")
Back to Journals » Journal of Inflammation Research » Volume 17
The Hemoglobin, Albumin, Lymphocyte, and Platelet (HALP) Score Predicts the Prognosis of Adults with Status Epilepticus: A Retrospective Study
Authors Fu J, Chen X, Li J, Rong B, Peng L
Received 15 August 2024
Accepted for publication 19 November 2024
Published 25 November 2024 Volume 2024:17 Pages 9625—9635
DOI https://doi.org/10.2147/JIR.S491666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Jie Fu,1 Xiu Chen,1 Jinglun Li,1 Benbing Rong,1 Lilei Peng2
1Department of Neurology, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 2Department of Neurosurgery, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China
Correspondence: Lilei Peng; Benbing Rong, Email [email protected]; [email protected]
Objective: The hemoglobin, albumin, lymphocyte, and platelet (HALP) score has been indicated to be a novel indicator that reflects systemic inflammation and is associated with the functional outcome in various neurological diseases. Since inflammation is closely involved in the pathogenesis of status epilepticus (SE), this study aimed to explore the predictive value of HALP for the prognosis of SE patients.
Methods: In the retrospective study, we investigated and validated the predictive value of HALP for the prognosis of adult SE patients. We collected patient’s clinical characteristics and laboratory test data. Information of 30-day mortality after SE onset was obtained, and modified Rankin scale (mRS) scores were used to evaluate the clinical outcomes. Multivariable logistic regression models were applied to explore the association between HALP and SE prognosis. Receiver operating characteristic (ROC) curve analysis was performed to determine the optimal cutoff of HALP to predict 30-day mortality in SE patients.
Results: We first analyzed the discovery cohort of 116 patients with SE. We observed that 19.0% (22/116) of the patients died within 30 days after SE onset, and 26.3% (20/76) had poor outcomes during the 6-month follow-up. Multivariate logistic regression analysis indicated that lower HALP on admission was an independent predictor of 30-day mortality (odds ratio: 0.980; 95% confidence interval, 0.962– 0.999; P = 0.044). In ROC analysis, a HALP of 20.32 was identified as the optimal cutoff value to predict 30-day mortality in SE patients. Furthermore, multivariate logistic regression analysis showed that HALP < 20.32 was related to an increased risk of poor SE outcomes (odds ratio: 27.051; 95% confidence interval, 3.589– 203.909; P = 0.001), which was validated in the external cohort.
Conclusion: Lower HALP is independently associated with an increased risk of 30-day mortality and poor functional outcomes in patients with SE. Our findings suggest that HALP may be a promising biomarker for predicting SE prognosis.
Keywords: status epilepticus, HALP score, inflammation, prognosis, biomarker
Introduction
Status epilepticus (SE) is a common neurological emergency with an incidence of 10 to 40 per 100,000 population.1 SE is associated with substantial mortality as well as long-term physical and cognitive impairments, which imposes a great burden on patients and their caregivers.2 Developing useful predictors of SE prognosis may aid in early recognition of high-risk patients with adverse outcomes, and thus early prevention could be implemented to reduce morbidity and mortality as well as improve the quality of life in SE patients.
Inflammation has been reported to exert a critical role in the pathogenesis of SE. SE can induce a rapid and intense inflammatory cascade in the brain, leading to the activation of microglia and astrocytes. Activated microglia and reactive astrocytes produce large amounts of pro-inflammatory mediators, which can increase neuronal excitability through neurogenesis, sprouting as well as neuronal damage, and further facilitates recurrent seizures.3 Various inflammatory biomarkers such as procalcitonin (PCT), C-reactive protein (CRP), and neutrophil-to-lymphocyte ratio (NLR) have been evidenced to be closely associated with the prognosis of SE.4–6 However, the associations between these markers and SE outcomes were inconsistent in different studies. For instance, NLR on admission was suggested to be independently associated with in-hospital mortality in patients with generalized convulsive SE,7 while the study by Olivo et al6 did not observe the signification relationship between admission NLR and short-term mortality in SE patients. Thus, it is essential to develop new and reliable markers or increase predictive items to improve the stability of predictions.
The hemoglobin, albumin, lymphocyte, and platelet (HALP) score is a novel indicator that reflects systemic inflammation and nutritional state.8 The HALP score was determined by hemoglobin (g/L)×albumin (g/L)×lymphocyte (/L) / platelet (/L),9 which was the combination of four laboratory markers and may be relatively more stable compared to individual blood indexes. Recent studies have indicated the predictive value of the HALP score for the risk and prognosis of cerebrovascular diseases, such as acute ischemic stroke,10 cerebral venous sinus thrombosis,11 and post-stroke cognitive impairment.12 Interestingly, cerebrovascular damage and reduced vascularization have been reported to be associated with the pathophysiological processes of SE and mesial temporal sclerosis, and drugs that afford vascular protection can reduce vascular lesions and subsequent neuronal cell loss during SE.13,14 However, whether HALP score is associated with the prognosis of SE patients remains unknown. Therefore, this study aimed to explore the predictive value of HALP score for the prognosis of adult patients with SE.
Methods
Study Design and Population
This retrospective study included two independent cohorts. Cohort 1 served as the discovery cohort, and we reviewed the medical records of patients with SE admitted to the department of neurology at the affiliated hospital of Southwest Medical University between January 2020 and December 2023. Cohort 2 was an external validation cohort, which enrolled a dataset of SE patients from the affiliated Traditional Chinese Medicine hospital of Southwest Medical University between January 2022 and December 2023. The inclusion criteria were age at least 18 years old and a diagnosis of SE, which was defined as a prolonged episode of clinical and/or electrographic seizure activity that persisted for over five minutes, or recurrent seizures without full functional recovery in between.15 The exclusion criteria were as follows: 1) patients with SE caused by hypoxic-ischemic encephalopathy after cardiac arrest; 2) patients with incomplete information; 3) patients were lost during follow-up. The Helsinki Declaration principles were followed during the entire study. This study was approved by the ethics committee of Southwest Medical University (Approval No.KY2024417). Informed consent was obtained from all patients or relatives.
Data Collection
Clinical characteristics were collected, including age; gender; etiology of SE; previous history of seizures; the number of antiepileptic drugs (AEDs); the modified Rankin scale (mRS) scores at admission; the Glasgow coma scale (GCS) scores at admission; the Charlson comorbidity index; comorbidities (hypertension, diabetes mellitus and previous stroke). SE etiology was categorized into the following groups: acute symptomatic SE, remote symptomatic SE, symptomatic SE due to progressive central nervous system disorders, or cryptogenic SE, which was defined by the International League Against Epilepsy (ILAE).4 Data of laboratory tests including red blood cell count, hemoglobin, red cell distribution width, white blood cell count, neutrophil count, lymphocyte count, monocyte count, platelet count, albumin, high density lipoprotein-cholesterol within 24 hours after admission were obtained. NLR was calculated as the ratio of neutrophil count to lymphocyte count. MLR was counted as the ratio of monocyte count to lymphocyte count. PLR was counted as the ratio of platelet count to lymphocyte count. MHR was defined as the ratio of monocyte count to high density lipoprotein-cholesterol. The formula was used to calculate HALP scores: hemoglobin (g/L) × albumin (g/L) × lymphocytes (/L) / platelets (/L).9
Outcome Assessment
The follow-up information was gained from the medical records or by interviewing (in person or by telephone) the patients and their family members. Data of mortality within 30 days after SE onset was collected. Then, surviving patients followed until 6 months after SE onset, and mRS scores were used to evaluate clinical outcomes. An mRS score of less than 3 was considered a good prognosis, while an mRS score of equal to or above 3 (including death) was considered a poor prognosis.16
Statistical Analysis
The Shapiro–Wilk test was employed to identify between normal and non-normal distributions. Continuous variables are expressed as means (standard deviation) or medians (interquartile range, IQR) for normally distributed and skewly distributed variables, respectively, while categorical variables were presented as frequency and percentage. Univariate analyses were conducted by using the t-test, the Mann–Whitney U-test and the chi-square (χ2) test. The t-test or Mann–Whitney U-test were used to compare continuous data, and the chi-square (χ2) test was carried out to compare categorical variables. Variables with P < 0.10 in the univariate analysis were entered into the multivariate logistic regression model. Multicollinearity was assessed with the variance inflation factor (VIF). The variable selected for further multivariate analysis was tolerance > 0.1 and VIF < 5. Receiver operating characteristic (ROC) curve analysis was applied to evaluate the predictive value of HALP for 30-day mortality in SE patients. The cutoff point of HALP was set by the Youden index. All statistical analyses were performed by using GraphPad Prism 9.0 and SPSS 26.0 softwares, and P values < 0.05 were defined as statistically significant.
Results
Baseline Characteristics of Patients with SE
In the Discovery cohort, after excluding 23 patients with hypoxic-ischemic encephalopathy, 12 patients with non-available data and 16 patients who were lost to follow-up, 116 SE patients were included. Among the 116 patients, 94 survived and 22 died within 30 days after SE onset. Out of the 94 surviving patients, follow-up data at 6 months after SE onset were available for 76 patients (80.9%). According to the mRS score, 73.7% (56/76) of patients had a good prognosis, and 26.3% (20/76) had a poor prognosis. In the external validation cohort, a total of 46 SE patients met the inclusion criteria and completed 6-month follow-up. Out of 46 SE patients, 33 patients (71.7%) had a good prognosis, and 13 patients (28.3%) had a poor prognosis.
HALP and 30-Day Mortality After SE Onset
The clinical and laboratory characteristics of 116 SE patients were presented in Table 1. Non-survivors had significantly higher baseline mRS scores, Charlson comorbidity index, white blood cell count, neutrophil count, NLR and MLR compared to survivors (all P < 0.05). Baseline GCS scores and the levels of lymphocyte count, albumin and HALP were lower in non-survivor than in survivors (all P < 0.05). There were no differences in gender, age, proportions of patients with SE caused by stroke or infection, previous history of seizures, the number of AEDs, proportions of patients with hypertension, diabetes mellitus or previous history of stroke, red blood cell count, hemoglobin, red cell distribution width, monocyte count, platelet count, high density lipoprotein-cholesterol, PLR and MHR in survivors and non-survivors (all P > 0.05). Subsequently, variables with P < 0.10 in the univariate comparisons were entered into the multivariate logistic regression model. The multivariate analysis demonstrated that HALP was independently associated with 30-day mortality in SE patients after adjusting for SE etiology, albumin, GCS score, MLR, Charlson comorbidity index and MHR [odds ratio: 0.980; 95% confidence interval, 0.962–0.999; P = 0.044] (Table 2).
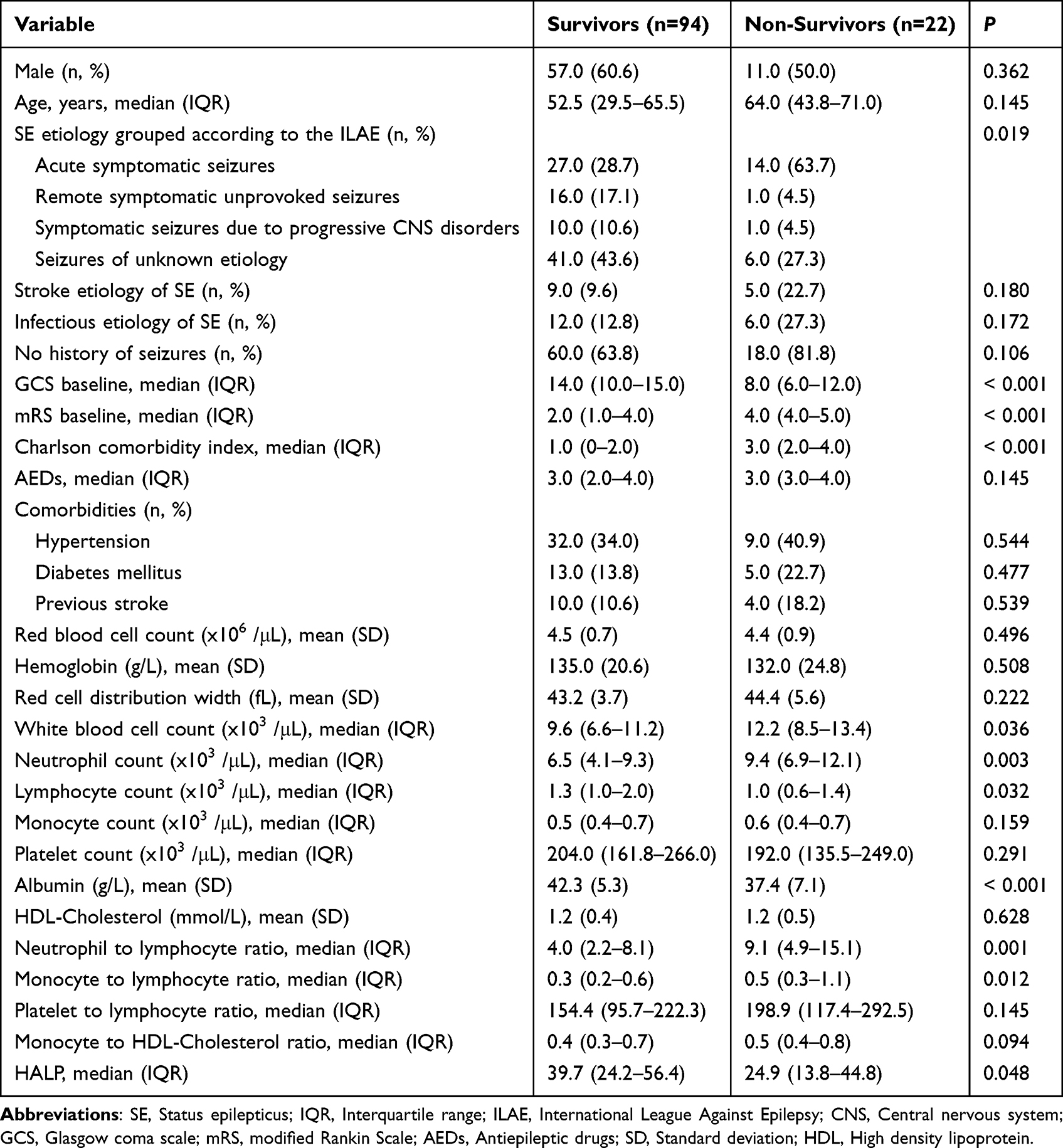 |
Table 1 Univariate Analysis of Clinical Characteristics and Laboratory Data Between Survivors and Non-Survivors |
 |
Table 2 Multivariate Analysis of Predictors for 30-Day Mortality in SE Patients |
The Predictive Power of HALP for 30-Day Mortality After SE Onset
We further performed the receiver operating characteristic (ROC) curve to assess the predictive ability of HALP for 30-day mortality in SE patients. The area under the ROC curve of HALP was 0.636 (95% confidence interval, 0.492–0.779, P = 0.048) for 30-day mortality (Figure 1). The optimal predictive cutoff value for 30-day mortality by HALP was 20.32 (sensitivity 50.0%, specificity 81.9%). Subsequently, 116 SE patients were categorized into two groups based on the cutoff point of HALP (HALP < 20.32 and HALP ≥ 20.32). We compared the data of 30-day mortality between the two groups (Table 3). As expected, compared to SE patients with HALP ≥ 20.32, a higher ratio of 30-day mortality was observed in SE patients with HALP < 20.32 (P = 0.002).
 |
Table 3 Comparison of Baseline Demographic and 30 Day-Mortality Between Patients with Different Levels of HALP |
 |
Figure 1 Receiver operating characteristic curve of HALP to predict 30-day mortality in SE patients. |
HALP and Poor Outcome at 6-Month Follow-Up
The clinical characteristics and data of laboratory tests of SE patients with good-prognosis and with poor-prognosis at 6-month follow-up were presented in Table 4. As shown in Table 4, SE patients with poor-prognosis had significantly higher baseline mRS scores, Charlson comorbidity index, white blood cell count, neutrophil count, monocyte count, platelet count, NLR, MLR, PLR and MHR compared to patients with good-prognosis (all P < 0.05). Baseline GCS scores and the levels of red blood cell count and HALP were lower in patients with poor-prognosis than in patients with good-prognosis (all P < 0.05). Of note, we also compared the proportion of patients with HALP less than 20.32 in SE patients with good-prognosis and with poor-prognosis, which indicated that SE patients with poor-prognosis had remarkably higher ratio of patients with HALP less than 20.32 (P < 0.001). Then, a multivariate logistic regression analysis including mRS score, GCS score, Charlson comorbidity index, albumin, red blood cell count, MHR and HALP < 20.32 was carried out, which suggested that HALP < 20.32 was an independent predictor for poor prognosis in SE patients (P = 0.001) (Table 5).
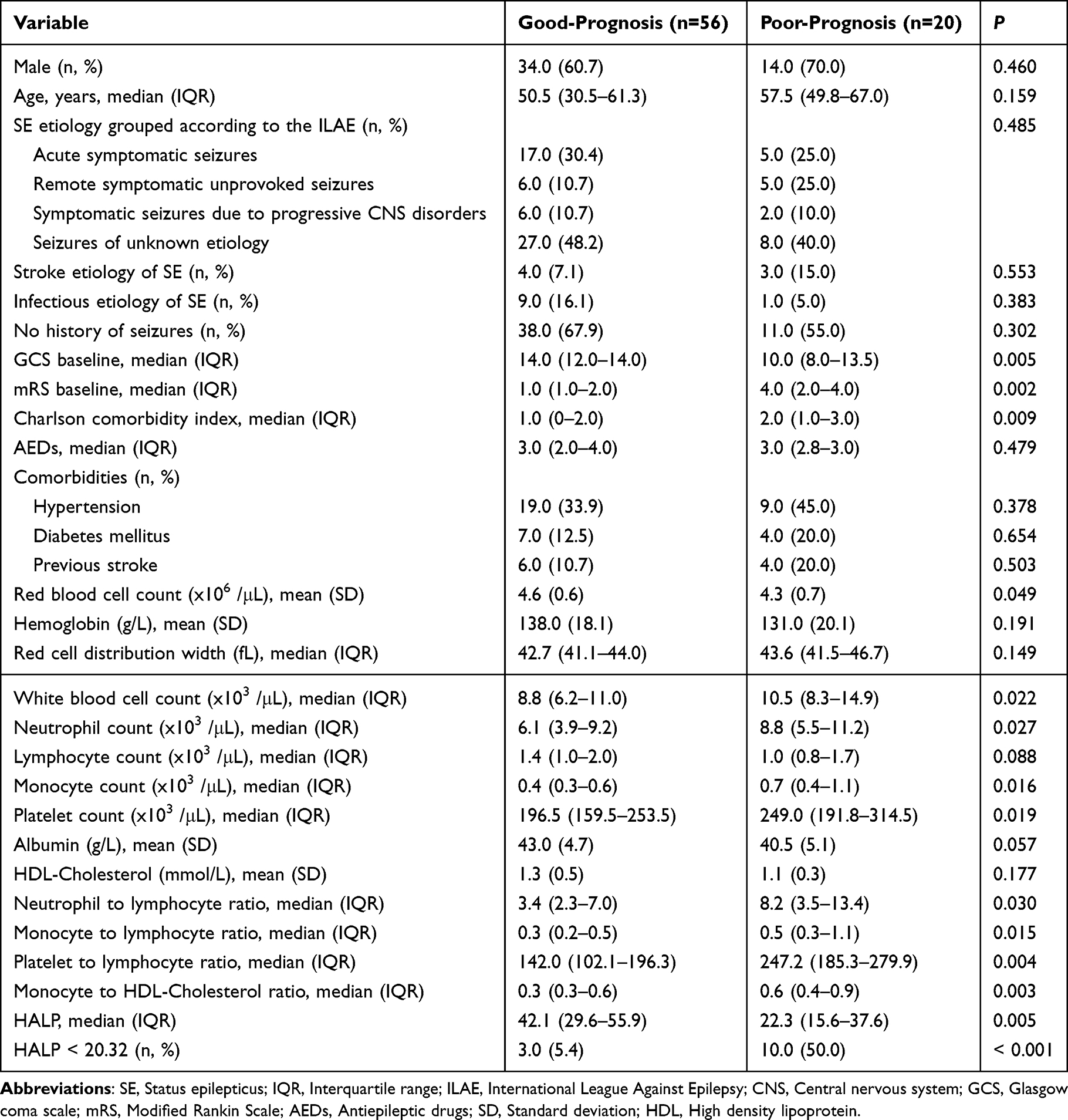 |
Table 4 Comparisons of Clinical Characteristics and Laboratory Data Between SE Patients with Good-Prognosis and Poor-Prognosis |
 |
Table 5 Multivariate Analysis of Predictors for Poor Outcome in SE Patients |
External Cohort Validated the Predictive Value of HALP for SE Prognosis
We further performed an external cohort to validate our results. Univariable and multivariable analyses conducted in the external cohort were present in Table 6 and Table 7, respectively. Univariable analysis identified GCS score, mRS score, Charlson comorbidity index, AEDs, diabetes mellitus, white blood cell count, neutrophil count, albumin, neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, HALP and HALP < 20.32 as prognostic factors for the outcome of SE patients (all P < 0.10, Table 6), and only GCS score, mRS score, Charlson comorbidity index, HALP < 20.32, diabetes mellitus, AEDs and albumin were entered into the multivariable analysis after multicollinearity assessment (Table 7). The multivariate analysis showed that HALP < 20.32 was independently associated with poor prognosis in SE patients (odds ratio: 43.872; 95% confidence interval, 2.238–859.988; P = 0.013). Thus, the results from the external cohort were in line with the findings of the discovery cohort, which further confirmed the predictive value of HALP for the prognosis of SE patients.
 |
Table 6 Comparisons of Clinical Characteristics and Laboratory Data Between SE Patients with Good-Prognosis and Poor-Prognosis in the External Validation Cohort |
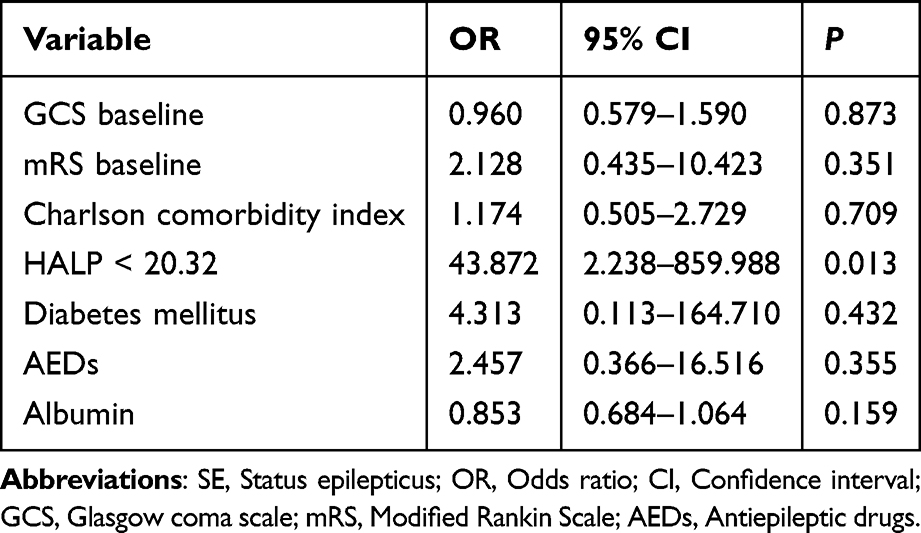 |
Table 7 Multivariate Analysis of Predictors for Poor Outcome in SE Patients in the External Validation Cohort |
Discussion
In the present study, a lower HALP at admission was recognized to be independently associated with a high risk of 30-day mortality and poor functional outcomes in SE patients. Our findings indicate that HALP, as an easily available inflammatory biomarker, may hold great potential to predict the prognosis of SE patients.
Inflammation is involved in the pathophysiological processes of SE. SE could disrupt the brain-blood barrier (BBB) and activate a wide range of cells, including microglia, astrocytes, monocyte-macrophages and neutrophils. Then, activated microglia, reactive astrocytes and the infiltrating immune cells could release massive pro-inflammatory cytokines, thus increasing brain excitability and reducing the threshold of seizure onset, ultimately inducing recurrent seizures, which causes a “vicious circle”.17 A variety of inflammatory biomarkers have been indicated to be useful predictors for SE outcomes. For instance, acute-phase proteins including PCT, CRP and albumin have been suggested to independently correlate with SE outcomes.4,5,18 Additionally, Hanin et al19 reported that the increased pro-inflammatory cytokines in patients with new-onset refractory SE were closely associated with worse short-term and long-term outcomes. In addition to single blood parameters, some ratios derived from two blood parameters have been also proposed to be associated with the prognosis of SE. NLR, the neutrophil to lymphocyte ratio, was suggested to be related to the length of hospitalization and need for ICU admission in patients with SE.6
The hemoglobin, albumin, lymphocyte, and platelet (HALP) score is a new emerging index that evaluates the inflammatory response and nutritional status in recent years. It was first reported by Chen et al20 in 2015. They found that hemoglobin, albumin, and lymphocyte may be positively associated with the prognosis of patients with gastric carcinoma, while platelet may be negatively related. Therefore, they proposed the HALP based on these four biochemical parameters to predict tumor prognosis, which indicated that HALP was an independent and accurate prognostic factor. Thereafter, HALP, as a potential predictor, has been identified to be related to the functional outcomes of various diseases.21–23 Consistently, in our study, we observed that low HALP was independently associated with poor prognosis of SE patients. Furthermore, SE patients with HALP less than 20.32 had higher 30-day mortality and worse outcomes during follow-up. Anemia characterized by low blood hemoglobin level has been suggested to be associated with epilepsy. Anemia could reduce the seizure threshold, leading to increased seizure activity. In addition, anemia may induce seizures through diverse processes, including a decline in inhibitory neurotransmitter gamma-aminobutyric acid, changes in neuron metabolism, enzyme decrease, and a decrease in brain oxygenation and energy metabolism.24 Albumin, as one of acute-phase proteins, was reported to be related to refractory epileptic activity and mortality in patients with SE.25 The effect of lymphocytes on epilepsy has been less investigated. Nevertheless, it seems that the levels of lymphocytes are remarkably decreased in convulsive SE patients.26 Several studies have demonstrated that lymphocytes could repair the injury via inflammation,27 and reduced lymphocyte level may reveal a poor outcome in systemic inflammatory diseases.12 Moreover, there is increasing acknowledgment of the vital role of platelets in inflammation responses. Activated platelets could release numerous inflammatory mediators, and platelets could also interact with leukocytes, thus promoting their release of pro-inflammatory cytokines.28 Given the above, it is reasonable to believe that HALP consisting of hemoglobin concentration, albumin level, lymphocyte count and platelet count is associated with SE.
Several studies have indicated that the HALP score can reflect the inflammation-nutritional status of patients and HALP may be a critical prognostic factor for patients with various tumors.29–31 Hemoglobin and albumin have been regarded as markers of nutritional status.32 Thrombosis could aggravate inflammation, while lymphocytes alleviate inflammation. Furthermore, it is reported that correction of low HALP may be beneficial to improve cancer-specific survival in patients with resectable esophageal squamous cell carcinoma.9 Our study indicated that HALP less than 20.32 was an independent predictor for poor SE outcomes. Thus, for SE patients with a low score of HALP (< 20.32), whether anti-inflammatory drugs to reduce inflammation or therapies to elevate the levels of hemoglobin and albumin can improve their prognosis needs further investigations, which could provide a novel therapeutic strategy.
In the current study, we also included some other inflammatory hematological ratios, such as NLR, MLR, PLR and MHR. These indicators have been suggested to be potential predictors for the outcomes of various neurological diseases, such as ischemic stroke,33–36 intracerebral hemorrhage37,38 and multiple sclerosis,39,40 etc. However, our study did not indicate the predictive value of these ratios in SE outcomes, while HALP was a promising factor for predicting SE prognosis that outperformed NLR, PLR, MLR and MHR in predictive power. We speculate that HALP that combines four indexes may be relatively more stable, which warrants additional studies.
The present study has some limitations. First, it was a single-center retrospective study with a relatively small sample size. Second, the blood samples tested in the present study were collected within 24 hours after admission, and dynamically monitoring alterations in blood indices is lacking. Third, our study only explored SE outcome within 6 months after SE onset, further investigations are needed to assess the correlation between the HALP and the long-term prognosis of SE.
Conclusion
In the present study, lower HALP was independently associated with 30-day mortality and unfavorable outcomes in SE patients. HALP may be a promising, easily available and cost-effective biomarker for predicting SE prognosis. Additionally, future studies are needed to determine the efficacy of correcting low HALP in SE patients for improving functional outcomes.
Data Sharing Statement
Data will be available from the corresponding authors on request.
Ethics Statement
This study was approved by the ethics committee of Southwest Medical University (Approval No. KY2024417). Informed consent was obtained from all patients or relatives.
Funding
This study was supported by the Doctoral Research Initiation Fund of Affiliated Hospital of Southwest Medical University (No. 21024).
Disclosure
The authors declare no potential conflicts of interests.
References
1. Hill CE, Parikh AO, Ellis C, Myers JS, Litt B. Timing is everything: where status epilepticus treatment fails. Ann Neurol. 2017;82:155–165. doi:10.1002/ana.24986
2. King-Stephens D, Wheless J, Krogh C, et al. Burden of disease in patients with a history of status epilepticus and their caregivers. Epilepsy Behav. 2020;112:107374. doi:10.1016/j.yebeh.2020.107374
3. Wang M, Chen Y. Inflammation: a network in the pathogenesis of status epilepticus. Front Mol Neurosci. 2018;11:341. doi:10.3389/fnmol.2018.00341
4. Sutter R, Valença M, Tschudin-Sutter S, Rüegg S, Marsch S. Procalcitonin and mortality in status epilepticus: an observational cohort study. Crit Care. 2015;19:361. doi:10.1186/s13054-015-1072-9
5. Madžar D, Reindl C, Mrochen A, Hamer HM, Huttner HB. Value of initial C-reactive protein levels in status epilepticus outcome prediction. Epilepsia. 2021;62:e48–e52. doi:10.1111/epi.16842
6. Olivo S, Buoite Stella A, Pavan S, et al. Admission neutrophil-to-lymphocyte ratio predicts length of hospitalization and need for ICU admission in adults with status Epilepticus. Seizure. 2023;106:80–84. doi:10.1016/j.seizure.2023.02.001
7. Wang D, Li M, Pan Y, et al. Risk factors for super-refractory and mortality in generalized convulsive status epilepticus: a 10-year retrospective cohort study. Ther Adv Neurol Disord. 2023;16:17562864231214846. doi:10.1177/17562864231214846
8. Xu M, Chen L, Hu Y, et al. The HALP (hemoglobin, albumin, lymphocyte, and platelet) score is associated with early-onset post-stroke cognitive impairment. Neurol Sci. 2023;44:237–245. doi:10.1007/s10072-022-06414-z
9. Feng JF, Wang L, Yang X. The preoperative hemoglobin, albumin, lymphocyte and platelet (HALP) score is a useful predictor in patients with resectable esophageal squamous cell carcinoma. Bosn J Basic Med Sci. 2021;21:773–781. doi:10.17305/bjbms.2021.5666
10. Tian M, Li Y, Wang X, et al. The Hemoglobin, Albumin, Lymphocyte, and Platelet (HALP) score is associated with poor outcome of acute ischemic stroke. Front Neurol. 2021;11:610318. doi:10.3389/fneur.2020.610318
11. Li S, Gao Y, Liu K, et al. The novel biomarkers-based HALP (Hemoglobin, Albumin, Lymphocyte and Platelet)-prognostic model for acute and subacute patients with cerebral venous sinus thrombosis: a retrospective cohort study. J Atheroscler Thromb. 2023;30(11):1742–1749. doi:10.5551/jat.64043
12. Zuo L, Dong Y, Liao X, et al. Low HALP (Hemoglobin, Albumin, Lymphocyte, and Platelet) score increases the risk of post-stroke cognitive impairment: a multicenter cohort study. Clin Interv Aging. 2024;19:81–92. doi:10.2147/CIA.S432885
13. Lucchi C, Vinet J, Meletti S, Biagini G. Ischemic-hypoxic mechanisms leading to hippocampal dysfunction as a consequence of status epilepticus. Epilepsy Behav. 2015;49:47–54. doi:10.1016/j.yebeh.2015.04.003
14. Mott RT, Thore CR, Moody DM, Glazier SS, Ellis TL, Brown WR. Reduced ratio of afferent to total vascular density in mesial temporal sclerosis. J Neuropathol Exp Neurol. 2009;68:1147–1154. doi:10.1097/NEN.0b013e3181b9d75f
15. Lin CH, Ho CJ, Lu YT, Shih FY, Chuang YC, Tsai MH. Predicting the functional outcome of adult patients with status epilepticus. J Clin Med. 2019;8:992. doi:10.3390/jcm8070992
16. Qiao S, Zhang SC, Zhang RR, et al. Thyroid function and low free triiodothyronine in Chinese patients with autoimmune encephalitis. Front Immunol. 2022;13:821746. doi:10.3389/fimmu.2022.821746
17. Rejdak K, Pikulicka A, Piekarska M, Pacek K, Płachta K. Inflammation as treatment target for status epilepticus. Curr Neuropharmacol. 2023;21:708–714. doi:10.2174/1570159X21666221117152249
18. Liao Q, Li SZ, Zeng QQ, Zhou JX, Huang K, Bi FF. The value of serum albumin concentration in predicting functional outcome of status epilepticus: an observational study. Epileptic Disord. 2023;25:150–159. doi:10.1002/epd2.20001
19. Hanin A, Cespedes J, Dorgham K, et al. Cytokines in New-onset refractory status epilepticus predict outcomes. Ann Neurol. 2023;94:75–90. doi:10.1002/ana.26627
20. Chen XL, Xue L, Wang W, et al. Prognostic significance of the combination of preoperative hemoglobin, albumin, lymphocyte and platelet in patients with gastric carcinoma: a retrospective cohort study. Oncotarget. 2015;6:41370–41382. doi:10.18632/oncotarget.5629
21. Zheng Y, Huang Y, Li H. Hemoglobin albumin lymphocyte and platelet score and all-cause mortality in coronary heart disease: a retrospective cohort study of NHANES database. Front Cardiovasc Med. 2023;10:1241217. doi:10.3389/fcvm.2023.1241217
22. Gursoy V, Sadri S, Kucukelyas HD, et al. HALP score as a novel prognostic factor for patients with myelodysplastic syndromes. Sci Rep. 2024;14:13843. doi:10.1038/s41598-024-64166-6
23. Liu L, Gong B, Wang W, Xu K, Wang K, Song G. Association between haemoglobin, albumin, lymphocytes, and platelets and mortality in patients with heart failure. ESC Heart Fail. 2024;11:1051–1060. doi:10.1002/ehf2.14662
24. Padda J, Khalid K, Syam M, et al. Association of anemia with epilepsy and antiepileptic drugs. Cureus. 2021;13:e19334. doi:10.7759/cureus.19334
25. Sutter R, Grize L, Fuhr P, Rüegg S, Marsch S. Acute-phase proteins and mortality in status epilepticus: a 5-year observational cohort study. Crit Care Med. 2013;41:1526–1533. doi:10.1097/CCM.0b013e318287f2ac
26. Güneş M, Büyükgöl H. Relationship between generalized epileptic seizure and neutrophil/lymphocyte ratio, platelet/lymphocyte ratio, and neutrophil mediated inflammation. Int J Neurosci. 2020;130:1095–1100. doi:10.1080/00207454.2020.1722662
27. Zou F, Wang J, Han B, Bao J, Fu Y, Liu K. Early neutrophil-to-lymphocyte ratio is a prognostic marker in acute ischemic stroke after successful revascularization. World Neurosurg. 2022;157:e401–e409. doi:10.1016/j.wneu.2021.10.097
28. Thomas MR, Storey RF. The role of platelets in inflammation. Thromb Haemost. 2015;114:449–458. doi:10.1160/TH14-12-1067
29. Xu SS, Li S, Xu HX, et al. Haemoglobin, albumin, lymphocyte and platelet predicts postoperative survival in pancreatic cancer. World J Gastroenterol. 2020;26:828–838. doi:10.3748/wjg.v26.i8.828
30. Duzkopru Y, Kocanoglu A, Dogan O, Sahinli H, Cilbir E, Altinbas M. Hemoglobin, albumin, lymphocyte, and platelet score as a predictor of prognosis in metastatic gastric cancer. World J Gastrointest Oncol. 2023;15:1626–1635. doi:10.4251/wjgo.v15.i9.1626
31. Vlatka P, Marko L, Stefan M, Dorian L. The hemoglobin, albumin, lymphocyte, and platelet (HALP) score is a novel prognostic factor for patients with diffuse large B-cell lymphoma. J Cancer Res Ther. 2022;18:725–732. doi:10.4103/jcrt.jcrt_174_21
32. Serra MC, Hafer-Macko CE, Ivey FM, Macko RF, Ryan AS. Impact of serum nutritional status on physical function in African American and caucasian stroke survivors. Stroke Res Treat. 2014;2014:174308. doi:10.1155/2014/174308
33. Chen C, Gu L, Chen L, et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as potential predictors of prognosis in acute ischemic stroke. Front Neurol. 2021;11:525621. doi:10.3389/fneur.2020.525621
34. Quan K, Wang A, Zhang X, et al. Neutrophil to lymphocyte ratio and adverse clinical outcomes in patients with ischemic stroke. Ann Transl Med. 2021;9:1047. doi:10.21037/atm-21-710
35. Wang CJ, Pang CY, Cheng YF et al. Monocyte-to-lymphocyte ratio affects prognosis in LAA-type stroke patients. Heliyon. 2022;8:e10948. doi:10.1016/j.heliyon.2022.e10948
36. Xu Q, Wu Q, Chen L, et al. Monocyte to high-density lipoprotein ratio predicts clinical outcomes after acute ischemic stroke or transient ischemic attack. CNS Neurosci Ther. 2023;29:1953–1964. doi:10.1111/cns.14152
37. Li L, Zhang H, Feng GL. Neutrophil-to-lymphocyte ratio predicts in-hospital mortality in intracerebral hemorrhage. J Stroke Cerebrovasc Dis. 2022;31:106611. doi:10.1016/j.jstrokecerebrovasdis.2022.106611
38. You S, Zhong C, Zheng D, et al. Monocyte to HDL cholesterol ratio is associated with discharge and 3-month outcome in patients with acute intracerebral hemorrhage. J Neurol Sci. 2017;372:157–161. doi:10.1016/j.jns.2016.11.022
39. Huang WC, Lin HC, Yang YH, et al. Neutrophil-to-lymphocyte ratio and monocyte-to-lymphocyte ratio are associated with a 2-year relapse in patients with multiple sclerosis. Mult Scler Relat Disord. 2022;58:103514. doi:10.1016/j.msard.2022.103514
40. Ulusoy EK, Bolattürk ÖF, Göl MF. Relation between the novel marker monocyte to high-density lipoprotein cholesterol ratio and severity in multiple sclerosis. Ann Indian Acad Neurol. 2020;23:275–279. doi:10.4103/aian.AIAN_249_19
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.