrated improvements in cognitive functions after PA,5 which is believed to be mediated by exerkines (cytokines secreted by organs in response to exercise).6 BDNF is one of the most prominent neurotrophic and neuroprotective exerkines in the central nervous system (CNS).7 BDNF is believed to be mediated by irisin, a myokine cleaved from the fibronectin type III domain-containing 5 (FNDC5) protein secreted by muscles in response to exercise.8–11
In the last decade, a holistic point of view has defined the need to link the body with psycho-emotional experience; ie the need for PA that improves physical function but also considers social relationships, emotional experience, and body awareness.12 These somatic approaches are appropriate for enhancing cognitive domains because they are designed to improve sensitivity, alter habitual movement patterns through sensory perception13 and include multi-faceted activities such as cognition, emotion, coordination, visual-spatial orientation, social interaction, and kinesthetic empathy.14,15 An essential feature of dance is the synchronization of movement and the connection to time through musical rhythms,16 promoting the imagery of spontaneous movement patterns, memories, and recollections.17 On the other hand, martial arts are mostly moderate-intensity group activities that allow older adults to exercise in a social environment and communicate with other participants in a similar way to dancing.15
In fact, both dance and martial arts are universal human behaviors associated with group rituals,18 and both have been shown to improve cognitive function in older adults.19–22 Moreover, dance could be superior to other physical activities23 because of its complexity of coordination.24 On the other hand, there is evidence that long-term dancing (more than 10 years) helped older individuals maintain healthy aging to the same extent as an adapted PA program.25 Therefore, it is important to distinguish between different types of dances and approaches. For example, a recent randomized controlled trial (RCT) found decreased BDNF and increased irisin after folk dance and balance training, accompanied by improved physical performance, glucose homeostasis and blood pressure.26 In this study, we focused on somatic practices, acknowledging their distinct nature and approaches to bodily movement.
To our knowledge, this is the first RCT to investigate the effect of two somatic-based practices, dance and martial arts on the secretion of chosen exerkines and cognitive performance. The main aim of our study was to determine the magnitude of the effect of the dance and martial arts on serum BDNF and irisin levels and to estimate whether changes in serum BDNF and irisin levels, anthropometrics, and physical performance were associated with changes in cognitive performance in older adults.
Methods
A randomized, three-arm, single-blind, controlled trial was conducted in two centers: 1) University Hospital Kralovske Vinohrady (UHKV), Charles University, Third Faculty of Medicine, Prague and 2) Charles University, Faculty of Physical Education and Sport, Prague, from May 2021 to December 2022. The study was approved by the Faculty of Physical Education and Sport ethics committees and the University Hospital Kralovske Vinohrady, and all the participants signed an informed consent. The trial was registered on clinicaltrials.gov with registration ID NCT05363228 03/05/2022.
Participants
Seventy-seven independently living older adults participated in the study. Inclusion criteria were age 65–80 years, no mobility limitations, less active according to the Rapid Assessment of Physical Activity (RAPA),27 complete independence in activities, normal score according to the Eight-item Informant Interview to Differentiate Aging and Dementia (AD8-CZ)28 and good vision and hearing. Exclusion criteria were as follows: neurological diseases (epilepsy, significant head injury, stroke, brain surgery, brain tumor, etc)., psychiatric diseases or treatments (schizophrenia, bipolar disorder, drug addiction, alcoholism, etc)., organ failure (heart, kidney, etc)., oncological diseases in the last five years or patients after chemotherapy or radiotherapy, surgery under general anesthesia in the last three months, use of cognitive enhancers. Participants who reported a much higher than average level of PA according to the RAPA were excluded. Depression was not an exclusion criterion. We set our sample size at a minimum total number of participants of N = 68 based on an a priori power analysis using G*Power 3.1.29 Based on prior findings,15,30 we sought to detect a medium effect size (f2 = 0.15) with 80% power and a probability of error of 0.05.
Trial Design
Participants were randomly assigned to a dance group (DG) and control group (CG) in the first year of the study and to a martial arts group (MaG) and CG in the second year. 12-week interventions lasted 90 minutes per session, twice a week. This amount was based on the WHO recommendation for older adults of at least 150–300 minutes of moderate-to-vigorous intensity activity throughout the week for substantial health benefits.31 Simple randomization based on a single sequence of random assignments using a shuffled deck of cards (even-numbered control, odd-numbered intervention) was used each year. AB generated the random allocation sequence. AB enrolled and allocated participants to interventions. Each participant was examined at the University Hospital Kralovske Vinohrady for cognitive assessment and at the Faculty of Physical Education and Sport for physical fitness testing. Blood samples were taken during the visit to the University Hospital Kralovske Vinohrady. Participants completed cognitive tests and physical fitness batteries, self-reported depression levels, functional status and years of education. The evaluators responsible for administering the tests were blinded to the participants’ assigned interventions, and the instructors (dance or martial arts) were not involved in administering the pre- and post-assessments. After all measurements, participants followed the intervention/maintenance of daily activities for 12 weeks, beginning in August (pre-test) and ending in December (post-test).
Exercise Interventions
Dance
The interventions took place twice a week, lasted 90 minutes per session, and lasted 12 weeks from September to November 2021. The location and structure of each session were the same and adapted to the group of older adults.
Characteristics of the dance sessions: energy expenditure is mostly aerobic and intermittent, with varying intensity and global muscle involvement and dynamic muscle activity.
Each session consisted of a 15-minute welcome in a circle (attention, breathing, body awareness, landing, grounding, relationships with others and with the environment through observation and rhythmic patterns) followed by a 30-minute warm-up technique (concerning the body on an anatomical level, including developmental pattern exercises, bones, muscles, fasciae, skin structures awareness through touch, stretching or resistance). Peek of the class included 30 minutes of controlled improvisation based on different choreographic scores, addressing different areas (spatial trajectories, shaping, walking, expressive qualities of movement, props, phrasing, attention, active participation, and relationships). The session ended with 15 minutes of cool-down (breathing, focusing on oneself) and verbal reflection. The motivation to move in a particular but individual way is carefully prepared and facilitated through verbal scores, suggestions and invitations based on imagination, stories, symbolism, or choreographic scores. Initially, the sessions were based on mirroring, imitation and clear identification of movement or spatial pathways, gradually giving way to creativity, spontaneity, and improvisation. A qualified professional dance teacher prepared, facilitated, and supervised each session.
Martial Arts
Like the dance intervention, the martial arts intervention took place twice a week, lasted 90 minutes per session and ran for 12 weeks; however, it took place from September to November 2022. Each session was designed specifically for the older adults, considering their needs and abilities and creating a supportive environment. Each session consisted of a 15-minute welcome and evaluation of the previous session while walking. This was followed by 30 minutes of muscle activation through warm-up. The warm-up always started from head to tail and then moved to a warm-up on the floor. The session included games that verbally motivated people to move through imagination. After the game, the main 30-minute session began with punching training, moving from shadow work on the palms to pad work, then to bags and then back to pair work with pad work. As soon as the palms were tired enough, the situation was relieved with a game or activity that released the whole arm. After a few lessons, the exercise also focused on the lower limbs and kicks. This was followed by more work in pairs or the entire group. A model situation was usually played out - how to solve it with a punch, kick or other maneuver that was the session’s content. This part was followed by exercise in the form of Tai Chi, or more specifically, chakra activation or relaxation of the part of the muscle most stressed during the lesson. This part aimed to improve flexibility, balance, and muscle strength, reduce stress and anxiety, and support cognitive function. As with the dance intervention, the session ended with 15 minutes of cool-down.
Control Group
In the CG, participants were either placed on a waiting list. The benefits of cooperation in the study were joining the exercise group of their choice, dancing or martial arts after the trial, or receiving a financial reward. In the CG, participants were asked to maintain their usual lifestyle as fewer active individuals according to RAPA were selected for the study, no specific recommendations for physical activity were required.
Serum Sample Collection and Preparation
During the first and third visit 9 mL of venous blood was drawn within the week, no earlier than 48 hours pre and post-intervention, from the antecubital vein of the arm and collected into Vacutainer tubes between 7.30 a.m. and 9 a.m. Participants were advised to refrain from unusual or intense PA for at least 24 hours prior to collection.32
The samples were then stored at room temperature for a maximum of 60 minutes to facilitate clotting and obtain high-quality serum.33 Sample collection, clotting time and storage was performed by an experienced nurse and laboratory technician according to University Hospital standards.
After, the blood samples were separated by centrifugation at 1500×g for 10 minutes at 20°C and stored frozen at −80°C until assayed. To estimate BDNF and irisin serum levels, we used the enzyme-linked immunosorbent assay (ELISA) kits in the Microplate Photometer HiPo MPP-96 (BioSan) reader. For the BDNF analysis, we used an ELISA kit from Thermofisher SCIENTIFIC (USA). The samples were diluted 5 times before analysis to fit the concentration range declared by the producer. The measured absorbance was recalculated according to the calibration curve and converted to the concentration in the sample. Irisin was analyzed using a kit from Sigma-Aldrich, Germany. The sample was not diluted; therefore, the measured absorbance corresponded directly to the concentration of irisin in the sample according to the calibration curve.
Cognitive Measures
Following a small snack immediately after the blood collection, participants completed a battery of neuropsychological tests in a quiet room through trained research team members who administered it under the supervision of a psychologist. The Rey Auditory Verbal Learning Test (RAVLT) assessed verbal memory and learning abilities. From RAVLT, we used the tests of immediate short-term memory (A1), as well as the ability and strategies to learn new information (∑A).34–36 We used two fluency verbal tests initially developed by Thurstone37 1) the phonemic fluency test of words with the initial letter “P” and 2) the animal fluency test that also evaluates semantic memory in addition to language, both under time constraints of 60 seconds. The subject is asked to say as many words as possible under a given condition and in a specified time frame. More words demonstrate better performance.38 The Digit Symbol (DS) subtest of the Wechsler Adult Intelligence Scale (WAIS-III) was used to test processing speed. The DS subtest consists of a key consisting of the numbers 1–9, each paired with a unique, easily drawn symbol such as a “-”, “=” or “כ”. The numbers 1–9 series are presented below the key in random order and repeated several times. The subject then has 120 seconds to fill in the corresponding symbol for each number.39,40 The Trail Making Test (TMT) in both versions A and B was used to assess attention and mental flexibility. In TMT A, the subject uses a pencil to connect a series of 25 encircled numbers in numerical order. In part B, the subject connects 25 encircled numbers and letters in numerical and alphabetical order, alternating between numbers and letters. For example, the first number, “1”, is followed by the first letter, “A”, then the second number, “2”, then the second letter, “B”, etc. Speed was measured, and participants were asked to complete the test as quickly as possible, with less time, which meant better performance on both tests.41–43
Self-Report Subjective Questionnaires
The battery included the Geriatric Depression Scale (GDS) questionnaire to assess their mood over the previous three months and after the trials. Scores on the GDS range from 0 to 15. The higher the score, the more depressed the responses on the GDS.44 The Questionnaire of Functional State (FAQ-CZ)45 was used to assess to what extent they were able to carry out everyday activities. The FAQ-CZ consists of 10 items and is scored on a 0–3-point scale. The raw score of the FAQ-CZ was used to calculate the percentage of independence.
Anthropometric and Strength Measures
During the second and fourth visits, the anthropometric and strength measurements were conducted in the morning within the week pre and post-intervention. Height was measured using a SECA 213 portable stadiometer, and weight and body composition were measured using bioelectrical impedance (InBody 720, Biospace Co., Ltd. Korea). Skeletal muscle mass (SMM) and fat estimations were obtained from the InBody device. Skeletal muscle index (SMI) was calculated as SMM (kg)/height2 (m2).46 Handgrip strength was measured using a TKK 5401 digital dynamometer (Takei, Japan). The best value from the three trials was used. The isometric knee extensor strength of the dominant limb was tested using a Humac Norm dynamometer (Cybex CSMI, Stoughton, MA). Prior to testing, participants completed a supervised general warm-up. They were tested according to standardized guidelines. Gait speed was assessed using the 4-metre walk test,47 and the chair stand was measured as time for 5 repetitions.48
Data Analysis
Means and standard deviations (SDs) were calculated for each continuous variable, and proportions for each categorical variable. We then used the Kolmogorov–Smirnov test to test the normality of the distribution of each continuous variable. As the normality assumption was violated in most of the variables, we used non-parametric methods in our analyses. Kruskal–Wallis test and chi-squared tests were used to test for similarity between groups on baseline measures. We then calculated T-scores from each cognitive, anthropometric and muscle strength variable as T-score = z*10 + 50, where z-score was calculated as z-score =  , where x is the raw score,
, where x is the raw score,  is the mean of the study sample and SD is the standard deviation of the study sample. From the individual T-scores, we calculated the average T-scores for each domain - cognitive, anthropometric, and physical. The Wilcoxon signed-ranks test was used to test for within-group differences at pre-post. Generalized linear models for gamma with log link distribution adjusted for age and pre-intervention levels of tested dependent variables were used as the main tool to test the effect of the intervention. In addition, generalized linear models for gamma with log link distribution were used to examine the association between changes in BDNF and irisin levels and changes in mean z-scores of cognitive domains, anthropometric and strength measures, controlling for the effect of the intervention groups. All analyses and graphs were performed using IBM SPSS Statistics 24.
is the mean of the study sample and SD is the standard deviation of the study sample. From the individual T-scores, we calculated the average T-scores for each domain - cognitive, anthropometric, and physical. The Wilcoxon signed-ranks test was used to test for within-group differences at pre-post. Generalized linear models for gamma with log link distribution adjusted for age and pre-intervention levels of tested dependent variables were used as the main tool to test the effect of the intervention. In addition, generalized linear models for gamma with log link distribution were used to examine the association between changes in BDNF and irisin levels and changes in mean z-scores of cognitive domains, anthropometric and strength measures, controlling for the effect of the intervention groups. All analyses and graphs were performed using IBM SPSS Statistics 24.
Results
174 people completed the web form, and 150 met the study criteria. We then selected 77 participants whose written PA was 2 out of 5 (highest PA) according to the RAPA. 77 older adults were randomly assigned to three groups - DG, MaG and CG. During the interventions, 34.4% of participants dropped out (Figure 1). The mean age of participants was 70.3 (3.8) years, and they were deemed non-obese, with a mean BMI of 26.7 (4.9) and higher education levels. The majority of the participants, 83.1%, were women. Overall adherence to the intervention was 76.6%. The highest dropout rate was 36.0% in MaG (Table 1).
 |
Table 1 Descriptive Characteristics of the Study Participants |
 |
Figure 1 Flow chart of study design. |
There were no significant changes in serum irisin levels in any of the groups, although a greater reduction in irisin was observed in the CG. The 12-week interventions resulted in a significant increase in serum BDNF levels in MaG (p < 0.05), whereas there was a significant decrease in CG. The between-group effect was significant for BDNF levels in both DG and MaG compared to CG (p < 0.05). In the cognitive domain, represented by T-scores, there was a significant improvement after the dance intervention (p < 0.05), and the between-group effect was significant in DG compared to CG (p < 0.05). Participants’ performance on the RAVLT A1 deteriorated significantly (p < 0.05) in CG after 12 weeks, but there was no significant between-group effect. The between-group effect was significant in DG compared to CG (p < 0.05) in TMT A. There was a significant improvement in TMT-B in the DG (p < 0.05), and the between-group effect was also significant compared to the CG (p < 0.05). Participants increased their gait speed ability after the dance intervention but not significantly compared to CG. Finally, there was an improvement in GDS in the DG (p < 0.05), and the between-group effect was significant compared to the CG (Table 2). With the exception of TNT B, DS, physical T-scores and handgrip, all pre-treatment measures were significantly associated with post-intervention change, meaning that with few exceptions, the lower the serum level or test performance, the greater the change predicted. Changes in the levels of selected variables for individual participants are shown in Figure 2, with the solid line indicating improvement and the dashed line indicating deterioration.
 |
Table 2 Pre and Post Measures and Changes in All Tested Variables |
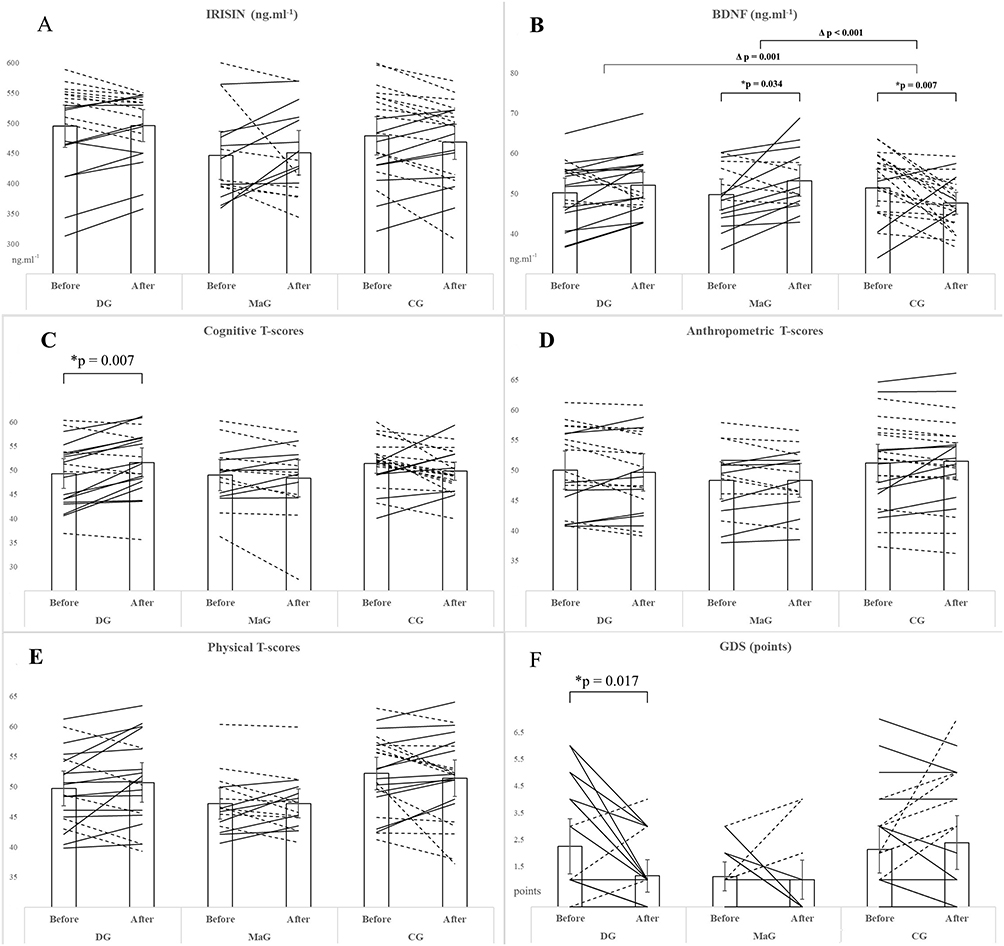 |
Figure 2 Pre and post means with 95% CIs and changes in levels of selected variables for individual participants by study group. (A) Irisin (ng.mL−1), (B) BDNF (ng.mL−1), (C) Cognitive T-scores, (D) Anthropometric T-scores, (E) Physical T-scores, (F) GDS (points); *Wilcoxon Signed Ranks Test; Δ Generalized linear models for gamma with log link distribution adjusted for age and pre-intervention level. |
According to the generalized linear models of the association between changes in BDNF and irisin levels and changes in mean cognitive domain T-scores, only anthropometric T-scores were significantly associated with changes in irisin levels (p = 0.026). There was no association with any other score changes after the intervention.
Discussion
This is the first RCT to investigate exerkines (irisin and BDNF) blood level changes concerning cognitive and physical fitness in healthy older adults after a 12-week dance and martial arts intervention (MaG) program. We found a significant increase in serum BDNF levels in MaG group and a significant decrease in serum BDNF in the control group (CG). Moreover, we found a significant improvement in cognitive T-scores, TMT – A and TMT – B after the dance intervention. On the other hand, performance on the RAVLT A1 in CG deteriorated significantly. Our results are largely in consensus with numerous studies which suggested that regular exercise is associated with improved memory, enhanced cognitive flexibility, physical performance, and mood due to elevated levels of some prominent exerkines.
Exerkines Levels
Exerkines are cytokines that are released in response to acute bouts of exercise, but chronic exercise also leads to changes in circulating humoral factors, even during periods of rest. These changes suggest that exerkine levels may serve as a marker of long-term adaptations to regular physical activity, highlighting the lasting effects of chronic training on the body’s physiological systems.49
The FNDC5/irisin effect on brain function was investigated only recently,50 and its beneficial effect has been proven particularly in AD patients.51 Our recent meta-analysis showed that long-term PA and exercise might increase irisin blood levels primarily in specific populations, including healthy and obese older adults; however, the results of individual studies exhibited high heterogeneity, which must be taken into account when interpreting irisin data.52 Our results did not confirm a significant change in serum irisin levels in any of our intervention groups, although a significant reduction in irisin was observed in the CG. In humans, some studies have shown increases in irisin levels in men following cardiovascular exercise,8,53 while others indicated no significant effect.54–56 The variability in findings may be attributed to the timing of sample collection, as irisin concentrations have been shown to exhibit temporal fluctuations following acute exercise. Specifically, irisin levels are modulated by acute physical activity for up to 48 hours post-exercise, which may account for inconsistencies in measurement outcomes across studies.57
Additionally, a recent meta-analysis reporting the effect of resistance exercise on irisin levels described that irisin levels significantly increased in PA lasting less than 12 weeks and decreased in PE lasting longer than 16 weeks.58 Other meta-analyses confirm that resistance training is crucial for increasing circulating irisin, especially in older adults.59,60 Rodziewicz-Flis et al26 also reported a significant increase in irisin serum levels after 12 weeks of folk dance. We assume that the nature of our dance intervention, based on perception and body connection rather than resistance training principles, could explain this difference between the results of both studies. In fact, folk dance can be regarded as a type of resistance training that focuses on leg strength, which was demonstrated in folk dancers when compared to healthy peers.61
It is suggested that peripheral PA-induced irisin can pass through the blood-brain barrier and influence BDNF levels.62 However, it remains unknown which neuronal receptor induces this pathway after being activated by irisin.63 However, it is postulated that the faciliatory effect of irisin on brain activity may be indirect by the induction of a rise in BDNF levels.64 In fact, our 12-week interventions resulted in a significant increase in serum BDNF levels in MaG and a significant decrease in CG. The Δ post-pre changes were positive in both intervention groups and negative in CG, which was significant between each intervention group compared to CG. This agrees with recent studies, where the peripheral concentration of BDNF significantly increased following the judo training compared with the control group in older people65 and where regular Taekwondo training improved cognitive function and increased BDNF levels in older women.66 Marinus et al67 demonstrated that resistance training is an essential component of the PA program in older adults to increase baseline BDNF levels; however, Dinoff et al68 did not find an effect of chronic resistance training on BDNF levels, but of aerobic exercise training. On the other hand, Rodziewicz-Flis et al26 found decreased levels of BDNF after balance training and folk dance. Possible reasons for this inconsistency include population heterogeneity, differences in type, intensity, and duration of the exercise intervention, and BDNF measurement from different blood components such as serum or plasma.69 We hypothesize that both of our somatic-based interventions exhibit greater similarities to aerobic training characteristics than resistance training.
More importantly, it was shown that serum BDNF concentrations systematically vary over the year, increasing in the spring-summer period and decreasing in the autumn-winter period. This finding is important as subtle effects of season on depressive behaviors have been described and long-known.70 Research studies have demonstrated that BDNF level in peripheral blood is correlated negatively with the severity of depression in rodents and humans.71,72 Our results did not show significant increases in serum BDNF after the dance intervention, but a significant decrease in depressive signs in DG assessed by GDS was observed, confirming that dance can indeed ameliorate mood in older adults and reduce depressive signs.73–75 Teixeira-Machado et al76 claim that dance practice improves neuroplasticity, and scientists link endurance exercise with BDNF expression in the brain concretely showing that neuroplasticity could well be induced by acute or chronic exposure to PA.7,77–79
Anthropometrics and Physical Fitness
Our study only found significant improvements in gait speed after the dance intervention. There were no other improvements in physical or anthropometric measures. However, regarding the association between selected variables, anthropometric T-scores Δ were significantly associated with irisin without group effect. Planella-Farrugia et al80 suggest that irisin may be considered a marker for improved muscular performance in older adults. For example, irisin correlates with muscle quality in Charcot-Marie-Tooth patients as a biomarker of muscle mass and strength loss.81 However, Baek et al82 did not observe the association between irisin serum level and clinical muscle parameters in humans. On the other hand, BDNF’s neuroprotective properties could indirectly impact muscle strength by promoting effective neuromuscular communication and thus preventing muscle weakness or atrophy.83,84 Higher BDNF levels have been associated with increased activation of fast-twitch muscle fibers, which generate force and power,85 primarily through its role in promoting muscle adaptation, growth, and overall function.86–88
Cognitive Fitness
Recently, cognition has been associated with frailty,89 impaired steady balance and poor mental flexibility in older people.90 Dance and other sensory-rich movement practices attract (neuro)science because they are complex activities that support adaptation to our environment during ageing.91 It includes self-managing based on soft skills such as connecting with intuition, promoting emotional and physical integration, self-esteem, empathy, mutual validation, and the ability to take risks. Our participants showed significant improvement in cognitive T-scores after the dance intervention and Δ post-pre change in cognitive T-scores when DG was compared to CG. Further, we found better participants’ performance in short-term memory assessed by the RAVLT A1 in DG compared to MaG and significant deterioration in CG. A recent meta-analysis summarized that dance interventions benefit specific cognitive domains, such as global cognition, memory, and executive function.92 Ma et al93 provide evidence that regular rhythmic movement, like dance, improves global cognitive function but not executive functions. In practices based on body awareness, the creative process leads to forgotten or new resources, stimulates new associations and releases energy for decision-making and action, thus creating relationships.18 Numerous studies suggest that a long-term dance intervention could be better than repeated PA for inducing neuroplasticity in the ageing human brain, which is related to the multimodal nature of dance.19,94 However, the duration of the intervention and the intensity of the dancing exercise might be the key factor for brain changes and cognitive improvements,19 as documented earlier on PA.10,95 Moreover, dance was shown to be superior to aerobic exercise after 12 weeks in older adults.96 Our results did not show a significant beneficial effect on cognition in more cognitive domains in both intervention groups compared to CG. The explanation could be the test’s low sensitivity for revealing changes in cognitive processes, the ceiling effect in pre-tests, and the possibility that changes in the brain precede the changes in measurable behavior.
Limitations and Future Proposal
Although we recruited the study participants based on the lowest RAPA score, most participants led fairly active lifestyles (social and sports activities), which became apparent from talks during interventions. Moreover, according to the FAQ-CZ score and cognitive and physical measurements, most study participants reported higher education levels and demonstrated good mental and physical condition. Also, the majority of the study participants were females. Therefore, all these might have influenced the study results due to the ceiling effect in the pre-tests. Moreover, a significant (more than 20%) dropout of the participants during the intervention period should also be considered a study limitation. Future studies should focus on follow-up and investigate the motivations behind adherence, as it is well known that neural plasticity in older adults depends on individual behavior,97,98 and can be positively modified by PA.99,100 Also, more extended intervention periods would benefit from observing changes related explicitly to cognitive domains. The ultimate goal should be finding a physical exercise protocol that works best to improve physical and cognitive performance deficits in specific populations of older adults.
Conclusion
Exerkines represent excellent biomarkers in our quest to comprehend the complex relationship between exercise and brain health. Even though our study found no significant changes in serum irisin levels across the groups, changes in anthropometric T-scores (Δ) (ie increased muscle mass and decreased fat mass) were significantly correlated with irisin levels, independent of group effects. We also found a significant increase in brain-derived neurotrophic factor (BDNF) levels in the MaG group, which suggests that BDNF can be upregulated by such somatic-based practice. Our data suggest that dance and martial arts could be promising non-pharmacological programs for the ageing brain, and scientists should further focus on providing evidence of their beneficial effects at the molecular level.
Declarations
The study was approved by the Charles University Faculty of Physical Education and Sport ethics committees (245/2020) and the Charles University Hospital Kralovske Vinohrady (EK-VP/13/0/2020), and all the participants signed an informed consent. All methods were performed following the Declarations of Helsinki.
Data Sharing Statement
The data supporting this study’s findings are available from the corresponding author, MS, upon reasonable request.
Acknowledgments
We appreciate each participant’s contribution and study member participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from Charles University Cooperation, SVV 260 731/ 2023, and by the Grant Agency of the Charles University grant number 268321. The funding agency played no role in the study design, data collection and analysis, the decision to publish, or the preparation of the manuscript.
Disclosure
This manuscript has not been previously submitted or published and is not under consideration in any other peer-reviewed media. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Ahlskog JE. Does vigorous exercise have a neuroprotective effect in Parkinson disease? Neurology. 2011;77(3):288–294. doi:10.1212/WNL.0b013e318225ab66
2. Arida RM, Cavalheiro EA, da Silva AC, Scorza FA. Physical activity and epilepsy: proven and predicted benefits. Sports Med. 2008;38(7):607–615. doi:10.2165/00007256-200838070-00006
3. Buchman AS, Boyle PA, Yu L, Shah RC, Wilson RS, Bennett DA. Total daily physical activity and the risk of AD and cognitive decline in older adults. Neurology. 2012;78(17):1323–1329. doi:10.1212/WNL.0b013e3182535d35
4. Zhang Q, Wu Y, Zhang P, et al. Exercise induces mitochondrial biogenesis after brain ischemia in rats. Neuroscience. 2012;205:10–17. doi:10.1016/j.neuroscience.2011.12.053
5. Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci. 2003;14(2):125–130. doi:10.1111/1467-9280.t01-1-01430
6. Heo J, Noble EE, Call JA. The role of exerkines on brain mitochondria: a mini-review. J Appl Physiol. 2023;134(1):28–35. doi:10.1152/japplphysiol.00565.2022
7. Knaepen K, Goekint M, Heyman EM, Meeusen R. Neuroplasticity - exercise-induced response of peripheral brain-derived neurotrophic factor: a systematic review of experimental studies in human subjects. Sports Med. 2010;40(9):765–801. doi:10.2165/11534530-000000000-00000
8. Bostrom P, Wu J, Jedrychowski MP, et al. A PGC1-alpha-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature. 2012;481(7382):463–468. doi:10.1038/nature10777
9. Dun SL, Lyu RM, Chen YH, Chang JK, Luo JJ, Dun NJ. Irisin-immunoreactivity in neural and non-neural cells of the rodent. Neuroscience. 2013;240:155–162. doi:10.1016/j.neuroscience.2013.02.050
10. Erickson KI, Voss MW, Prakash RS, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A. 2011;108(7):3017–3022. doi:10.1073/pnas.1015950108
11. Wrann CD, White JP, Salogiannnis J, et al. Exercise induces hippocampal BDNF through a PGC-1alpha/FNDC5 pathway. Cell Metab. 2013;18(5):649–659. doi:10.1016/j.cmet.2013.09.008
12. Lopez-Ortiz S, Lista S, Valenzuela PL, et al. Effects of physical activity and exercise interventions on Alzheimer’s disease: an umbrella review of existing meta-analyses. J Neurol. 2023;270(2):711–725. doi:10.1007/s00415-022-11454-8
13. Batson G. Update on proprioception: considerations for dance education. J Dance Med Sci. 2009;13(2):35–41. doi:10.1177/1089313X0901300201
14. Spanos K. Kinesthetic empathy in creative and cultural practices. Theatre Surv. 2014;55(2):264–266. doi:10.1017/S0040557414000131
15. Woodward TW. A review of the effects of martial arts practice on health. WMJ. 2009;108(1):40–43.
16. Brown S, Martinez MJ, Parsons LM. The neural basis of human dance. Cereb Cortex. 2006;16(8):1157–1167. doi:10.1093/cercor/bhj057
17. Sandel SL. Movement therapy with geriatric patients in a convalescent home. Hosp Community Psychiatry. 1978;29(11):738–741. doi:10.1176/ps.29.11.738
18. Fink B, Bläsing B, Ravignani A, Shackelford TK. Evolution and functions of human dance. Evol Hum Behav. 2021;42(4):351–360. doi:10.1016/j.evolhumbehav.2021.01.003
19. Muinos M, Ballesteros S. Does dance counteract age-related cognitive and brain declines in middle-aged and older adults? A systematic review. Neurosci Biobehav Rev. 2021;121:259–276. doi:10.1016/j.neubiorev.2020.11.028
20. Porto FHG, Tusch ES, Fox AM, Alperin BR, Holcomb PJ, Daffner KR. One of the most well-established age-related changes in neural activity disappears after controlling for visual acuity. Neuroimage. 2016;130:115–122. doi:10.1016/j.neuroimage.2016.01.035
21. Solianik R, Mickeviciene D, Zlibinaite L, Cekanauskaite A. Tai chi improves psycho-emotional state, cognition, and motor learning in older adults during the COVID-19 pandemic. Exp Gerontol. 2021;150:111363. doi:10.1016/j.exger.2021.111363
22. Wayne PM, Walsh JN, Taylor-Piliae RE, et al. Effect of tai chi on cognitive performance in older adults: systematic review and meta-analysis. J Am Geriatr Soc. 2014;62(1):25–39. doi:10.1111/jgs.12611
23. Fong Yan A, Nicholson LL, Ward RE, et al. The effectiveness of dance interventions on psychological and cognitive health outcomes compared with other forms of physical activity: a systematic review with meta-analysis. Sports Med. 2024;54(5):1179–1205. doi:10.1007/s40279-023-01990-2
24. Predovan D, Julien A, Esmail A, Bherer L. Effects of dancing on cognition in healthy older adults: a systematic review. J Cogn Enhanc. 2019;3(2):161–167. doi:10.1007/s41465-018-0103-2
25. Tommasini E, Cipriani E, Antonietti A, Galvani C. Correlations between physical activity level, quality of life, and cognitive performance in elderly individuals engaging in multi-year dance activities. J Dance Med Sci. 2022;26(1):34–40. doi:10.12678/1089-313X.031522e
26. Rodziewicz-Flis EA, Kawa M, Kaczor JJ, et al. Changes in selected exerkines concentration post folk-dance training are accompanied by glucose homeostasis and physical performance improvement in older adults. Sci Rep. 2023;13(1):8596. doi:10.1038/s41598-023-35583-w
27. Topolski TD, LoGerfo J, Patrick DL, Williams B, Walwick J, Patrick MB. The rapid assessment of physical activity (RAPA) among older adults. Prev Chronic Dis. 2006;3(4):A118.
28. Galvin JE, Roe CM, Powlishta KK, et al. The AD8: a brief informant interview to detect dementia. Neurology. 2005;65(4):559–564. doi:10.1212/01.wnl.0000172958.95282.2a
29. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
30. Kattenstroth JC, Kalisch T, Holt S, Tegenthoff M, Dinse HR. Six months of dance intervention enhances postural, sensorimotor, and cognitive performance in elderly without affecting cardio-respiratory functions. Front Aging Neurosci. 2013;5:5. doi:10.3389/fnagi.2013.00005
31. WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour: At a Glance. Geneva: World Health Organization; 2020.
32. Lippi G, Salvagno GL, Montagnana M, Lima-Oliveira G, Guidi GC, Favaloro EJ. Quality standards for sample collection in coagulation testing. Semin Thromb Hemost. 2012;38(6):565–575. doi:10.1055/s-0032-1315961
33. Tuck MK, Chan DW, Chia D, et al. Standard operating procedures for serum and plasma collection: early detection research network consensus statement standard operating procedure integration working group. J Proteome Res. 2009;8(1):113–117. doi:10.1021/pr800545q
34. Bean J. Rey Auditory Verbal Learning Test, Rey AVLT. In: Kreutzer JS, DeLuca J, Caplan B editors, Encyclopedia of Clinical Neuropsychology.
35. Bezdicek O, Stepankova H, Motak L, et al. Czech version of rey auditory verbal learning test: normative data. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn. 2014;21(6):693–721. doi:10.1080/13825585.2013.865699
36. Rey A. L’examen psychologique dans les cas d’encéphalopathie traumatique. (Les problems.). Arch Psychol. 1941;28:215–285. French.
37. Thurstone LL. Primary mental abilities. Science. 1948;108(2813):585.
38. Preiss M, Rodriguez M, Kawaciukowa R, Laing H. Neuropsychological Battery of Psychiatric Prague Center: Clinical Assessment of Basic Cognitive Functions. Praha, Czech Republic: Psychiatricke centrum Praha; 2007.
39. Kaufman AS, Lichtenberger EO. Assessing Adolescent and Adult Intelligence. Wiley; 2005.
40. Lezak MD, Howieson DB, Hannay HJ, Loring DW, Fischer JS. Neuropsychological Assessment. Oxford University Press; 2004.
41. Bowie CR, Harvey PD. Administration and interpretation of the trail making test. Nat Protoc. 2006;1(5):2277–2281. doi:10.1038/nprot.2006.390
42. Preiss M, Bartos A, Čermáková R, et al. Neuropsychological Battery of the Psychiatric Prague Center: Clinical Examinations of Major Cognitive Functions. Prague: Psychiatrické centrum; 2012.
43. Reitan RM. Validity of the trail making test as an indicator of organic brain damage. Percept Mot Skills. 1958;8(3):271–276. doi:10.2466/pms.1958.8.3.271
44. Lesher EL, Berryhill JS. Validation of the geriatric depression scale-short form among inpatients. J Clin Psychol. 1994;50(2):256–260. doi:10.1002/1097-4679(199403)50:2<256::aid-jclp2270500218>3.0.co;2-e
45. Pfeffer RI, Kurosaki TT, Harrah CH Jr, Chance JM, Filos S. Measurement of functional activities in older adults in the community. J Gerontol. 1982;37(3):323–329. doi:10.1093/geronj/37.3.323
46. Baumgartner RN, Koehler KM, Gallagher D, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol. 1998;147(8):755–763. doi:10.1093/oxfordjournals.aje.a009520
47. Maggio M, Ceda GP, Ticinesi A, et al. Instrumental and non-instrumental evaluation of 4-meter walking speed in older individuals. PLoS One. 2016;11(4):e0153583. doi:10.1371/journal.pone.0153583
48. Guralnik JM, Ferrucci L, Pieper CF, et al. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol a Biol Sci Med Sci. 2000;55(4):M221–231. doi:10.1093/gerona/55.4.m221
49. Chow LS, Gerszten RE, Taylor JM, et al. Exerkines in health, resilience and disease. Nat Rev Endocrinol. 2022;18(5):273–289. doi:10.1038/s41574-022-00641-2
50. Jodeiri Farshbaf M, Alvina K. Multiple roles in neuroprotection for the exercise derived myokine irisin. Front Aging Neurosci. 2021;13:649929. doi:10.3389/fnagi.2021.649929
51. Lourenco MV, Frozza RL, de Freitas GB, et al. Exercise-linked FNDC5/irisin rescues synaptic plasticity and memory defects in Alzheimer’s models. Nat Med. 2019;25(1):165–175. doi:10.1038/s41591-018-0275-4
52. Jandova T, Buendia-Romero A, Polanska H, et al. Long-term effect of exercise on irisin blood levels-systematic review and meta-analysis. Healthcare. 2021;9(11). doi:10.3390/healthcare9111438
53. Miyamoto-Mikami E, Sato K, Kurihara T, et al. Endurance training-induced increase in circulating irisin levels is associated with reduction of abdominal visceral fat in middle-aged and older adults. PLoS One. 2015;10(3):e0120354. doi:10.1371/journal.pone.0120354
54. Kim HJ, Lee HJ, So B, Son JS, Yoon D, Song W. Effect of aerobic training and resistance training on circulating irisin level and their association with change of body composition in overweight/obese adults: a pilot study. Physiol Res. 2016;65(2):271–279. doi:10.33549/physiolres.932997
55. Norheim F, Langleite TM, Hjorth M, et al. The effects of acute and chronic exercise on PGC-1alpha, irisin and browning of subcutaneous adipose tissue in humans. FEBS J. 2014;281(3):739–749. doi:10.1111/febs.12619
56. Pekkala S, Wiklund PK, Hulmi JJ, et al. Are skeletal muscle FNDC5 gene expression and irisin release regulated by exercise and related to health? J Physiol. 2013;591(21):5393–5400. doi:10.1113/jphysiol.2013.263707
57. Tommasini E, Missaglia S, Vago P, et al. The time course of irisin release after an acute exercise: relevant implications for health and future experimental designs. Eur J Transl Myol. 2024;34(2). doi:10.4081/ejtm.2024.12693
58. Cosio PL, Crespo-Posadas M, Velarde-Sotres A, Pelaez M. Effect of chronic resistance training on circulating irisin: systematic review and meta-analysis of randomized controlled trials. Int J Environ Res Public Health. 2021;18(5):2476. doi:10.3390/ijerph18052476
59. Mohammad Rahimi GR, Hejazi K, Hofmeister M. The effect of exercise interventions on Irisin level: a systematic review and meta-analysis of randomized controlled trials. Excli J. 2022;21:524–539. doi:10.17179/excli2022-4703
60. Motahari Rad M, Bijeh N, Attarzadeh Hosseini SR, Raouf Saeb A. The impact of different modes of exercise training on irisin: a systematic review and meta-analysis research. J Adv Med Biomed Res. 2021;29:125–138. doi:10.30699/jambs.29.134.125
61. Uusi-Rasi K, Sievanen H, Vuori I, et al. Long-term recreational gymnastics, estrogen use, and selected risk factors for osteoporotic fractures. J Bone Miner Res. 1999;14(7):1231–1238. doi:10.1359/jbmr.1999.14.7.1231
62. Nicolini C, Michalski B, Toepp SL, et al. A single bout of high-intensity interval exercise increases corticospinal excitability, brain-derived neurotrophic factor, and uncarboxylated osteocalcin in sedentary, healthy males. Neuroscience. 2020;437:242–255. doi:10.1016/j.neuroscience.2020.03.042
63. Chen X, Gan L. An exercise-induced messenger boosts memory in Alzheimer’s disease. Nat Med. 2019;25(1):20–21. doi:10.1038/s41591-018-0311-4
64. Vints WAJ, Levin O, Fujiyama H, Verbunt J, Masiulis N. Exerkines and long-term synaptic potentiation: mechanisms of exercise-induced neuroplasticity. Front Neuroendocrinol. 2022;66:100993. doi:10.1016/j.yfrne.2022.100993
65. Kujach S, Chroboczek M, Jaworska J, et al. Judo training program improves brain and muscle function and elevates the peripheral BDNF concentration among the elderly. Sci Rep. 2022;12(1):13900. doi:10.1038/s41598-022-17719-6
66. Cho SY, Roh HT. Taekwondo enhances cognitive function as a result of increased neurotrophic growth factors in elderly women. Int J Environ Res Public Health. 2019;16(6):962. doi:10.3390/ijerph16060962
67. Marinus N, Hansen D, Feys P, Meesen R, Timmermans A, Spildooren J. The impact of different types of exercise training on peripheral blood brain-derived neurotrophic factor concentrations in older adults: a meta-analysis. Sports Med. 2019;49(10):1529–1546. doi:10.1007/s40279-019-01148-z
68. Dinoff A, Herrmann N, Swardfager W, et al. The effect of exercise training on resting concentrations of peripheral brain-derived neurotrophic factor (BDNF): a meta-analysis. PLoS One. 2016;11(9):e0163037. doi:10.1371/journal.pone.0163037
69. Pareja-Galeano H, Alis R, Sanchis-Gomar F, et al. Methodological considerations to determine the effect of exercise on brain-derived neurotrophic factor levels. Clin Biochem. 2015;48(3):162–166. doi:10.1016/j.clinbiochem.2014.11.013
70. Molendijk ML, Haffmans JP, Bus BA, et al. Serum BDNF concentrations show strong seasonal variation and correlations with the amount of ambient sunlight. PLoS One. 2012;7(11):e48046. doi:10.1371/journal.pone.0048046
71. Lee P, Linderman JD, Smith S, et al. Irisin and FGF21 are cold-induced endocrine activators of brown fat function in humans. Cell Metab. 2014;19(2):302–309. doi:10.1016/j.cmet.2013.12.017
72. Serra MP, Poddighe L, Boi M, et al. Effect of acute stress on the expression of BDNF, trkB, and PSA-NCAM in the hippocampus of the roman rats: a genetic model of vulnerability/resistance to stress-induced depression. Int J Mol Sci. 2018;19(12):3745. doi:10.3390/ijms19123745
73. Guzman-Garcia A, Hughes JC, James IA, Rochester L. Dancing as a psychosocial intervention in care homes: a systematic review of the literature. Int J Geriatr Psychiatry. 2013;28(9):914–924. doi:10.1002/gps.3913
74. Vankova H, Holmerova I, Machacova K, Volicer L, Veleta P, Celko AM. The effect of dance on depressive symptoms in nursing home residents. J Am Med Dir Assoc. 2014;15(8):582–587. doi:10.1016/j.jamda.2014.04.013
75. Podolski OS, Whitfield T, Schaaf L, et al. The impact of dance movement interventions on psychological health in older adults without dementia: a systematic review and meta-analysis. Brain Sci. 2023;13(7):981. doi:10.3390/brainsci13070981
76. Teixeira-Machado L, Arida RM, de Jesus Mari J. Dance for neuroplasticity: a descriptive systematic review. Neurosci Biobehav Rev. 2019;96:232–240. doi:10.1016/j.neubiorev.2018.12.010
77. Muller P, Duderstadt Y, Lessmann V, Muller NG. Lactate and BDNF: key mediators of exercise induced neuroplasticity? J Clin Med. 2020;9(4):1136. doi:10.3390/jcm9041136
78. Svensson M, Lexell J, Deierborg T. Effects of physical exercise on neuroinflammation, neuroplasticity, neurodegeneration, and behavior: what we can learn from animal models in clinical settings. Neurorehabil Neural Repair. 2015;29(6):577–589. doi:10.1177/1545968314562108
79. Vilela TC, Muller AP, Damiani AP, et al. Strength and aerobic exercises improve spatial memory in aging rats through stimulating distinct neuroplasticity mechanisms. Mol Neurobiol. 2017;54(10):7928–7937. doi:10.1007/s12035-016-0272-x
80. Planella-Farrugia C, Comas F, Sabater-Masdeu M, et al. Circulating irisin and myostatin as markers of muscle strength and physical condition in elderly subjects. Front Physiol. 2019;10:871. doi:10.3389/fphys.2019.00871
81. Colaianni G, Oranger A, Dicarlo M, et al. Irisin serum levels and skeletal muscle assessment in a cohort of Charcot-Marie-tooth patients. Front Endocrinol. 2022;13:886243. doi:10.3389/fendo.2022.886243
82. Baek JY, Jang IY, Jung HW, et al. Serum irisin level is independent of sarcopenia and related muscle parameters in older adults. Exp Gerontol. 2022;162:111744. doi:10.1016/j.exger.2022.111744
83. Gomez-Pinilla F, Hillman C. The influence of exercise on cognitive abilities. Compr Physiol. 2013;3(1):403–428. doi:10.1002/cphy.c110063
84. Xia DY, Huang X, Bi CF, Mao LL, Peng LJ, Qian HR. PGC-1alpha or FNDC5 is involved in modulating the effects of Aβ1−42 oligomers on suppressing the expression of BDNF, a beneficial factor for inhibiting neuronal apoptosis, Aβ deposition and cognitive decline of APP/PS1 Tg mice. Front Aging Neurosci. 2017;9:65. doi:10.3389/fnagi.2017.00065
85. Zoladz JA, Pilc A, Majerczak J, Grandys M, Zapart-Bukowska J, Duda K. Endurance training increases plasma brain-derived neurotrophic factor concentration in young healthy men. J Physiol Pharmacol. 2008;59(7):119–132.
86. Guilherme J, Semenova EA, Borisov OV, et al. The BDNF-increasing allele is associated with increased proportion of fast-twitch muscle fibers, handgrip strength, and power athlete status. J Strength Cond Res. 2022;36(7):1884–1889. doi:10.1519/JSC.0000000000003756
87. Clow C, Jasmin BJ. Brain-derived neurotrophic factor regulates satellite cell differentiation and skeletal muscle regeneration. Mol Biol Cell. 2010;21(13):2182–2190. doi:10.1091/mbc.e10-02-0154
88. Renteria I, Garcia-Suarez PC, Fry AC, et al. The molecular effects of BDNF synthesis on skeletal muscle: a mini-review. Front Physiol. 2022;13:934714. doi:10.3389/fphys.2022.934714
89. Brigola AG, Rossetti ES, Dos Santos BR, et al. Relationship between cognition and frailty in elderly: a systematic review. Dement Neuropsychol. 2015;9(2):110–119. doi:10.1590/1980-57642015DN92000005
90. Pieruccini-Faria F, Lord SR, Toson B, Kemmler W, Schoene D. Mental flexibility influences the association between poor balance and falls in older people - a secondary analysis. Front Aging Neurosci. 2019;11:133. doi:10.3389/fnagi.2019.00133
91. Basso JC, Satyal MK, Rugh R. Dance on the brain: enhancing intra- and inter-brain synchrony. Front Hum Neurosci. 2020;14:584312. doi:10.3389/fnhum.2020.584312
92. Menezes AC, Drumond G, Shigaeff N. Dance therapy and cognitive impairment in older people: a review of clinical data. Dement Neuropsychol. 2022;16(4):373–383. doi:10.1590/1980-5764-DN-2021-0103
93. Ma C, Li M, Li R, Wu C. The effect of rhythmic movement on physical and cognitive functions among cognitively healthy older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2023;104:104837. doi:10.1016/j.archger.2022.104837
94. Rehfeld K, Luders A, Hokelmann A, et al. Dance training is superior to repetitive physical exercise in inducing brain plasticity in the elderly. PLoS One. 2018;13(7):e0196636. doi:10.1371/journal.pone.0196636
95. FGdM C, Gobbi S, Andreatto CAA, Corazza DI, Pedroso RV, Santos-Galduróz RF. Physical exercise modulates peripheral levels of brain-derived neurotrophic factor (BDNF): a systematic review of experimental studies in the elderly. Arch Gerontol Geriatr. 2013;56(1):10–15. doi:10.1016/j.archger.2012.06.003
96. Esmail A, Vrinceanu T, Lussier M, et al. Effects of dance/movement training vs. aerobic exercise training on cognition, physical fitness and quality of life in older adults: a randomized controlled trial. J Bodyw Mov Ther. 2020;24(1):212–220. doi:10.1016/j.jbmt.2019.05.004
97. Brehmer Y, Kalpouzos G, Wenger E, Lovden M. Plasticity of brain and cognition in older adults. Psychol Res. 2014;78(6):790–802. doi:10.1007/s00426-014-0587-z
98. Pascual-Leone A, Amedi A, Fregni F, Merabet LB. The plastic human brain cortex. Annu Rev Neurosci. 2005;28:377–401. doi:10.1146/annurev.neuro.27.070203.144216
99. Toril P, Reales JM, Ballesteros S. Video game training enhances cognition of older adults: a meta-analytic study. Psychol Aging. 2014;29(3):706–716. doi:10.1037/a0037507
100. Vaportzis E, Niechcial MA, Gow AJ. A systematic literature review and meta-analysis of real-world interventions for cognitive ageing in healthy older adults. Ageing Res Rev. 2019;50:110–130. doi:10.1016/j.arr.2019.01.006
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.