")
Back to Journals » Journal of Inflammation Research » Volume 17
The Mediating Role of Inflammation and Coagulation in the Association Between COVID-19 and 3-Month Outcome After Stroke During the Omicron Wave
Authors Zhan L, Zhang Y, Li Y , Lin C, Zhang H, Liu Y , He J
Received 9 April 2024
Accepted for publication 16 August 2024
Published 10 October 2024 Volume 2024:17 Pages 7171—7182
DOI https://doi.org/10.2147/JIR.S465127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Luqian Zhan,1,* Ye Zhang,2,* Yanwei Li,3 Chenhui Lin,3 Heyu Zhang,3 Yuntao Liu,3 Jincai He3
1Department of Neurology, Integrated Traditional Chinese and Western Medicine Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China; 2Third Department of Cerebrovascular Disease, Cangzhou Central Hospital, Cangzhou, People’s Republic of China; 3Department of Neurology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jincai He; Yuntao Liu, Department of Neurology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Acute ischemic stroke (AIS) patients with COVID-19 have severe neurological symptoms and high mortality. It remains unclear how COVID-19 causes unfavorable outcomes. This study aimed to explore the possible mechanism focusing on inflammation and coagulation.
Patients and Methods: 109 AIS patients were recruited and followed up 3 months after stroke. We used binary logistic regression to investigate if COVID-19 infection is an independent prognostic factor. To analyze the link between inflammation, coagulation, and neurological outcomes, we used mediation analysis.
Results: Compared to the non-COVID-19 group, the COVID-19 group had significantly higher fibrinogen (FIB) (P < 0.001), APTT ratio (P < 0.001), D-dimer (P < 0.001), CRP (P < 0.001). Patients with unfavorable outcomes had a higher incidence of COVID-19 infection (P = 0.002), along with elevated levels of INR (P = 0.005), D-dimer (P < 0.001), and CRP (P = 0.012). The significant association between 3-month functional outcomes and COVID-19 tends to be insignificant (P = 0.294) after adding the covariates of inflammation and coagulation. The mediation analyses showed the APTT ratio mediated the association between COVID-19 and the 3-month outcome (percent mediation = 56.3%). The integrated pathway analysis implicated that the path of COVID-19 infection→CRP→APTT ratio→ 3-month outcome was significant (percent mediation = 18.7%).
Conclusion: AIS with COVID-19 had a poorer prognosis. We delineated a more accurate mechanism by which COVID-19 influences functional outcomes: COVID-19 infection→inflammation→endogenous coagulation pathway→poor stroke outcome. This study provided new insight into the pathway mechanisms of AIS with COVID-19.
Keywords: COVID-19, Omicron, stroke, mediation analysis, APTT ratio
Introduction
Stroke is the leading cause of disability and death worldwide. For people over 40 years old in China, the prevalence, incidence, and death rate of stroke in 2020 were 2.6%, 505.2 per 100,000 person-years, and 343.4 per 100,000 person-years respectively.1 The most common subtype is ischemic stroke. The potential long-term effects of ischemic events include physical disabilities, mood disorders such as depression and anxiety, insomnia, and cognitive impairments.2 Since 2019, the COVID-19 pandemic has swept the world. As of the 22nd of November 2023, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has infected more than 772 million individuals worldwide and has caused over 6.9 million deaths.3 Based on the COVID-19 infection situation in China, as published by the Chinese Center for Disease Control and Prevention (CDC), the Omicron subvariants BA.5.2 and BF.7 were primarily strains in December 2022 and it is evident that COVID-19 can result in reinfection and may not disappear quickly.4 The presence of virus mutations and evolution still poses a risk of a COVID-19 pandemic. Long COVID-19 symptoms, including cough, brain fog, loss of smell, trouble sleeping, and mood changes can last many months.5 Due to mutations on the spike protein, Omicron was highly transmissible. Even though most affected individuals experienced only mild symptoms, AIS patients may experience a worse outcome if infected.6
Research shows that COVID-19 patients with stroke have severe neurological symptoms, higher mortality, and higher modified Rankin Scale (mRS) scores at discharge.7,8 Some of the important reasons for the aggravation of stroke severity caused by COVID-19 are hypercoagulable state, hyperinflammatory state leading to thrombus expansion, and aggravation of local inflammatory response. Studies have shown that in the hyperinflammatory state of COVID-19, locally activated platelets induced the release of neutrophil extracellular traps covered with tissue factor to activate exogenous coagulation, and NETs release histone and DNA fragments to activate endogenous coagulation and lead to the formation of thrombin.9 Therefore, both endogenous and exogenous coagulation pathways are activated and involved in the hypercoagulable state caused by COVID-19. Some clinical studies have suggested that CRP, fibrinogen, and D-dimer were increased in COVID-19 patients, and platelet count, PT, and APTT are usually normal or nearly normal. Abnormal prolongation of PT and APTT was seen in non-survivors.9
At present, there is a lack of research on the potential pathway mechanism of the poor prognosis of COVID-19 patients with stroke. Moreover, due to the high prevalence of COVID-19, the control groups (stroke without COVID-19) were not enrolled at the same time, which reduced the reliability of the results. Considering that inflammation and coagulation pathways play a critical role, the present study explored the above mechanism of the unfavorable outcome of stroke caused by COVID-19.
Methods
Study Population
Our research focuses on ischemic stroke patients at the First Affiliated Hospital of Wenzhou Medical University from December 2022 to February 2023. The inclusion standards were: (1) age >18 years old (2) CT or MRI confirmed AIS (3) admitted within 1 week of AIS (4) obtain informed consent. The exclusion standards were: (1) had a history of mental disorders, cancer, and other severe organic diseases (2) unconsciousness, aphasia, and cognitive dysfunction that cannot complete scales (3) had an infection during hospitalization, except for COVID-19 (4) incomplete clinical data. The diagnosis criteria of COVID-19 include 3 items: (1) had actual epidemiology (2) had symptoms like high fever and cough (3) SARS-CoV-2 nucleic acid test was positive when admission or discharge within 2 weeks.
Figure 1 outlines the screening and selection process. We screened 326 AIS patients and finally, 139 patients were recruited (61 COVID-19 AIS patients, and 48 non-COVID-19 AIS patients). Figure S1 shows the time interval between COVID-19 symptoms and stroke in AIS with COVID-19 patients, over 88.5% of patients were in the acute phase (stroke onset ±7 days) of COVID-19 and stroke. We compared the basic characteristics of the lost follow-up population and the study cohort and found that there were no significant differences in demographics, clinical data, and important blood indicators, except for NIHSS scores at admission (Table S1).
 |
Figure 1 The flow of participants. Abbreviation: AIS, acute ischemic stroke. |
This study was performed in line with the principles of the Declaration of Helsinki. Due to the high number of COVID-19 patients in the hospital wards and the high transmissibility of the Omicron variant during the observation period, we opted to contact patients by phone instead of in person to reduce the risk of virus transmission to both researchers and participants. Participants verbally consented to participate in the study, and their consent was documented through recorded phone calls. The study and the methods employed to secure informed consent were approved by the ethics committee of the First Affiliated Hospital of Wenzhou Medical University.
Baseline Data Collection
We collected demographic data and cerebral vascular risk factors from electronic medical records and primary nursing records. Demographic data included age, gender, and body mass index (BMI). Vascular risk factors include smoking history, drinking history, hypertension, and diabetes mellitus. Clinical data were collected: history of stroke, stroke severity, stroke subtyping, hemorrhagic transformations, early neurological deterioration (END), venous thromboembolism events detected during hospitalization (VTE detected), anticoagulation use, and glucocorticoid use during hospitalization. In Table S2, we have added detailed information about anticoagulation treatment, including the anticoagulant treatments, encompassing both oral and parenteral options, along with their respective dosages and durations of treatment. Experienced neurologists assessed stroke severity using the National Institutes of Health Stroke (NIHSS) Scale. We clarified the stroke subtyping according to the TOAST criteria, which were used to assign the likely stroke etiology as large-artery atherosclerosis, cardio aortic embolism, small-artery occlusion, and other determined etiology or undetermined etiology. END was defined as an increase of ≥2 points in the NIHSS within the first 72 hours.
Laboratory tests included lymphocyte absolute value, platelets, LDH, CRP, serum calcium, coagulation function, and NT-proBNP. To make the two groups maximally comparable, we chose and measured the blood samples after they had symptoms of COVID-19 within 6 hours (COVID-19 AIS group) or in the early morning of day 2 of hospitalization (non-COVID-19 AIS group). Since the time point of the blood sample we took might be different (the day after admission vs had symptoms of COVID-19 within 6 hours), we explored the difference in blood draw time after stroke onset and found there was no statistical difference between the two groups [non-COVID-19 vs COVID-19, 2 (1–4) vs 3 (1–5), P = 0.478]. The coagulation analyses were performed using an STA R Max Coagulation Analyzer (Stago). Biochemistry parameters were tested by an AU5800 (Beckman Coulter). Blood cell counts were examined using an automated hematology analyzer (Mindray, BC-6800vet, China).
Outcome Assessment and Follow-Up
Patients were followed up 3 months after discharge by telephone interview. The mRS score was used to evaluate the functional outcome. Patients were divided into a favorable outcome group (mRS score: 0–1 points) and an unfavorable outcome group (mRS score ≥ 2 points). In addition, we recorded whether patients experienced a stroke recurrence or died.
Statistical Analysis
The continuous variables of normal distribution were evaluated by Student’s t-test and described by mean ± SD. The variables of skewness distribution were shown as median (25–75%) and analyzed using Mann–Whitney U-tests. Categorical variables were shown as proportions, and group differences were analyzed using the chi-square or Fisher’s exact tests. We used Binary logistic regression analyses to investigate if COVID-19 infection is an independent prognostic factor. Variables reflecting significant group differences (P < 0.05) or influencing the prognosis theoretically were considered confounding factors and included in the Model. Model 1 includes age, gender, and BMI. Model 2 includes Model 1, adding hypertension, diabetes, and NIHSS score. We sought to explore the mediate effects of inflammation and coagulation between COVID-19 and neurological outcomes. Given the limited number of cases, and to ensure the stability of the model, we selected representative blood indicators for inclusion in Model 3 based on our research objectives. Lymphocyte absolute value and CRP were well-established inflammatory markers, and so as the INR (exogenous pathway) and APTT ratio (endogenous pathway) for coagulation. We tested for multicollinearity among these predictors, and assessed the tolerance (TOL) and variance inflation factors (VIFs). All the TOL> 0.2 and all the VIFs <5, and thus the multicollinearity does not exist in the three models. We use INR instead of Prothrombin time (PT) to measure the exogenous coagulation pathway, which was adjusted for variations in PT measurements. APTT ratio is the patient’s coagulation time compared to normal, which was normalized and measures the endogenous coagulation pathway.10 Thus, Model 3 included the above indicators representing the mechanism of inflammation and coagulation.
The associations between COVID-19 and prognosis were not a simple direct correlation, we used PROCESS V4.2 by Andrew F. Hayes to test the significance of the mediating effect. We took COVID-19 infection as the independent variable, and 3-month mRS as the dependent variable, to explore whether CRP, APTT ratio, and other indicators play a mediating effect. Furthermore, we estimated the effect of a hypothesized serial, dual mediator path: COVID-19 infection→CRP→APTT ratio→3-month mRS. The simple mediating model was tested by PROCESS model 4, and the dual mediating model by PROCESS model 6. We adjusted age, gender, BMI, hypertension, diabetes, and NIHSS score. All mediating models were based on a 5000-sample bootstrapping set. All data analysis was calculated by IBM SPSS statistical software Version 26 and two-tailed P-values < 0.05 were considered statistically significant.
Results
Baseline Characteristics of AIS with or Without COVID-19
Age, gender, and NIHSS scores at admission between the two groups had no significant difference, indicating that the two groups were comparable at the baseline. Compared to non-COVID-19, patients with COVID-19 had higher BMI (kg/m2) (25.07 ± 3.38 vs 23.84 ± 2.77, P = 0.044), longer hospitalization days (8 [6.5–12] vs 6 [5–7], P < 0.001), Lower oxygen saturation during hospitalization (94.4 [93–95] vs 96 [95–98], P < 0.001), higher prevalence of prior stroke (13 [21.3%]vs 1 [2.1%], P = 0.012), posterior circulation (23 [37.7%] vs 12 [25%], P = 0.014), and glucocorticoid use (8 [13.1%] vs 0, P = 0.025). In terms of laboratory indicators, the COVID-19 ALS group showed significantly higher values in LDH (254 [206–261] vs 187 [161–209], P < 0.001), INR (1.04 [0.98–1.1] vs 0.995 [0.95–1.06], P = 0.011), FIB (4.12 [3.42–5.11] vs 3.46 [2.83–4.05], P < 0.001), APTT ratio (1.06 [0.945–1.14] vs 0.94 [0.88–1.03], P < 0.001), D-dimer (0.88 [0.47–2.25] vs 0.41 [0.25–0.99], P < 0.001), CRP (31.67 [7.7–51] vs 3 [1.35–6.45], P < 0.001), and NT-proBNP (907 [200–932.63] vs 86.6 [46.43–353.4], P < 0.001), lower values in lymphocyte counts (0.95 [0.63–1.43] vs 1.55 [1.19–1.88], P < 0.001) and serum calcium (2.191 ± 0.097 vs 2.242 ± 0.086, P = 0.005) than the other group (Table 1). After 3-month follow-up, the COVID-19 ALS group had poorer recovery of neurological function (mRS ≥ 2) (42 (48.9%) vs 18 (37.5%), P = 0.002). Among the COVID-19 group, four patients died (non-COVID-19 was zero). Figure 2 details the distribution of 3-month mRS for the two groups. We presented a detailed analysis of the anticoagulant treatments, encompassing both oral and parenteral options, along with their respective dosages and durations of treatment in Table S2. We found there was no difference between COVID-19 and non-COVID-19 (all P > 0.05). Besides, overall 25 (Non-COVID-19 AIS n=10, COVID-19 AIS n=15) were receiving anticoagulation treatment, and 33 (Non-COVID-19 AIS n=10, COVID-19 AIS n=23) were receiving respiratory support. There was no difference in the anticoagulation treatment (Table S2) but a statistical difference in the respiratory support, and the latter suggested that people with COVID-19 had a worse respiratory function and needed more respiratory support (Table S3).
 |
Table 1 Baseline Characteristics of the Samples |
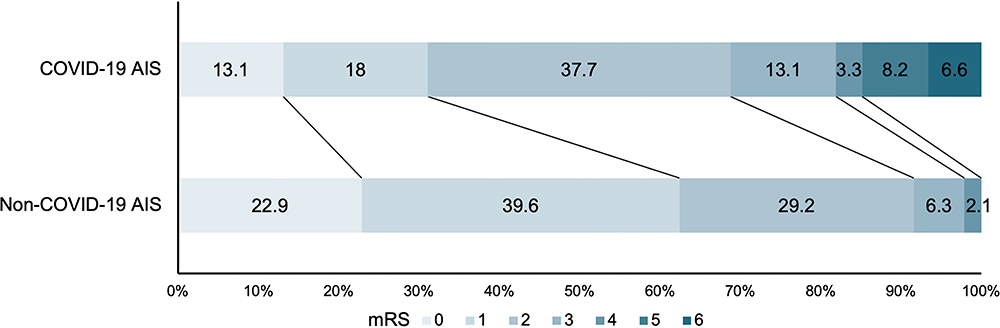 |
Figure 2 Distribution of 3-month mRS. Abbreviations: AIS, acute ischemic stroke; mRS, modified Rankin Scale. |
Baseline Characteristics of AIS with or Without Favorable Outcome
We analyzed the baseline characteristics between patients with favorable (mRS < 2) and unfavorable outcomes (mRS ≥ 2). The unfavorable outcome group was significantly associated with higher BMI (25.18 ± 3.15 vs 23.74 ± 3.05], P = 0.018), NIHSS scores at admission (4 [3–8] vs 3 [1.5–4], P = 0.003), longer hospitalization days (8 [6–12] vs 7 [5–8], P = 0.013), lower oxygen saturation (95 [93–96] vs 95 [95–98], P = 0.01), and higher prevalence of COVID-19 (42 [70%] vs 19 [38.8%], P = 0.002) when compared to the favorable outcome group. Unfavorable outcome patients had higher LDH (242.5 [197–260] vs 199 [163.5–234.5], P < 0.001), INR (1.05 [0.97–1.09] vs 1 [0.95–1.05], P = 0.005), D-dimer (0.85 [0.44–2.19] vs 0.44 [0.26–1.09], P < 0.001), CRP (12.5 [3.58–42.85] vs 4.9 [1.8–20.2], P = 0.012), NT-proBNP (440.5 [163–929.9] vs 126 [48.35–826], P < 0.001), and lower Lymphocyte counts (1.11 [0.71–1.52] vs 1.42 [1.04–1.93], P = 0.015), PLT (198.5 [160.8–228.8] vs 222 [183.5–267.5], P = 0.036) (Table 2). We also presented a detailed analysis of the anticoagulant treatments in Table S2. We found there was no difference between mRS<2 and mRS≥2 (all P > 0.05).
 |
Table 2 Baseline Characteristics of Patients with Different Outcomes |
Association Between COVID-19 and 3-Month mRS
Table 3 displays binary logistic regression results analyzing COVID-19 association with 3-month mRS. The prevalence of unfavorable outcomes was significantly higher in the ALS patients who had COVID-19 compared to those who did not have COVID-19 in an unadjusted model (OR: 3.68; 95% CI: 1.66–8.17, P = 0.001). In Model 1, after adjustment for age, gender, and BMI, COVID-19 was independently related to the prevalence of unfavorable outcomes (OR: 3.11; 95% CI: 1.35–7.18, P = 0.008). In Model 2, we added hypertension and diabetes as confounding factors, COVID-19 was still significant, with an odds ratio (OR) of 2.69 (95% CI: 1.13–6.40). When adding inflammatory indicators (lymphocyte absolute value and CRP), and coagulation indicators (INR and APTT ratio) as covariates (Model 3), the association became weak and insignificant (P = 0.294), which indicates the factors above potentially mediate the effect of COVID-19 on 3-month prognosis.
 |
Table 3 Binary Logistic Regression Analysis for the Association Between COVID-19 and 3-Month mRS |
Inflammation and Coagulation Mediating the Association of COVID-19 and 3-Month mRS
Binary logistic regression shows that the association between COVID-19 and unfavorable outcomes in 3 months may be mediated by inflammation factors (lymphocyte absolute value, CRP) and coagulation factors (INR, APTT ratio). To explore which factors were critical, we analyzed the mediation effect of lymphocyte absolute value, CRP, INR, and APTT ratio in the association between COVID-19 and 3-month mRS. The total effect (95% confidence interval) of COVID-19 to 3-month mRS was 0.604 (0.104, 1.104), P = 0.018. The indirect effect (Figure 3D) was significant [0.34 (0.115, 0.610)], suggesting that the APTT ratio specifically mediates the association between COVID-19 and 3 months outcome (accounting for 56.3% of the total effect) after adjustment for age, gender, BMI, NIHSS, hypertension, and diabetes. The mediation effects of other models (lymphocyte, CRP, and INR) were not significant (Figure 3). These results suggest that COVID-19 might have a specific impact on neurological outcomes through endogenous coagulation processes.
 |
Figure 3 The flow of mediating effect of laboratory indicators between COVID-19 and 3-month mRS. Abbreviations: mRS, modified Rankin Scale; CRP, C-reactive protein; INR, international normalized ratio; APTT, activated partial thromboplastin time; CI, Confidence interval. Notes: Indirect effect of lymphocyte absolute num (A), CRP (B), INR (C), APTT ratio (D) between COVID-19 and 3 months outcome. The total effect size of COVID-19 on 3-month mRS is 0.604, P = 0.018. Adjusting for age, gender, BMI, NIHSS, hypertension, and diabetes. a: the effect size of COVID-19 on laboratory indicators; b: the effect size of laboratory indicators on 3-month mRS; c’: the direct effect size of COVID-19 on 3-month mRS. |
Inflammation and coagulation might be interconnected to mediate the association between COVID-19 and 3-month mRS
Studies on COVID-19-associated coagulopathy suggest that when under high inflammatory conditions, locally activated platelets can induce the release of neutrophil extracellular traps, thereby activating endogenous and exogenous coagulation.9 CRP is an acute phase reactant and an inflammatory marker. To confirm the link between inflammation and coagulation in stroke people, we further performed an integrated mediation analysis to estimate the effect of the hypothesized path of COVID-19 infection→CRP↑→APTT ratio↑→3-month mRS↑ (Figure 4). After adjusting age, gender, BMI, NIHSS, hypertension, and diabetes, the path was significant [mediate effect (95% CI) = 0.113 (0.029, 0.270), percent mediation% = 18.7%, Table 4]. These results indicated that the high inflammation reactions triggered by COVID-19 could affect the prognosis of stroke through endogenous coagulation pathways.
 |
Table 4 Mediation Analysis for the Hypothesized Pathway from COVID-19 to 3-Month mRS |
 |
Figure 4 Mediation analysis for the hypothesized pathway from COVID-19 to 3-month mRS. Abbreviations: CRP, C-reactive protein; APTT, activated partial thromboplastin time; mRS, modified Rankin Scale. Notes: The total effect size of COVID-19 on 3-month mRS is 0.604, P = 0.018. Adjusting for age, gender, BMI, NIHSS, hypertension and diabetes. a1: the effect size of COVID-19 on CRP; a2: the effect size of COVID-19 on APTT ratio; a3: the effect size of CRP on APTT ratio; b1: the effect size of CRP on 3-month mRS; b2: the effect size of APTT ratio on 3-month mRS; c’: the direct effect size of COVID-19 on 3-month mRS. |
Discussion
This study is the first to explore the pathway mechanism between COVID-19 infection and stroke mid-term functional outcomes. Firstly, we found that stroke patients with COVID-19 had worse neurological functional outcomes 3 months after stroke. Secondly, we found that COVID-19 might affect the mid-term functional outcomes by specifically impacting the endogenous coagulation pathway. Thirdly, there might be complex interactions between inflammation and coagulation pathways after COVID-19 infection. The systemic inflammatory response triggered by COVID-19 might also contribute to poor outcomes by affecting the endogenous coagulation pathway.
Most of the existing studies suggest that COVID-19 patients with stroke have more severe neurological symptoms, longer hospitalization time, higher in-hospital mortality rates, and higher disability rates at discharge. In these studies, the research period was in an acute stroke phase.7,11,12 However, there is limited follow-up research on the outcomes, especially during the omicron period, and the pathway mechanism was scarce to explore. Research conducted before the omicron period suggests that among COVID-19 patients, the proportion of disabled individuals in the stroke population is higher compared to other neurological disorders at a 6-month prognosis.13 However, the time between COVID-19 and the onset of stroke is unclear. Another multicenter study found that COVID-19 patients with ischemic stroke have a higher mortality rate and fewer good functional outcomes at 3 months, and the COVID-19 patients in this study were in serious condition.14 These findings are similar to our conclusion. Differently, patients in our study were in the acute phase of COVID-19 infection and stroke, and the prevalent strain was omicron, which exhibited so milder COVID-19 symptoms that might easily be overlooked.
The spike protein of the COVID-19 virus triggers innate immune cells to express proinflammatory acute-response cytokines (tumor necrosis factor [TNF] and IL-1β) and chemotactic cytokines (IL-8 and monocyte chemoattractant protein-1 [MCP-1]) through TLR2-dependent activation of the NF-κB pathway, which promotes the continuous increase of IL-6 and triggers cytokine storm.7,15 Compared to patients with either COVID-19 or stroke alone, COVID-19 with ALS patients demonstrate excessive activation of systemic inflammation, suggesting a synergistic effect between COVID-19 infection and ischemic stroke.16
The activation of inflammation affects the coagulation function through the following five aspects. First, a large number of neutrophil extracellular traps (NETs) are formed. NETs are formed around active neutrophils, which can activate both intrinsic and extrinsic coagulation pathways through the expression of functional tissue factor (TF), capture platelets, and release of histones and DNA fragments.7,17 Second, cytokines play a role in this process. Cytokines IL-6 and CRP can trigger the expression of TF in monocytes. IL-6 can also stimulate the production of CRP, fibrinogen, and coagulation factors. TNF-a can promote the expression of TF in platelet and macrophage.9,18 Third, CRP, cytokines, complement, endothelial cells, and neutrophils activate platelets. Activated platelets release intracellular granule constituents and expose membrane phosphatidylserine which can promote the formation of thrombosis, triggering immune thrombosis formation.17 Fourth, inflammation stimulates endothelial cells to express procoagulant molecules, which puts the body in a hypercoagulable state. Fifth, the activation of complements promotes the release of procoagulant extracellular vesicles containing TF and other coagulation factors. C3a and C5a activate platelets and endothelial cells, and increase the expression of TF, von Willebrand factor (VWF).17,18 Thus, the activation of inflammation contributes to a hypercoagulable state.
Existing research suggests that the exogenous coagulation pathway is the dominant one in COVID-19-related coagulation disease, which is mainly driven by the expression of TF. A study has indicated that the increase of plasma kallikrein at least partially drives the hypercoagulable state in COVID-19, which means the endogenous coagulation pathway also plays an important role.19 In COVID-19-infected patients, the activation of the exogenous coagulation system is observed in the early stage, characterized by decreased prothrombin time (PT) and a hypercoagulable state. SARS-CoV2 infection induces hyperfibrinolysis, and the more severe the condition, the more severe the hyperfibrinolysis. With the progress of the disease, especially when patients develop disseminated intravascular coagulation (DIC), there is a significant prolong in PT and APTT, which is associated with poor outcomes. The prolongation of APTT is correlated with the mortality rate in COVID-19.20–23
The coagulation disorder after COVID-19 infection may impact the functional prognosis of stroke patients through the following three aspects. Firstly, during the initial stage of infection, patients are in a hypercoagulable state, which makes thrombosis extend.24 Additionally, the occurrence of VET events increases and impacts the recovery outcome of stroke patients. Secondly, due to the consumption and insufficient production of coagulation factors, activation of the anticoagulation system, production of antiphospholipid antibodies, and damage of endothelial cells, there is a prolongation of INR and APTT, indicating a risk of bleeding transformation, which worsens the severity of stroke and deteriorates functional outcomes.25–27 Thirdly, the activation of plasmin results in increased infectivity and virulence of the COVID-19 virus by facilitating virus entry into cells, leading to aggravating the COVID-19 infection.28,29
Limitation
This study has several limitations. First, we did not compare the COVID-19 infection with other pathogen infections (eg, bacterial pneumonia). It was also an important question that is the impact on the endogenous coagulation pathway specific to COVID-19 or just the general reaction of infection? Second, blood samples were only collected during hospitalization, and there was no data available during follow-up. Therefore, we cannot know the dynamic changes in coagulation function over time. Third, because the control group did not undergo nucleic acid testing, there may be asymptomatic COVID-19 patients. Fourth, this is a single-center study, and it needs to be further validated by a large multi-center sample. Fifth, although the study was conducted during the omicron variant pandemic, the COVID-19 virus strain could not be identified because it was not sequenced. Lastly, this is a preliminary, retrospective study, thus we can not make a causal inference. The mediation we identified should be further corroborated by longitudinal studies.
Conclusions
In summary, we found endogenous coagulation pathway mediate the association between COVID-19 and 3-month outcome after stroke during the Omicron wave. The systemic inflammatory response triggered by COVID-19 might also contribute to poor outcomes by affecting the endogenous coagulation pathway. The current study delineated a more accurate mechanism by which COVID-19 influences functional outcomes: COVID-19 infection→inflammation→endogenous coagulation pathway→ poor stroke outcome. Since anti-inflammation methods such as the cortisol hormones have side effects and might aggravate COVID-19 infection, we proposed the endogenous coagulation pathway might be the optimal target for stroke patients with COVID-19. This study found the specific pathway mechanism and provided new insights and ideas for secondary prevention for stroke patients with COVID-19 infection. Patients would benefit from the early use of tailored anti-coagulant strategies (targeting the endogenous coagulation pathway, which reduces the risk of bleeding complications).
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank each of the authors for their contributions to the article. We also thank all the patients who participated.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Tu WJ, Zhao ZP, Yin P, et al. Estimated Burden of Stroke in China in 2020. JAMA Network Open. 2023;6(3):15. doi:10.1001/jamanetworkopen.2023.1455
2. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics-2023 Update: a Report From the American Heart Association. Circulation. 2023;147(8):E93–E621. doi:10.1161/cir.0000000000001123
3. World Health Organization. WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. World Health Organization. WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. Available from: https://covid19.who.int/.
4. Chinese Center for Disease Control and Prevention. Epidemic situation of COVID-19 in China. Chinese Center for Disease Control and Prevention. Epidemic situation of COVID-19 in China. Available from: https://www.chinacdc.cn/.
5. Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–232. doi:10.1016/S0140-6736(20)32656-8
6. Rana R, Kant R, Huirem RS, Bohra D, Ganguly NK. Omicron variant: current insights and future directions. Microbiol Res. 2022;265:127204. doi:10.1016/j.micres.2022.127204
7. Sagris D, Papanikolaou A, Kvernland A, et al. COVID-19 and ischemic stroke. Eur J Neurol. 2021;28(11):3826–3836. doi:10.1111/ene.15008
8. Takacs TT, Berki AJ, Bojti PP, et al. The impact of SARS-CoV-2 infection on the outcome of acute ischemic stroke-A retrospective cohort study. PLoS One. 2023;18(3):e0282045. doi:10.1371/journal.pone.0282045
9. Gorog DA, Storey RF, Gurbel PA, et al. Current and novel biomarkers of thrombotic risk in COVID-19: a Consensus Statement from the International COVID-19 Thrombosis Biomarkers Colloquium. Nat Rev Cardiol. 2022;19(7):475–495. doi:10.1038/s41569-021-00665-7
10. Tripodi A, Lippi G, Plebani M. How to report results of prothrombin and activated partial thromboplastin times. Clin Chem Lab Med. 2016;54(2):215–222. doi:10.1515/cclm-2015-0657
11. Pezzini A, Grassi M, Silvestrelli G, et al. SARS-CoV-2 infection and acute ischemic stroke in Lombardy, Italy. J Neurol. 2022;269(1):1–11. doi:10.1007/s00415-021-10620-8
12. Akhtar N, Abid F, Singh R, et al. Ischemic stroke in patients that recover from COVID-19: comparisons to historical stroke prior to COVID-19 or stroke in patients with active COVID-19 infection. PLoS One. 2022;17(6):e0270413. doi:10.1371/journal.pone.0270413
13. Beretta S, Cristillo V, Camera G, et al. Incidence and Long-term Functional Outcome of Neurologic Disorders in Hospitalized Patients With COVID-19 Infected With Pre-Omicron Variants. Neurol. 2023;101(9):e892–e903. doi:10.1212/WNL.0000000000207534
14. Bhatia R, Padma Srivastava MV, Sylaja PN, et al. Clinical Features and Outcome of Stroke with COVID-19. COVID-19 Stroke Study Group (CSSG), India. Ann Indian Acad Neurol. 2021;24(5):668–685. doi:10.4103/aian.AIAN_122_21
15. Khan S, Shafiei MS, Longoria C, Schoggins JW, Savani RC, Zaki H. SARS-CoV-2 spike protein induces inflammation via TLR2-dependent activation of the NF-kappaB pathway. Elife. 2021;10. doi:10.7554/eLife.68563
16. Yao X, Liu S, Wang J, et al. The clinical characteristics and prognosis of COVID-19 patients with cerebral stroke: a retrospective study of 113 cases from one single-centre. Eur J Neurosci. 2021;53(4):1350–1361. doi:10.1111/ejn.15007
17. Conway EM, Mackman N, Warren RQ, et al. Understanding COVID-19-associated coagulopathy. Nat Rev Immunol. 2022;22(10):639–649. doi:10.1038/s41577-022-00762-9
18. Song Y, Fan H, Tang X, Luo Y, Liu P, Chen Y. The effects of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on ischemic stroke and the possible underlying mechanisms. Int J Neurosci. 2023;133(2):176–185. doi:10.1080/00207454.2021.1897588
19. Busch MH, Timmermans S, Nagy M, et al. Neutrophils and Contact Activation of Coagulation as Potential Drivers of COVID-19. Circulation. 2020;142(18):1787–1790. doi:10.1161/CIRCULATIONAHA.120.050656
20. Davidescu EI, Odajiu I, Tulba D, et al. Prognostic Factors in COVID-19 Patients With New Neurological Manifestations: a Retrospective Cohort Study in a Romanian Neurology Department. Front Aging Neurosci. 2021;13:645611. doi:10.3389/fnagi.2021.645611
21. Citu C, Burlea B, Gorun F, et al. Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: a Retrospective Observational Study in Romania. J Clin Med. 2022;11(10):2831. doi:10.3390/jcm11102831
22. Shang Y, Pan C, Yang X, et al. Management of critically ill patients with COVID-19 in ICU: statement from front-line intensive care experts in Wuhan, China. Ann Int Care. 2020;10(1):73. doi:10.1186/s13613-020-00689-1
23. El-Lateef AE A, Alghamdi S, Ebid G, Khalil K, Kabrah S, Abdel Ghafar MT. Coagulation Profile in COVID-19 Patients and its Relation to Disease Severity and Overall Survival: a Single-Center Study. Br J Biomed Sci. 2022;79:10098. doi:10.3389/bjbs.2022.10098
24. De Michele M, Lorenzano S, Piscopo P, et al. SARS-CoV-2 infection predicts larger infarct volume in patients with acute ischemic stroke. Front Cardiovasc Med. 2022;9:1097229. doi:10.3389/fcvm.2022.1097229
25. Bowles L, Platton S, Yartey N, et al. Lupus Anticoagulant and Abnormal Coagulation Tests in Patients with Covid-19. N Engl J Med. 2020;383(3):288–290. doi:10.1056/NEJMc2013656
26. Belen-Apak FB, Sarialioglu F. Pulmonary intravascular coagulation in COVID-19: possible pathogenesis and recommendations on anticoagulant/thrombolytic therapy. J Thromb Thrombolysis. 2020;50(2):278–280. doi:10.1007/s11239-020-02129-0
27. Wang R, Zeng J, Wang F, Zhuang X, Chen X, Miao J. Risk factors of hemorrhagic transformation after intravenous thrombolysis with rt-PA in acute cerebral infarction. QJM. 2019;112(5):323–326. doi:10.1093/qjmed/hcy292
28. Ji HL, Zhao R, Matalon S, Matthay MA. Elevated Plasmin(ogen) as a Common Risk Factor for COVID-19 Susceptibility. Physiol Rev. 2020;100(3):1065–1075. doi:10.1152/physrev.00013.2020
29. Fu Y, Xue H, Wang T, Ding Y, Cui Y, Nie H. Fibrinolytic system and COVID-19: from an innovative view of epithelial ion transport. Biomed Pharmacother. 2023;163:114863. doi:10.1016/j.biopha.2023.114863
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.