")
Back to Journals » Journal of Pain Research » Volume 17
The Efficacy of Liposomal Bupivacaine in Thoracic Surgery: A Systematic Review and Meta-Analysis
Authors Gong R , Tan G, Huang Y
Received 23 August 2024
Accepted for publication 21 November 2024
Published 28 November 2024 Volume 2024:17 Pages 4039—4051
DOI https://doi.org/10.2147/JPR.S492117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Ruisong Gong, Gang Tan, Yuguang Huang
Department of Anesthesiology, Peking Union Medical College Hospital, Beijing, 100730, People’s Republic of China
Correspondence: Gang Tan, Department of Anesthesiology, Peking Union Medical College Hospital, Beijing, People’s Republic of China, Email [email protected]
Purpose: Patients undergoing thoracic surgery suffer from severe postoperative pain, and a series of complications will occur if there is no effective analgesic treatment. Liposomal bupivacaine (LB) is a novel multivesicular formulation with up to 72 hours of analgesia, which can be used in thoracic surgery. This meta-analysis aimed to evaluate the efficacy of LB in improving recovery in patients undergoing thoracic surgery compared with non-liposomal local anesthetics.
Patients and Methods: A literature search was conducted using PubMed, Cochrane Library, Embase, and Web of science, and to identify all observational or retrospective studies and randomized controlled trials (RCTs) from inception to December 2023. The primary outcome was the in-hospital postsurgical opioid consumption in morphine milligram equivalents (MMEs). Secondary outcomes included 24-hour postoperative MMEs, postoperative pain score in the first 24 and 48 hours, hospital length of stay (LOS), time to first ambulation, readmission, and perioperative complications. RevMan 5.3 was used for the data analysis.
Results: A total of 10 studies were included in the analysis, of which eight were observational or retrospective analyses and two were RCTs. There were no significant differences in the postoperative MMEs, pain score, LOS, time to first ambulation, readmission, and perioperative complications.
Conclusion: According to this meta-analysis, LB was found to be not superior to non-liposomal local anesthetics for analgesic and functional outcomes in thoracic surgery.
Keywords: liposomal bupivacaine, thoracic surgery, intercostal nerve block, analgesic, meta-analysis
Introduction
Thoracic surgery is widely acknowledged as one of the most painful surgical procedures.1 Postoperative pain management stands as a crucial aspect in the recovery of patients undergoing thoracic surgery, as it can significantly impact their outcomes and lead to serious complications,2 including atelectasis, ventilation disorders, respiratory distress, and chronic pain.3 Therefore, early and effective pain management is an important element of the Enhanced Recovery After Surgery (ERAS) program during the perioperative period.4
The postoperative analgesic strategy encompasses various approaches such as patient-controlled analgesia with potent opioids, administration of nonsteroidal anti-inflammatory drugs and cyclooxygenase-2 inhibitors, continuous paravertebral block, intercostal nerve block (INB), thoracic epidural analgesia as well as infusion of local anesthetics into the wound.5 However, prolonged postoperative opioid use may have a detrimental effect on patient prognosis.6 INB with local anesthetic allows faster recovery and less opioid use, which is effective and safe.7
Commonly used local anesthetics in clinical practice include lidocaine, ropivacaine, and bupivacaine. The duration of effectiveness of lidocaine is 1 to 2 hours, that of ropivacaine is no more than 6 hours, and that of bupivacaine is 2 to 4 hours.8,9 However, their main limitation lies in the fact that the duration of analgesia provided by a single administration often falls short of the duration of surgical pain.10 Compared to standard bupivacaine, liposomal bupivacaine (LB) has a slower release rate and prolonged analgesia for up to 72 hours.11 LB was approved by the US Food and Drug Administration for postsurgical analgesia in 2011,12 and it has been recognized as a potentially effective alternative for relieving postoperative pain and reducing opioid use. Nevertheless, the actual effectiveness of LB in thoracic surgery is controversial in many studies.13 For example, both Scott’s14 and Kian’s15 studies showed that the application of LB decreased the dose of opiate consumption among patients undergoing thoracic surgery. And yet the studies of Benny16 and Sowmyanarayanan17 revealed that LB demonstrated no significant superiority in reducing opioid dosages in patients undergoing such surgeries. The researches were of different types and thus differed in quality and persuasiveness. The objective of our research is to ascertain whether LB provides any advantages over non-liposomal local anesthetics for INB in thoracic surgery.
Materials and Methods
Study Design
This systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) protocols.18 The study was registered on PROSPERO with registration number CRD42024485383. The literature selection was guided by the following inclusion criteria:
Participants: Adult patients undergoing thoracic surgery (thoracoscopy).
Intervention: Patients received LB via INB.
Comparator: Patients received non-liposomal local anesthetics via INB.
Outcomes: The primary outcome was the in-hospital postsurgical opioid consumption measured in morphine milligram equivalents (MMEs). Secondary outcomes included 24-hour postoperative MMEs, postoperative pain score during the first 24 and 48 hours, hospital length of stay (LOS), time to first ambulation, readmission, and perioperative complications.
Type of studies: The published observational or retrospective studies and randomized controlled trials (RCTs).
Exclusion criteria: Studies that did not report relevant outcomes as described above, studies lacking extractable valid data, and studies published in languages other than English.
Data Sources and Search Strategies
The literature search was based on the PubMed and Cochrane Library databases from their inception dates to Dec 2023. The search utilized keywords such as liposomal bupivacaine, thoracic surgery, and their synonyms, including bupivacaine liposome, thoracoscopic surgery, lobectomy, lung resection, and thoracoscopy.
Articles Selection and Data Extraction
Two independent researchers reviewed each article to select potentially relevant publications for inclusion and eliminate all irrelevant studies. Any discrepancies were resolved through discussion and, if necessary, adjudicated by a third researcher. Moreover, studies were evaluated for eligibility and quality. If there are issues such as the inability to extract meaningful data, major problems with the research design, a high level of confounding factors, and unclear important information, we will exclude it as a low-quality study. A standardized form was used to extract data, including the author, publication year, country, study type, sample size in each group, interventions, as well as the outcomes, etc. The data in the form was double-checked by researchers to avoid transcription errors. Authors were contacted via Email to request supplementary information if necessary data were not available in the article.
Assessment of the Bias
Two researchers independently assessed the quality of studies using Cochrane’s risk-of-bias tool for randomized trials (RoB 2) and the Risk Of Bias in Non-randomized Studies of Interventions (ROBINS-I).19,20 For randomized trials, assessment criteria included random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Non-randomized studies were evaluated based on confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, selection of the reported result, and overall bias. Randomized trials were categorized as having a “low”, “unclear”, or “high risk” of bias for each criterion. Non-randomized studies were classified as having “low”, “moderate”, “serious”, or “critical” risk of bias in each ROBINS-I domain. Consensus on bias assessment was reached through discussion between the two researchers. In cases where consensus could not be achieved, the label ‘unclear risk of bias’ was assigned.
Statistical Analysis
Statistical computations were performed using Review Manager 5.3 (RevMan 5.3). Mean difference (MD) with 95% confidence intervals (CIs) was used for continuous data, and odds ratio (OR) with 95% CIs was used for dichotomous outcomes. If data were reported as a median or range, formulas were used to calculate the mean and standard deviation (SD).21,22 The application of the random-effects model in a meta-analysis would be preferred when the number of primary studies and the sample sizes in the primary studies are reasonably large, while the fixed-effects model could be favored for circumstances with a smaller number of studies and uniformly small sample sizes of primary studies.23 So outcomes in this meta-analysis were analyzed by the random-effects model. Chi-squared test and I2 test were performed to judge heterogeneity among the studies. An I2 value less than 40% indicates low heterogeneity, 30% to 60% suggests moderate heterogeneity, 50% to 90% represents possible substantial heterogeneity, and 75% to 100% is considered high heterogeneity. The stability of the outcome was assessed through a sensitivity analysis, which involved progressively excluding low-quality studies. A P value of less than 0.05 was considered statistically significant.
Results
Study Selection and Characteristics
The literature search strategy yielded 260 articles, which were subsequently screened for duplicates and article type resulting in the selection of 67 articles based on title and abstract. After an initial evaluation, 25 articles underwent full-text review, with a final assessment of eligibility conducted on 13 articles. One article failed to extract valid data, the research participants of one article did not comply with the inclusion criteria, and the surgical types of one article were inconsistent. Eventually, ten articles were included into this study.14–17,24–29 The flow diagram is presented in Figure 1.
 |
Figure 1 Search strategy flow diagram. |
These ten studies, involving a total of 1086 patients, were eligible for inclusion in this study. All articles were from the United States and were published between 2017 and 2022. Sample sizes ranged from 47 to 256 patients. Among the ten studies, eight were observational or retrospective in design14,15,24–29 while two were prospective RCTs.16,17 Further details are reported in Table 1.
 |
Table 1 Studies Characteristics |
Risk of Bias in Studies
The risk of bias assessment is presented in Figure 2, and the risk of bias summary is shown in Figure 3. Overall, most studies had a low risk of bias. Two RCTs16,17 were evaluated using RoB 2, with the domain showing the lowest risk of bias being “random sequence generation”, “blinding of participants and personnel”, “incomplete outcome data”, and “selective reporting”, while the domain with the highest risk of bias was “allocation concealment”. Additionally, eight non-RCTs14,15,24–29 were evaluated using ROBINS-I. The domains with the lowest risk of bias were “classification of interventions”, “deviations from intended interventions”, and “measurement of outcomes”, whereas the domain with the highest risk was “selection of participants”.
 |
Figure 2 Risk of bias graph: (A) the risk of bias for RCTs, (B) the risk of bias for non-RCTs. |
 |
Figure 3 Risk of bias summary: (A) the risk of bias summary for RCTs, (B) the risk of bias summary for non-RCTs. |
Postoperative Morphine Dose
As depicted in Figure 4A, the in-hospital postsurgical opioid consumption in MMEs was analyzed in four studies,14–17 involving a total of 438 patients. Two of them were non-RCTs14,15 and two were RCTs.16,17 The results indicated no differences between the LB group and control group (MD −6.36 mg; 95% CI, −23.33–10.60; P = 0.46; I2 = 65%). Subgroup analyses showed no statistically significant differences between LB and control groups in both non-RCTs (MD −34.30 mg; 95% CI, −103.52–34.91; P = 0.33; I2 = 86%) and RCTs (MD 2.87 mg; 95% CI, −10.38–16.12; P = 0.67; I2 = 0%). Furthermore, two non-RCTs24,25 showed that LB might not affect the 24-hour postoperative MMEs between the two groups (MD −2.69 mg; 95% CI, −11.30–5.93; P = 0.54; I2 = 0%) (Figure 4B).
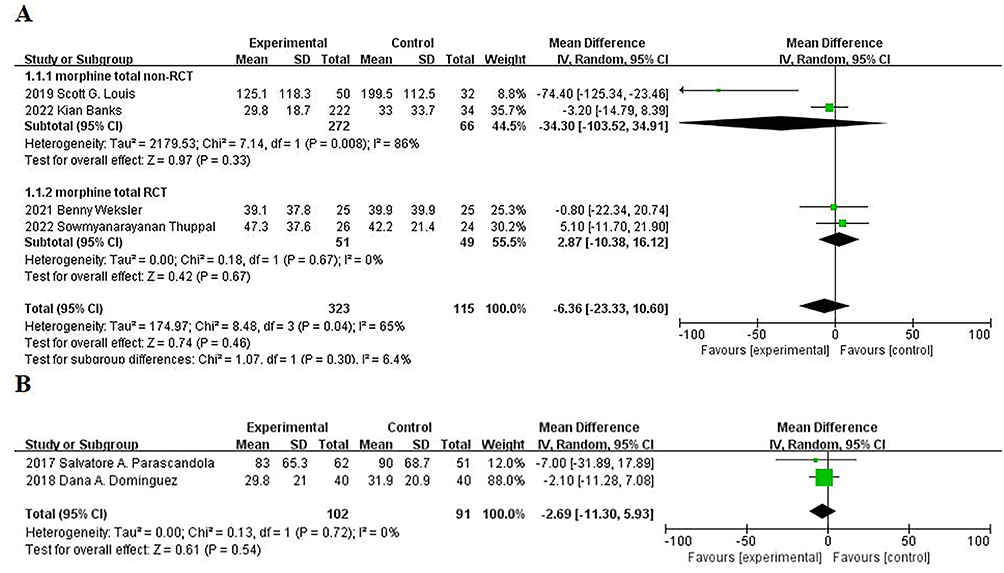 |
Figure 4 Forrest plots of postoperative morphine dose: (A) total in-hospital postsurgical opioid consumption in morphine milligram equivalents (MMEs), (B) 24-hour postoperative MMEs. Abbreviation: CI, confidence interval. |
Postoperative Pain Scores
Two non-RCTs15,25 and two RCTs16,17 compared the 24-hour postoperative pain score between the LB group and control group. The results showed no significant differences in non-RCTs (MD 0.68; 95% CI, −0.11–1.46; P = 0.09; I2 = 69%), RCTs (MD −0.31; 95% CI, −1.16–0.54; P = 0.48; I2 = 0%), or overall analysis (MD 0.32; 95% CI, −0.35–0.99; P = 0.36; I2 = 60%) (Figure 5A). Besides, two RCTs16,17 recorded the 48-hour postoperative pain score for the LB and control groups, showing no differences between the two groups (MD −0.02; 95% CI, −0.75–0.70; P = 0.95; I2 = 0%) (Figure 5B).
 |
Figure 5 Forrest plots of postoperative pain scores: (A) 24-hour postoperative pain score, (B) 48-hour postoperative pain score. Abbreviation: CI, confidence interval. |
Length of Stay (LOS)
Figure 6 shows the results of LOS for the two groups. Five of the included non-RCTs14,15,25,27,28 and two RCTs16,17 reported this endpoint. No differences were found between the two groups (MD −0.32d; 95% CI, −0.90–0.25; P = 0.27; I2 = 82%). This result was consistent with the subgroup analyses of RCTs16,17 (MD 0.39d; 95% CI, −0.14–0.91; P = 0.15; I2 = 0%), yet discrepant from the non-RCT ones14,15,25,27,28 (MD −0.62d; 95% CI, −1.17–0.07; P = 0.03; I2 = 75%).
 |
Figure 6 Forrest plots of length of stay (LOS). Abbreviation: CI, confidence interval. |
Time to First Ambulation
Data from two studies15,17 showed no statistically differences between the LB group and control group in terms of time to first ambulation (MD −0.62h; 95% CI, −5.41–4.17; P = 0.80; I2 = 27%) (Figure 7).
 |
Figure 7 Forrest plots of time to first ambulation. Abbreviation: CI, confidence interval. |
Readmission
Readmission data are presented in Figure 8. Three studies15,25,29 involving 588 patients found no significant differences between the two groups (OR 1.49; 95% CI, 0.78–2.84; P =0.23; I2 = 0%).
 |
Figure 8 Forrest plots of readmission. Abbreviation: CI, confidence interval. |
Perioperative Complications
Similarly, no differences were detected in six studies16,17,24,26,27,29 for perioperative complications, both in the overall analysis (OR 0.86; 95% CI, 0.54–1.36; P =0.51; I2 = 12%) and subgroup analysis (non-RCTs: OR 0.77; 95% CI, 0.43–1.38; P =0.38; I2 = 27%) (RCTs: OR 1.17; 95% CI, 0.49–2.81; P =0.73; I2 = 0%) (Figure 9).
 |
Figure 9 Forrest plots of perioperative complications. Abbreviation: CI, confidence interval. |
Discussion
This study intended to assess the efficacy of LB in improving recovery outcomes among patients undergoing thoracic surgery compared to non-liposomal local anesthetics. The findings of this systematic review and meta-analysis suggest that the current published evidence does not support the use of LB in thoracic surgery, either for analgesic purposes or for improving other perioperative outcomes.
The incidence of chronic pain after thoracotomy and thoracoscopy exceeds 35%. Given the correlation between acute pain severity and chronic pain occurrence,3 anesthesiologists have devoted significant attention to optimizing analgesia for thoracic surgery. Intercostal nerve injury is considered to be one of the causes of neuropathic pain after thoracic surgery,30 so INB is commonly used to reduce postoperative pain. However, the analgesic effect of INB is constrained by the limited duration of the anesthetic.31 Therefore, could the efficacy of INB be enhanced by the administration of long-acting anesthetic? This study was designed to address this inquiry. As a local anesthetic with extraordinarily long duration of action, LB has attracted extensive attention in recent years, but its actual effects are not satisfactory. Our results are consistent with some previous studies,7,32 compared with non-liposomal local anesthetics, LB does not show advantages in postoperative analgesia, does not reduce opioid consumption, nor does it reduce pain scores.
On one hand, when bupivacaine makes initial contact with injected tissue, it initiates a local inflammatory response that alters the pH in the surrounding area. This alteration causes LB to remain stagnant outside of the tissue cells, preventing its penetration and reducing its analgesic effectiveness.33 On the other hand, surgical interventions can also induce inflammatory responses that increase tissue acidity and hinder the penetration of local anesthetics into nerve cells. Additionally, inflammatory mediators can directly affect nociceptors, leading to peripheral sensitization and further diminishing the activity of local anesthetics.34 Therefore, the inflammatory reaction may be the main reason why the clinical efficacy of LB cannot surpass that of non-liposomal local anesthetics. Expanding the scope of nerve block, changing the method of nerve block, and adjusting drug dosages may enhance therapeutic effects and improve perioperative outcomes, which warrants further investigation.
In addition to opioid utilization and pain scores, we also analyzed other perioperative outcomes. The LOS for patients undergoing thoracic surgery is influenced by various factors, including age, complications, postoperative pain, and so on. There are no statistically significant differences in postoperative pain scores between the two groups, suggesting that the recovery process was comparable regardless of whether LB or non-liposomal local anesthetic was utilized. The findings of some studies also indicate that LB does not result in a reduction in the LOS,35,36 which aligns with our conclusion. However, subgroup analysis revealed that in the non-RCTs, the LOS was shorter in the LB group, which might require further confirmation through more high-quality studies.
Only two studies15,17 with 306 patients analyzed the time to first ambulation after surgery. The majority of patients try to get out of bed within 24 to 48 hours after surgery, but many are still affected by the traditional belief that too early activity will cause severe pain.37 Postoperative pain is an important factor affecting patients’ early mobilization. The findings of this study reveal no statistically significant disparity in pain scores between the two groups at 24 and 48 hours postoperatively, which may elucidate the absence of a statistical distinction in the time taken for initial ambulation between the two groups.
The most common reasons for readmission are respiratory or airway complications and infections.38 There are no statistically significant differences in readmissions observed between the two groups, likely due to the lack of impact of LB on perioperative complications.
Although existing studies indicated that LB management was associated with a reduction in pulmonary complications, as compared with nonuse,39 the results of our study indicate that there are no statistically significant differences in the reduction of perioperative complications between LB and non-liposomal agents. Similar results have been reported by other studies.35,40,41 In their data analysis, they found no benefits of LB in patients undergoing other procedures.
There are several limitations in our meta-analysis. First, the study only incorporated two RCTs, while retrospective or observational studies were susceptible to confounding factors and bias, potentially impacting the conclusions drawn from the meta-analysis. By including more RCTs, the statistical validity of the findings will be enhanced. Second, heterogeneity in some results was high, especially among non-RCTs, which may affect the reliability of our study. Third, data presentation (median or mean) varied across studies. Data conversions were undertaken to ensure that the most studies were included in the review, which may have introduced bias in our results. We expect that future clinical studies will stringently control all aspects such as the participants, intervention measures, blinding methods, and result analyses, and provide genuine and lucid data when publishing articles, which is conducive to enhancing the robustness of future meta-analyses.
Conclusion
In conclusion, our study failed to demonstrate clinically significant improvements in inpatient opioid dose, pain scores, or other outcomes among patients undergoing thoracic surgery who received LB, which may offer valuable insights for future research and guiding clinical medication. Considering the existing literature suggesting limited benefits of LB, cautious consideration should be given to its use. Future investigations should assess the efficacy of LB separately for different surgical procedures and routes of administration.
Abbreviations
LB, liposomal bupivacaine; RCTs, randomized controlled trials; MMEs, morphine milligram equivalents; LOS, length of stay; ERAS, enhanced recovery after surgery; INB, intercostal nerve block; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; ROBINS-I, Risk Of Bias in Non-randomized Studies of Interventions; MD, mean difference; CIs, confidence intervals; OR, odds ratio; SD, standard deviation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Support was provided from National High Level Hospital Clinical Research Funding (2022-PUMCH-B-006).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marshall K, McLaughlin K. Pain management in thoracic surgery. Thorac Surg Clin. 2020;30(3):339–346. doi:10.1016/j.thorsurg.2020.03.001
2. Ren Y, Wei M, Liu H, et al. Efficacy and safety of dexmedetomidine as an adjuvant to local wound infiltration anaesthesia: a meta-analysis with trial sequential analysis of 23 randomised controlled trials. Int Wound J. 2021;18(1):32–48. doi:10.1111/iwj.13517
3. Feray S, Lemoine A, Aveline C, Quesnel C. Pain management after thoracic surgery or chest trauma. Minerva Anestesiol. 2023;89(11):1022–1033. doi:10.23736/s0375-9393.23.17291-9
4. van Boekel RLM, Warlé MC, Nielen RGC, et al. Relationship between postoperative pain and overall 30-day complications in a broad surgical population: an observational study. Ann Surg. 2019;269(5):856–865. doi:10.1097/sla.0000000000002583
5. Bayman EO, Curatolo M, Rahman S, Brennan TJ. AAAPT diagnostic criteria for acute thoracic surgery pain. J Pain. 2021;22(8):892–904. doi:10.1016/j.jpain.2021.03.148
6. Yoon S, Hong WP, Joo H, et al. Long-term incidence of chronic postsurgical pain after thoracic surgery for lung cancer: a 10-year single-center retrospective study. Reg Anesth Pain Med. 2020;45(5):331–336. doi:10.1136/rapm-2020-101292
7. Abbas AE. Commentary: liposomal bupivacaine intercostal nerve block. All that is gold does not glitter. J Thorac Cardiovasc Surg. 2021;161(5):1662–1663. doi:10.1016/j.jtcvs.2020.01.030
8. Bajwa MS, Bashir MM, Bajwa MH, et al. How long to wait after local infiltration anaesthesia: systematic review. BJS Open. 2023;7(5). doi:10.1093/bjsopen/zrad089
9. Collins JB, Song J, Mahabir RC. Onset and duration of intradermal mixtures of bupivacaine and lidocaine with epinephrine. Can J Plast Surg. 2013;21(1):51–53. doi:10.1177/229255031302100112
10. Ilfeld BM, Eisenach JC, Gabriel RA. Clinical effectiveness of liposomal bupivacaine administered by infiltration or peripheral nerve block to treat postoperative pain. Anesthesiology. 2021;134(2):283–344. doi:10.1097/aln.0000000000003630
11. Chintalapudi N, Agarwalla A, Bortman J, et al. Liposomal bupivacaine associated with cost savings during postoperative pain management in fragility intertrochanteric hip fractures. Clin Orthop Surg. 2022;14(2):162–168. doi:10.4055/cios21024
12. McCann ME. Liposomal Bupivacaine. Anesthesiology. 2021;134(2):139–142. doi:10.1097/aln.0000000000003658
13. Campos JH, Seering M. Does liposomal bupivacaine have any advantage over bupivacaine hydrochloride for intercostal nerve blocks in minimally invasive thoracic surgery? J Cardiothorac Vasc Anesth. 2021;35(5):1399–1403. doi:10.1053/j.jvca.2021.01.023
14. Louis SG, King C, Baral P, Veeramachaneni N. Liposomal bupivacaine enhances the pain-control benefits of uniportal thoracoscopic lobectomy. Ann Thorac Surg. 2019;108(5):1514–1518. doi:10.1016/j.athoracsur.2019.04.095
15. Banks K, Ely S, Hsu DS, et al. Intercostal nerve blockade with liposomal bupivacaine reduces length of stay after video assisted thoracic surgery (VATS) lobectomy. J Thorac Dis. 2022;14(1):18–25. doi:10.21037/jtd-21-1583
16. Weksler B, Sullivan JL, Schumacher LY. Randomized trial of bupivacaine with epinephrine versus bupivacaine liposome suspension in patients undergoing minimally invasive lung resection. J Thorac Cardiovasc Surg. 2021;161(5):1652–1661. doi:10.1016/j.jtcvs.2020.01.112
17. Thuppal S, Sleiman A, Chawla K, et al. Randomized trial of bupivacaine versus liposomal bupivacaine in minimally invasive lobectomy. Ann Thorac Surg. 2022;114(4):1128–1134. doi:10.1016/j.athoracsur.2022.02.058
18. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
19. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:4898. doi:10.1136/bmj.l4898
20. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi:10.1136/bmj.i4919
21. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
22. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135. doi:10.1186/1471-2288-14-135
23. Cai Z, Fan X. A comparison of fixed-effects and random-effects models for multivariate meta-analysis using an SEM approach. Multivariate Behav Res. 2020;55(6):839–854. doi:10.1080/00273171.2019.1689348
24. Parascandola SA, Ibañez J, Keir G, et al. Liposomal bupivacaine versus bupivacaine/epinephrine after video-assisted thoracoscopic wedge resection†. Interact Cardiovasc Thorac Surg. 2017;24(6):925–930. doi:10.1093/icvts/ivx044
25. Dominguez DA, Ely S, Bach C, Lee T, Velotta JB. Impact of intercostal nerve blocks using liposomal versus standard bupivacaine on length of stay in minimally invasive thoracic surgery patients. J Thorac Dis. 2018;10(12):6873–6879. doi:10.21037/jtd.2018.10.124
26. Kelley TM, Bailey DW, Sparks P, et al. Intercostal nerve blockade with exparel® results in lower opioid usage during the first 24 hours after video-assisted thorascopic surgery. Am Surg. 2018;84(9):1433–1438. doi:10.1177/000313481808400945
27. Rincavage M, Hammond L, Reddy S, Sytsma C, Prater A, Brackbill M. Pain control using liposomal bupivacaine versus bupivacaine for robotic assisted thoracic surgery. Int J Clin Pharm. 2019;41(1):258–263. doi:10.1007/s11096-018-0776-8
28. Pedoto A, Noel J, Park BJ, Amar D. Liposomal bupivacaine versus bupivacaine hydrochloride for intercostal nerve blockade in minimally invasive thoracic surgery. J Cardiothorac Vasc Anesth. 2021;35(5):1393–1398. doi:10.1053/j.jvca.2020.11.067
29. Kodia K, Razi SS, Stephens-McDonnough JA, Szewczyk J, Villamizar NR, Nguyen DM. Liposomal bupivacaine versus bupivacaine/epinephrine intercostal nerve block as part of an Enhanced Recovery After Thoracic Surgery (ERATS) care pathway for robotic thoracic surgery. J Cardiothorac Vasc Anesth. 2021;35(8):2283–2293. doi:10.1053/j.jvca.2021.02.065
30. Takenaka S, Saeki A, Sukenaga N, et al. Acute and chronic neuropathic pain profiles after video-assisted thoracic surgery: a prospective study. Medicine. 2020;99(13):e19629. doi:10.1097/md.0000000000019629
31. Sheets NW, Davis JW, Dirks RC, et al. Intercostal nerve block with liposomal bupivacaine vs epidural analgesia for the treatment of traumatic rib fracture. J Am Coll Surg. 2020;231(1):150–154. doi:10.1016/j.jamcollsurg.2019.12.044
32. Uskova A, O’Connor JE. Liposomal bupivacaine for regional anesthesia. Curr Opin Anaesthesiol. 2015;28(5):593–597. doi:10.1097/aco.0000000000000240
33. Hussain N, Brull R, Sheehy B, et al. Perineural liposomal bupivacaine is not superior to nonliposomal bupivacaine for peripheral nerve block analgesia. Anesthesiology. 2021;134(2):147–164. doi:10.1097/aln.0000000000003651
34. Ottoboni T, Quart B, Pawasauskas J, Dasta JF, Pollak RA, Viscusi ER. Mechanism of action of HTX-011: a novel, extended-release, dual-acting local anesthetic formulation for postoperative pain. Reg Anesth Pain Med. 2019. doi:10.1136/rapm-2019-100714
35. Li Y, Shen Z, Wang H, Feng T, Xia Y. Efficacy of liposomal bupivacaine for pain control in shoulder surgery: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2022;31(9):1957–1968. doi:10.1016/j.jse.2022.02.037
36. Jiang H, Ma Q, Dong J, Ye X. The effect of liposomal bupivacaine for surgical wound infiltration: a meta-analysis of randomised controlled trials. Int Wound J. 2023;20(5):1591–1608. doi:10.1111/iwj.14015
37. Ding X, Zhang H, Liu H. Early ambulation and postoperative recovery of patients with lung cancer under thoracoscopic surgery-an observational study. J Cardiothorac Surg. 2023;18(1):136. doi:10.1186/s13019-023-02263-9
38. Kogon BE, Oster ME, Wallace A, et al. Readmission after pediatric cardiothoracic surgery: an analysis of the society of thoracic surgeons database. Ann Thorac Surg. 2019;107(6):1816–1823. doi:10.1016/j.athoracsur.2019.01.009
39. Corsini EM, Mitchell KG, Zhou N, et al. Liposomal bupivacaine intercostal block is important for reduction of pulmonary complications. Ann Thorac Surg. 2021;112(2):423–429. doi:10.1016/j.athoracsur.2020.09.017
40. Chitty L, Ridley B, Johnson B, Ibrahim M, Mongan PD, Hoefnagel AL. Liposomal compared to 0.25% bupivacaine in patients undergoing hemorrhoidectomy: a pre- and post-implementation quality improvement evaluation. J Clin Anesth. 2022;80:110868. doi:10.1016/j.jclinane.2022.110868
41. Pichler L, Poeran J, Zubizarreta N, et al. Liposomal bupivacaine does not reduce inpatient opioid prescription or related complications after knee arthroplasty: a database analysis. Anesthesiology. 2018;129(4):689–699. doi:10.1097/aln.0000000000002267
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.