")
Back to Journals » Clinical Ophthalmology » Volume 18
The Efficacy and Safety of Dexamethasone Intracanalicular Insert Use in Patients with Chronic Seasonal/Perennial Allergic Conjunctivitis: A Systematic Review and Meta-Analysis
Authors Alsudais AS, Alshehri WM, Alrehaili AM, Albeladi RK, Khoshhal M, Albelowi A , Alzahrani RS, Alnabihi A , Bashrahil B, Alabbasi O
Received 6 May 2024
Accepted for publication 12 August 2024
Published 21 September 2024 Volume 2024:18 Pages 2657—2666
DOI https://doi.org/10.2147/OPTH.S470657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ali S Alsudais,1,2 Waleed Mohammed Alshehri,3 Ahmed M Alrehaili,4 Reyadh Khalid Albeladi,5 Mohammed Khoshhal,4,6 Ahmed Albelowi,4 Raghad Saleh Alzahrani,1,2 Ahmed Alnabihi,1,2 Bader Bashrahil,1,2 Omar Alabbasi3
1College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia; 3Department of Ophthalmology, King Salman Bin Abdulaziz Medical City, Madinah, Saudi Arabia; 4College of Medicine, Taibah University, Madinah, Saudi Arabia; 5College of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 6Ohud Hospital, Madinah, Saudi Arabia
Correspondence: Ahmed Alnabihi, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, 21423, Saudi Arabia, Tel +966569493360, Email [email protected]
Objective: This meta-analysis evaluated the efficacy and safety of DEXTENZA, an intracanalicular dexamethasone insert, for the treatment of seasonal/perennial allergic conjunctivitis.
Methods: Multiple databases, including PubMed, the Cochrane Central Register of Controlled Trials (CENTRAL), ClinicalTrials.gov, the Directory of Open Access Journals, and Scopus, were searched for randomized controlled trials (RCTs) comparing the efficacy of DEXTENZA with a placebo. The primary efficacy endpoint was the change in the conjunctival allergen challenge (CAC) model. The GRADE approach was used to assess the certainty of evidence, and the revised Cochrane risk of bias tool for randomized trials was employed to assess bias.
Results: Four RCTs involving 323 participants met the eligibility criteria, and all had a low risk of bias. A meta-analysis revealed a statistically significant increase in the mean CAC change for conjunctival itching, with low heterogeneity among measurements at 3 minutes (P < 0.00001, I2 = 47%), 5 minutes (P < 0.00001, I2 = 46%), and 7 minutes (P < 0.00001, I2 = 41%). Additionally, the meta-analysis found a statistically significant increase in the mean CAC change for conjunctival redness with low heterogeneity (P < 0.00001, I2 = 15%). The pooled analysis showed no significant difference (P = 0.57, I2 = 0%) between the DEXTENZA and placebo groups in the frequency of adverse events.
Conclusion: DEXTENZA has emerged as a promising and viable treatment option for patients with seasonal/perennial allergic conjunctivitis and is an effective alternative to current therapeutic modalities.
Keywords: conjunctivitis, allergic conjunctivitis, dexamethasone insert, DEXTENZA
Introduction
In recent decades, there has been a gradual increase in the global incidence of allergic diseases, including allergic conjunctivitis.1 Allergic conjunctivitis is an inflammatory disorder affecting the conjunctiva, a thin mucous membrane that covers the sclera and lines the inner surface of the eyelids.2 Allergic conjunctivitis can be classified into two main categories based on the underlying immune mechanisms. Seasonal and perennial allergic conjunctivitis are IgE-mediated, meaning they are triggered by exposure to specific allergens. In contrast, vernal keratoconjunctivitis (VKC) and atopic keratoconjunctivitis (AKC) have a more complex etiology, involving a mixed IgE and non-IgE mediated process, where they can be triggered not just by allergens but also by nonspecific irritants.3 The prevalence of allergic conjunctivitis at the population level was determined through the implementation of the National Health and Nutrition Examination Survey III from 1988 to 1994. This extensive survey aimed to collect comprehensive data on the health status, socioeconomic, and demographic characteristics of individuals. A total of 33,994 participants were interviewed, revealing that approximately 40% of individuals aged 17 years and older had symptoms meeting the criteria for allergic conjunctivitis.4,5 Allergic conjunctivitis has several subtypes, including atopic, vernal, seasonal/perennial, and giant papillary conjunctivitis. These classifications delineate distinct clinical presentations and underlying pathophysiological mechanisms.2 Common clinical manifestations of allergic conjunctivitis include pruritus (itchiness), lacrimation (excessive tearing), photophobia (sensitivity to light), and ocular pain.6
The management of allergic conjunctivitis necessitates a multifaceted approach involving both pharmacological and non-pharmacological interventions. Initial measures focus on the avoidance of environmental irritants to minimize exposure and subsequent allergic reactions. Pharmacological management includes both prophylactic and therapeutic medications, administered via topical ocular drops or systemic routes.7 Prophylactic drugs, such as sodium cromoglycate and nedocromil, function as mast cell stabilizers, exerting their effect by blocking the release of inflammatory mediators and thereby preventing the onset of symptoms.7,8 Symptomatic relief is achieved through the use of decongestants, including astringents (eg, silver nitrate or zinc sulfate), vessel vasoconstrictors (alpha and beta sympathomimetics), or antihistamines (eg, astemizole or cetirizine). These medications work by a reduction in conjunctival congestion, constriction of blood vessels, and inhibition of histamine-mediated allergic responses.7,8 Furthermore, anti-inflammatory drugs such as NSAIDs and corticosteroids play a key role in reducing inflammation and suppressing immune-mediated responses. These agents act by inhibiting the production of pro-inflammatory mediators and modulating the immune response, thereby alleviating symptoms and promoting ocular comfort.7,8
Corticosteroids are effective for allergic reactions by inhibiting the production of inflammatory substances such as prostaglandins and leukotrienes, reducing inflammatory cells, and suppressing mast cell proliferation. These pleiotropic actions make corticosteroids effective in both the early and late stages of the allergic response.9 Consequently, patients who are more prone to experiencing the late-phase inflammatory response, eg, those with moderate to severe symptoms, prolonged or recurrent allergen exposure, or inadequate symptom management with antihistamines and mast cell stabilizers, often receive topical corticosteroid treatment.9,10 It is important to note, however, that prolonged use of corticosteroids may cause significant adverse effects, including increased intraocular pressure and the development of glaucoma, cataracts, and an elevated risk of infection.11 Despite the frequent use of topical therapies for allergic conjunctivitis, there are still several needs unmet by the current treatment options. These inadequacies include inconsistent efficacy, short duration of action, delayed onset of action, and safety concerns associated with side effects, particularly those induced by steroids and preservatives. Consequently, there remains a demand for long-acting therapies that consistently demonstrate efficacy, require lower dosages, and effectively inhibit the late-phase inflammatory response without major adverse effects.11
The introduction of an intracanalicular dexamethasone insert, commercially known as DEXTENZA (dexamethasone ophthalmic insert, 0.4 mg), developed by Ocular Therapeutix, Inc., in Bedford, Massachusetts, USA, has provided a means of harnessing the benefits of corticosteroids while mitigating the risk of severe side effects. The insert encompasses a biodegradable, crosslinked, synthetic, hydrophilic, polyethylene glycol–based hydrogel that has been specifically engineered to serve as a drug delivery system for the controlled release of preservative-free dexamethasone to the ocular surface.12 This hydrogel-based dexamethasone implant eliminates the need for conventional eye drops containing preservatives by replacing them with a sustained-release delivery system. To ensure ease and visual confirmation of insertion, the implant is conjugated with fluorescein. It is inserted into the canaliculus of the eyelid through the lacrimal punctum, where it remains for up to thirty days, gradually releasing 0.4 milligrams of dexamethasone onto the ocular surface.13 If necessary, the insert can be removed, but it is designed to be resorbable, thus obviating the need for a physician to manually extract it. Instead, it is naturally cleared through the nasolacrimal duct.14
The objective of the present study was to conduct a systematic review and meta-analysis of published trials to evaluate the clinical efficacy and safety of utilizing the dexamethasone intracanalicular insert in patients diagnosed with seasonal/perennial allergic conjunctivitis.
Methods
This systematic review and meta-analysis followed the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) to ensure transparency and rigor in reporting. The study was also registered in the PROSPERO registry, with a unique identification number (CRD42023456862); this entry can be referenced for further details.
Search Strategy
A comprehensive and rigorous search strategy was implemented across multiple databases, including the Cochrane Central Register of Controlled Trials (CENTRAL), Midline, Scopus, the Directory of Open Access Journals, and ClinicalTrials.gov. The aim was to identify relevant studies meeting predefined inclusion criteria of randomized controlled trials (RCTs) evaluating the use of DEXTENZA in patients with seasonal/perennial allergic conjunctivitis. The search encompassed the entire lifespans of the databases, from inception to August 2023, and excluded non-English studies and those employing different study designs. The search terms employed were carefully selected, including keywords related to allergic conjunctivitis and intracanalicular dexamethasone insert, along with relevant synonyms and variations (Supplementary file).
Study Selection
The studies and clinical trials identified through the comprehensive search strategy underwent a meticulous selection process, adhering to the predefined inclusion and exclusion criteria. Two independent reviewers screened the titles, abstracts, and full texts of the identified publications to evaluate their eligibility for inclusion in the systematic review and meta-analysis. Any discrepancies between the reviewers were resolved through extensive discussion and consensus, ensuring a comprehensive and unbiased selection of studies. The primary endpoints of this systematic review and meta-analysis were assessments of the change in the mean score of the modified conjunctival allergen challenge (CAC) test at different follow-up intervals. The CAC test measures the ocular allergic response after controlled exposure to a relevant allergen, with outcomes typically including ocular signs and symptoms such as redness, itching, and tearing.15 This objective measure serves as an indicator of the clinical efficacy of DEXTENZA in managing seasonal/perennial allergic conjunctivitis. Secondary endpoints included the safety profile of DEXTENZA, providing valuable insights into the adverse events and potential risks associated with its use.
Data Extraction
Data extraction was performed by two independent reviewers using a standardized data extraction form to ensure consistency and accuracy. The reviewers extracted pertinent information from each included trial, including important aspects such as study characteristics (eg, author, publication year, study design, sample size, and follow-up duration), participant characteristics (eg, demographics, disease severity, and inclusion/exclusion criteria), and outcome measures (specifically, changes in the modified CAC test results at different intervals and adverse events).To maintain consistency in the data extraction process, any discrepancies in extracted data between the reviewers were resolved through thorough discussion and consensus.
Risk of Bias Assessment
The Cochrane Risk of Bias 2 tool (RoB 2) was employed to assess potential bias in the studies included in the analysis.16 The assessment of the risk of bias of each study was conducted independently by two authors, namely, A.S. and R.Z. Any discrepancies in extracted data between the reviewers were resolved through discussion and consensus. To determine the quality of evidence for each outcome, the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) criteria were employed.17,18 The GRADE instrument, which is endorsed by the Cochrane Collaboration, enabled a comprehensive evaluation of the quality of evidence and strength of the recommendations of the studies included in the meta-analysis.17 This systematic evaluation considered various important factors, including research design, consistency, indirectness, heterogeneity, imprecision, publication bias, and other relevant characteristics discussed in the papers included in this systematic review. Subsequently, the quality of evidence was categorized into distinct levels—high, moderate, low, or very low—based on an overall assessment conducted in accordance with the GRADE framework.17,18
Meta-Analysis
Data analysis was performed using Review Manager (RevMan), version 5.3 (Cochrane Collaboration). The meta-analysis was performed using a random-effects model. A 95% confidence level and P < 0.05 were selected to indicate statistical significance. Statistical heterogeneity was assessed using I2. We used mean change in ocular itching and conjunctival redness in the CAC score as continuous variables, and the standardized mean difference (SMD) was used as the effect measure. Dichotomous outcomes (adverse events) were represented as risk ratios (RRs) and pooled using inverse variance weighting. Subgroup analysis was conducted by evaluating the CAC scores at different time points (3, 5, 7, 15, and 20 minutes post-CAC).
Results
Following an extensive search of the aforementioned databases, a total of 1073 reports were initially retrieved. Among them, 1066 reports were deemed ineligible and subsequently excluded due to a lack of conformity with the predetermined eligibility criteria. Moreover, three additional studies were excluded from the analysis due to inaccessibility or different study designs that did not align with the specific research objectives. Eventually, a rigorous selection process led to the inclusion of four reports derived from four RCTs in the final analysis (Figure 1).19–22
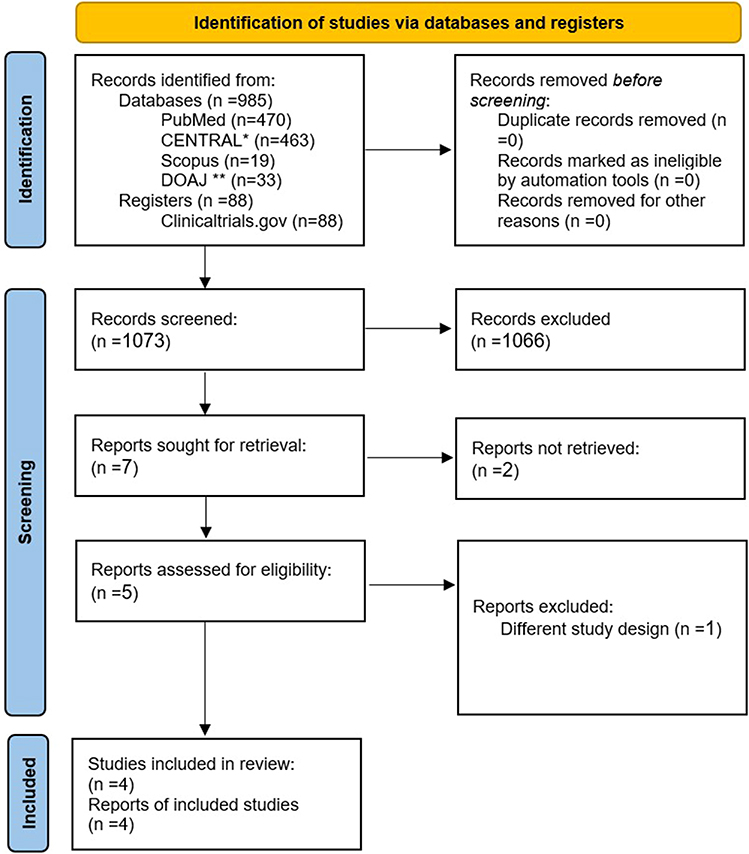 |
Figure 1 PRISMA flowchart. *Cochrane Central Register of Controlled Trials **Directory of Open Access Journals. |
Trial Characteristics
This meta-analysis comprised four clinical trials,19–22 encompassing a collective sample size of 323 patients. Among these participants, 162 were randomly assigned to a DEXTENZA group, whereas 161 were assigned to a placebo vehicle insertion group. The mean duration of participant follow-up in these studies was approximately 30 days. The range of follow-up, from initial intracanalicular insert placement to final study completion, was approximately 1 to 2 months. Notably, the mean age of the participants across all trials was 41.8 years, with an age range spanning from 18 to 71 years. Of the 323 patients in the aggregated trials, 168 (52%) were female and 155 (48%) were male (Supplementary Table 1).
Risk of Bias Assessment
Two independent reviewers (A.S. and R.Z). utilized RoB 214 to individually evaluate the risk of bias of the eligible RCTs. Subsequently, their assessments were combined to provide a comprehensive evaluation. Remarkably, all four trials included in this study demonstrated a low risk of bias, as illustrated in Figure 2 and Supplementary Figure 1.
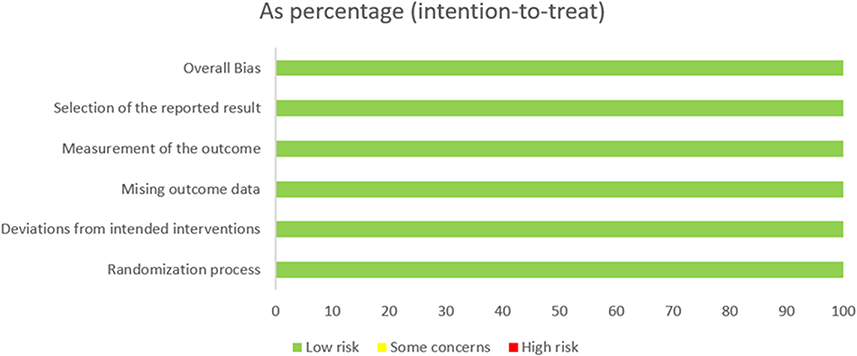 |
Figure 2 Risk of bias graph. |
Efficacy
Ocular Itching in the Conjunctival Allergen Challenge (CAC) Model
The four studies19–22 included in the analysis used ocular itching as the primary endpoint, with examinations 3, 5, and 7 minutes post-CAC. The meta-analysis demonstrated a statistically significant increase in the mean change in CAC scores for conjunctival itching at each time point. The effect sizes, represented by the SMD, were measured at 3 minutes (SMD −0.74, 95% CI −1.05 to −0.44, P < 0.00001, I2 = 47%), 5 minutes (SMD −0.80, 95% CI −1.09 to −0.51, P < 0.00001, I2 = 46%), and 7 minutes (SMD −0.85, 95% CI −1.13 to −0.57, P < 0.00001, I2 = 41%). These findings indicate a significant improvement in conjunctival itching compared to the placebo across all examination durations. Moreover, a sensitivity analysis was performed to assess the impact of individual studies on heterogeneity. The analysis revealed that the significant improvement in conjunctival itching with DEXTENZA resulted in the omission of heterogeneity (I2 = 0%). This indicates that the observed heterogeneity in the initial analysis can be attributed to specific studies (Figure 3 and Supplementary Figure 2). The quality of evidence for this outcome was assessed using the GRADE framework and yielded high certainty of evidence (Table 1).
 |
Table 1 Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) Evidence Profile |
 |
Figure 3 Forest plot of ocular itching in the conjunctival allergen challenge (CAC) model. Abbreviations: CI, confidence interval; SD, standard deviation. |
Conjunctival Redness in the Conjunctival Allergen Challenge (CAC) Model
Two studies19,21 representing 132 subjects included conjunctival redness as their primary endpoint, with examinations 7, 15, and 20 minutes post-CAC. The meta-analysis of these studies revealed a statistically significant increase in the mean change in conjunctival redness at each time point (7, 15, and 20 minutes). The effect size, as measured by the SMD, was −0.44 (95% CI −0.60 to −0.29, P < 0.00001, I2 = 15%), indicating an overall reduction in conjunctival redness with the intervention. Furthermore, a subgroup analysis revealed significant reductions in conjunctival redness at each respective endpoint: 7 minutes (SMD −0.38, 95% CI −0.62 to −0.13, P < 0.003, I2 = 0%), 15 minutes (SMD −0.48, 95% CI −0.90 to −0.06, P < 0.003, I2 = 64%), and 20 minutes (SMD −0.49, 95% CI −0.83 to −0.14, P < 0.005, I2 = 47%). These findings further support the effectiveness of the intervention in reducing conjunctival redness at different time intervals (Figure 4). The quality of evidence for this outcome was assessed using the GRADE framework and yielded high certainty of evidence (Table 1).
 |
Figure 4 Forest plot of conjunctival redness in the conjunctival allergen challenge (CAC) model. Abbreviations: CI, confidence interval; SD, standard deviation. |
Safety Profile
Adverse Events
Four studies19–22 were included in the analysis to investigate the adverse events associated with the insertion of DEXTENZA in patients with seasonal/perennial allergic conjunctivitis. The pooled analysis of these studies revealed no statistically significant difference in the frequency of adverse events between the DEXTENZA and placebo groups (RR = 0.88, 95% CI 0.55–1.39, P = 0.57, I2 = 0%). This finding suggests that DEXTENZA has a favorable safety profile and can be used safely in this patient population (Supplementary Figure 3). The quality of evidence for this outcome was assessed using the GRADE framework and yielded high certainty of evidence (Table 1).
Discussion
DEXTENZA is an intracanalicular insert containing the corticosteroid dexamethasone and has been specifically formulated to provide a sustained release of 0.4 mg of dexamethasone to the ocular surface. In recent studies, the use of DEXTENZA has been investigated in patients with seasonal/perennial allergic conjunctivitis aiming to alleviate the distressing symptoms of ocular itching and redness associated with this condition.19–22 However, to the best of our knowledge, no systematic review and meta-analysis has comprehensively evaluated the safety and efficacy of this novel drug delivery system in patients with seasonal/perennial allergic conjunctivitis. To address this research gap, we conducted a rigorous meta-analysis incorporating four RCTs involving a total of 323 patients with chronic seasonal/perennial allergic conjunctivitis.19–22 The pooled results from these trials consistently demonstrated statistically significant improvements in conjunctival itching and redness when using DEXTENZA compared to a placebo across all designated examination durations. Furthermore, the pooled analysis of the included trials revealed no statistically significant difference in the frequency of adverse events between the DEXTENZA and placebo groups, indicating a favorable safety profile of DEXTENZA when used in this patient population. Notably, DEXTENZA was exclusively utilized in patients diagnosed with seasonal/perennial allergic conjunctivitis who exhibited induced symptoms and signs of conjunctivitis through the modified CAC. Subsequent to the induction of such symptoms, DEXTENZA was inserted to systematically assess its efficacy and safety.19–22
The use of intracanalicular inserts, such as DEXTENZA, confers several advantages over traditional topical eye drops. Primarily, these inserts offer the benefit of sustained drug release, delivering a consistent dosage of 0.4 mg of dexamethasone. As a result, a continuous therapeutic effect is achieved, thereby reducing the need for frequent administration. This feature has the potential to enhance patient compliance23–26 and provide added convenience by mitigating the challenges associated with suboptimal administration techniques27,28 and the accidental injury29 commonly associated with conventional corticosteroid eye drops. Additionally, intracanalicular inserts facilitate direct delivery of the medication to the ocular surface. This mode of administration bypasses potential barriers such as tear dilution and systemic absorption, which are commonly encountered with traditional eye drops. By precisely targeting the ocular surface, the inserts enhance the efficacy of the medication while concurrently reducing the likelihood of systemic side effects.23
Our meta-analysis yielded compelling findings regarding the impact of DEXTENZA insertion on ocular itching and ocular redness, with a statistically significant change observed in the mean CAC value. The evidence supporting this finding is of high certainty, and a strong association was established (P < 0.00001) for both ocular itching and redness. Notably, to the best of our knowledge, our study is the first meta-analysis to investigate the use of DEXTENZA in patients with seasonal/perennial allergic conjunctivitis; no previous studies have been conducted to assess the strength of its effects in this specific population. Nevertheless, our results align with previous investigations that have explored the efficacy and safety of DEXTENZA in treating pain and inflammation following cataract surgery.14,30,31 These previous studies14,30,31 consistently reported positive outcomes, highlighting the effectiveness and tolerability of DEXTENZA in mitigating post-surgical pain and inflammation.
Our comprehensive analysis yielded results indicating no statistically significant difference in the frequency of adverse events between the DEXTENZA and placebo groups, thereby suggesting a favorable safety profile for DEXTENZA in patients diagnosed with seasonal/perennial allergic conjunctivitis. The evidence supporting this finding is of high certainty, reinforcing the reliability of our conclusions. These findings align with previous investigations that have consistently demonstrated a favorable safety profile of DEXTENZA across various conditions].14,23,30,31 Furthermore, a recent study outlined additional advantages of DEXTENZA, including improved patient satisfaction, enhanced convenience, and increased comfort compared to traditional corticosteroid eye drops.32 Moreover, the absence of preservatives, such as benzalkonium chloride (BAK) is an important advantage of DEXTENZA, as preservatives in topical ophthalmic medications can negatively impact ocular tissues.24 These findings collectively highlight the potential of DEXTENZA as a safe and promising treatment option for patients with seasonal/perennial allergic conjunctivitis.
It is crucial to note some limitations of our study. First, the number of included studies was relatively small, which may limit the generalizability of our findings. Second, the duration of the follow-up period varied among the included studies, and longer-term safety and efficacy data were not available. Future studies with longer follow-up periods are needed to assess the sustained effects and long-term safety of DEXTENZA. Further investigations, including larger-scale trials and long-term follow-up studies, are warranted to corroborate these findings and provide a more comprehensive understanding of the efficacy and safety of DEXTENZA use for the management of ocular conditions.
Conclusion
In conclusion, this systematic review and meta-analysis provides compelling evidence supporting the efficacy and safety of DEXTENZA as a potential therapeutic treatment for seasonal/perennial allergic conjunctivitis. The analysis of high-quality RCTs consistently demonstrated a significant and clinically meaningful improvement in conjunctival itching and redness. Importantly, the safety profile of DEXTENZA was favorable, with no observed correlation between DEXTENZA use and serious adverse events or mortality. The frequency of adverse events did not significantly differ between the DEXTENZA and placebo groups, suggesting good tolerability. The inclusion of high-quality RCTs strengthened the reliability and validity of these results. The high certainty of evidence supporting our findings further strengthened the validity of our conclusions. Further research, including long-term studies and comparative effectiveness trials, is warranted to evaluate the long-term efficacy, safety, and potential benefits of DEXTENZA for specific subtypes of allergic conjunctivitis and in different patient populations. Overall, DEXTENZA offers a viable solution to the unmet needs in the management of allergic conjunctivitis and has the potential to improve patient outcomes and quality of life.
Data Sharing Statement
The datasets utilized and/or analyzed in the current study can be obtained from the corresponding author upon submitting a reasonable request.
Funding
There is no funding to report.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Barbee RA, Kaltenborn W, Lebowitz MD, Burrows B. Longitudinal changes in allergen skin test reactivity in a community population sample. J Allergy Clin Immunol. 1987;79(1):16–24. doi:10.1016/S0091-6749(87)80010-6
2. Patel N, Venkateswaran N, Wang Z, Galor A. Ocular involvement in atopic disease: a review. Current Opinion in Ophthal. 2018;29(6):576–581. doi:10.1097/ICU.0000000000000532
3. Shaker M, Salcone E. An update on ocular allergy. Curr Opin Allergy Clin Immunol. 16(5):505–510. doi:10.1097/ACI.0000000000000299
4. Miyazaki D, Fukagawa K, Okamoto S, et al. Epidemiological aspects of allergic conjunctivitis. Allergology Int. 2020;69(4):487–495. doi:10.1016/j.alit.2020.06.004
5. Singh K, Axelrod S, Bielory L. The epidemiology of ocular and nasal allergy in the United States, 1988-1994. J Allergy Clin Immunol. 2010;126(4):778–783.e6. doi:10.1016/j.jaci.2010.06.050
6. Palmares J, Delgado L, Cidade M, Quadrado MJ, Filipe HP. Allergic conjunctivitis: a national cross-sectional study of clinical characteristics and quality of life. European j Ophthal. 2010;20(2):257–264. doi:10.1177/112067211002000201
7. Ciprandi G, Buscaglia S, Cerqueti PM, Canonica GW. Drug treatment of allergic conjunctivitis. A review of the evidence. Drugs. 1992;43(2):154–176. doi:10.2165/00003495-199243020-00003
8. Mishra P, Tamboli G, Jwala V, K Mitra, J A. Recent patents and emerging therapeutics in the treatment of allergic conjunctivitis. Recent Pat Inflamm All Drug Disco. 5(1):26–36. doi:10.2174/187221311794474883
9. Bielory L, Meltzer EO, Nichols KK, Melton R, Thomas RK, Bartlett JD. An algorithm for the management of allergic conjunctivitis. Allerg asthma procet]. 2013;34(5):408–420. doi:10.2500/aap.2013.34.3695
10. Varu DM, Rhee MK, Akpek EK, et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019;126(1):PP94–169. doi:10.1016/j.ophtha.2018.10.020
11. Gomes P, Slocum C, Smith LM, Abelson MB. Challenges faced in clinical trials for chronic allergic conjunctivitis. Expert Rev Ophthalmol. 2015;10(5):509–518. doi:10.1586/17469899.2015.1081563
12. Sawhney AS, Bassett M, Blizzard C Drug delivery through hydrogel plugs - Google Patents.
13. Dextenza, Ocular Inflammation Treatment | Ocular Therapeutix. Available from: https://www.ocutx.com/products/dextenza-ocular-inflammation-pain-and-itching/.
14. Lee A, Blair HA. Dexamethasone Intracanalicular Insert: a Review in Treating Post-Surgical Ocular Pain and Inflammation. Drugs. 2020;80(11):1101–1108. doi:10.1007/s40265-020-01344-6
15. Abelson MB, Loeffler O. Conjunctival allergen challenge: models in the investigation of ocular allergy. Current All Asthma Rep. 2003;3(4):363–368. doi:10.1007/s11882-003-0100-z
16. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ.
17. Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–406. doi:10.1016/j.jclinepi.2010.07.015
18. Chapter 14: completing ‘Summary of findings’ tables and grading the certainty of the evidence | Cochrane Training [Internet]. Available from: https://training.cochrane.org/handbook/current/chapter-14.
19. Torkildsen G, Abelson MB, Gomes PJ, McLaurin E, Potts SL, Vehicle-Controlled MFS. Phase 2 Clinical Trial of a Sustained-Release Dexamethasone Intracanalicular Insert in a Chronic Allergen Challenge Model. J Ocular Pharm Therapeu. 2017;33(2):79–90. doi:10.1089/jop.2016.0154
20. Study Details | OTX-15-002: a Phase 3 Study Evaluating the Safety and Efficacy of OTX-DP for the Treatment of Chronic Allergic Conjunctivitis | clinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT02988882.
21. McLaurin EB, Evans D, Repke CS, et al. Phase 3 Randomized Study of Efficacy and Safety of a Dexamethasone Intracanalicular Insert in Patients With Allergic Conjunctivitis. Am J Ophthalmol. 2021;229:288–300. doi:10.1016/j.ajo.2021.03.017
22. A Study Evaluating the Safety and Efficacy of OTX-DP for the Treatment of Allergic Conjunctivitis. Available from: https://ctv.veeva.com/study/a-study-evaluating-The-safety-and-efficacy-of-otx-dp-for-The-treatment-of-allergic-conjunctivitis.
23. Blizzard C, McLaurin EB, Driscoll A, et al. Plasma Pharmacokinetic Parameters of Dexamethasone Following Administration of a Dexamethasone Intracanalicular Insert in Healthy Adults. Clinical Ophthal. 2021;15:2055–2061. doi:10.2147/OPTH.S307194
24. Brooks CC, Jabbehdari S, Gupta PK. Dexamethasone 0.4mg Sustained-Release Intracanalicular Insert in the Management of Ocular Inflammation and Pain Following Ophthalmic Surgery: design, Development and Place in Therapy. Clin Ophthalmol. 2020;14:89–94. doi:10.2147/OPTH.S238756
25. Robin A, Grover D. Compliance and adherence in glaucoma management. Indian J Ophthalmology. 2011;59(Suppl1):S93. doi:10.4103/0301-4738.73693
26. Olthoff CMG, Schouten JSAG, van de Borne BW, Webers CAB. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension an evidence-based review. Ophthalmology. 2005;112(6):953–961.e7. doi:10.1016/j.ophtha.2004.12.035
27. Gomes BF, Paredes AF, Madeira N, Moraes HV, Santhiago MR. Assessment of eye drop instillation technique in glaucoma patients. Arquivos brasileiros de oftalmologia. 2017;80(4):238–241. doi:10.5935/0004-2749.20170058
28. Gupta R, Patil B, Shah BM, Bali SJ, Mishra SK, Dada T. Evaluating eye drop instillation technique in glaucoma patients. J Glaucoma. 2012;21(3):189–192. doi:10.1097/IJG.0b013e31820bd2e1
29. Solomon A, Chowers I, Raiskup F, Siganos CS, Frucht-Pery J. Inadvertent conjunctival trauma related to contact with drug container tips: a masquerade syndrome. Ophthalmology. 110(4):796–800. doi:10.1016/S0161-6420(02)01967-X
30. Tyson SL, Bafna S, Gira JP, et al. Multicenter randomized phase 3 study of a sustained-release intracanalicular dexamethasone insert for treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 45(2):204–212. doi:10.1016/j.jcrs.2018.09.023
31. Walters T, Bafna S, Vold S, et al. Efficacy and Safety of Sustained Release Dexamethasone for the Treatment of Ocular Pain and Inflammation after Cataract Surgery: results from Two Phase 3 Studies. J Clin Exp Ophthalmol. 2016;07(04). doi:10.4172/2155-9570.1000572
32. Gira JP, Sampson R, Silverstein SM, Walters TR, Metzinger JL, Talamo JH. Evaluating the patient experience after implantation of a 0.4 mg sustained release dexamethasone intracanalicular insert (DextenzaTM): results of a qualitative survey</sup>. Patient Prefer Adhe. 2017;11:487–494. doi:10.2147/PPA.S126283
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.