")
Back to Journals » Journal of Inflammation Research » Volume 17
The Predictive Value of Monocarboxylate Transporter 4 (MCT4) on Lung Adenocarcinoma Patients Treated with PD-1 Inhibitors
Authors Zhang Q , Pan G, Zhang L , Xu Y , Hao J
Received 29 August 2024
Accepted for publication 28 November 2024
Published 6 December 2024 Volume 2024:17 Pages 10515—10531
DOI https://doi.org/10.2147/JIR.S493632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Qinghua Zhang,1,* Guizhen Pan,2,* Lu Zhang,1 Yidan Xu,1 Jiqing Hao1
1Department of Oncology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui Province, People’s Republic of China; 2Department of Radiation Oncology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiqing Hao, Department of Oncology, The First Affiliated Hospital of Anhui Medical University, 218 Jixi Road, Hefei, 230022, People’s Republic of China, Tel +86 13965029739, Email [email protected]
Purpose: Monocarboxylate transporter 4 (MCT4) can influence the amount of lactate in the tumor microenvironment and further control cancer cell proliferation, migration, and angiogenesis. This study aimed to evaluate the predictive value of MCT4 for prognosis and immunotherapy efficacy in advanced lung adenocarcinoma (LUAD).
Patients and methods: First, bioinformatics analysis was used to assess the relevance of MCT4 for survival and immunotherapy outcomes in LUAD. Subsequently, we performed a retrospective study involving 126 patients with stage IIIb to IV LUAD treated with programmed death-1 (PD-1)/programmed death-ligand 1 (PD-L1) inhibitors. MCT4 expression in LUAD tissues was detected by immunohistochemistry (IHC), then the patients were divided into high and low expression groups. The differences in the medical records of the two groups were compared using the X2 test. Kaplan-Meier (K-M) method was used for survival analysis. Univariate and multivariate analysis were used to pinpoint independent predictors, and a nomogram was developed based on the significant factors for overall survival (OS) in the multivariate analysis. The predictive ability of the nomogram was evaluated through C-index, receiver operating characteristic (ROC) curve, calibration curve, and decision curve analysis (DCA).
Results: Both bioinformatics analysis and clinical study revealed that low MCT4 expression was associated with better prognosis and immunotherapy efficacy. Multivariate analysis of clinical characteristics showed that age > 65 years, stage IV, high MCT4 expression, neutrophil-to-lymphocyte ratio (NLR)> 3, lactate dehydrogenase (LDH)> 250 (U/L) and carcinoembryonic antigen (CEA)> 5 (ng/mL) were significantly associated with poor prognosis on immunotherapy. These factors were subsequently incorporated into the nomogram model. The C-index value of the model stood at 0.735 (95% CI= 0.662 ~ 0.807), indicating robust predictive performance of the model. The DCA curve showed that the model had a notable clinical application value.
Conclusion: High expression of MCT4 is associated with poor prognosis and reduced efficacy of immunotherapy in patients with advanced LUAD.
Keywords: lung adenocarcinoma, monocarboxylate transporter 4, immunotherapy efficacy, prognosis, nomogram
Introduction
With nearly 2.5 million new cases and over 1.8 million deaths worldwide, lung cancer was the leading cause of cancer morbidity and mortality in 2022. Among non-small cell lung cancer (NSCLC) subtypes, lung adenocarcinoma (LUAD) stands out as the most prevalent, contributing significantly to cancer-related mortality.1,2 Traditional treatments for LUAD include surgery, radiotherapy, chemotherapy, and targeted therapy. However, their efficacy in advanced cases is often restricted. Recently, immune checkpoint inhibitors, specifically targeting programmed death-1 (PD-1) and programmed death-ligand 1 (PD-L1), have emerged as a promising approach. These inhibitors have demonstrated notable effectiveness, prolonging survival and enhancing quality of life for certain LUAD patients.3 However, there are notable inter-individual variations in patient with LUAD responses to immunotherapy, which may be attributed to a multitude of factors, including the genetic characteristics of the tumor, the tumor microenvironment and the patient’s immune status.4,5 Hence, there is a pressing need to develop an accurate and personalized prognostic model to predict patient with LUAD responses to immunotherapy and guide treatment decisions.
Tumor cells are recognized for inducing an immunosuppressive microenvironment through metabolic reprogramming, wherein lactate, a byproduct of glycolysis, plays a crucial role.6–9 The monocarboxylic acid transporter (MCT) family of proteins is responsible for the transport of lactate and other metabolic monocarboxylic acids. The MCT family facilitates the transport of lactate and other metabolic monocarboxylic acids. Specifically, monocarboxylate transporter 4 (MCT4) plays a crucial role in mediating the cellular efflux of lactate and H+. Overexpression of MCT4 has been associated with unfavorable outcomes in patients with a variety of tumors, including breast cancer, hepatocellular carcinoma and melanoma, suggesting that it is a promising biomarker for predicting cancer prognosis.10–13 To date, studies on MCT4 in LUAD have primarily focused on its transcriptomic profile and the metabolic level.10,14–16 However, there is a lack of systematic studies of its potential value for clinical applications to comprehensively assess the potential value of MCT4 in predicting response to immunotherapy in patients with LUAD.
Several routine laboratory parameters have been shown to correlate with an adverse prognosis in cancer patients.17–21 These parameters include blood counts, neutrophil-to-lymphocyte ratio (NLR) and derived neutrophil-lymphocyte ratio (dNLR), lactate dehydrogenase (LDH), tumor biomarkers. Furthermore, these laboratory tests are not only readily available, but are also routinely performed during each cycle of PD-1/PD-L1 inhibitors therapy to facilitate continuous monitoring of the patient’s status. Thus, there is increasing research interest in integrating these routine laboratory parameters with prognostic gene expression to improve predictive accuracy beyond the use of prognostic genes alone. In this study, our objective is to develop a predictive model for assessing prognosis and immunotherapy efficacy by integrating MCT4 expression with clinical features and routine laboratory parameters.
Materials and Methods
Bioinformatics Analysis
To facilitate a comprehensive understanding of MCT4 expression, we analyzed pan-cancer expression data from The Cancer Genome Atlas (TCGA) and plotted the expression pattern of MCT4 across various malignancies.22,23 Using the “TCGAplot” R package, we explored the correlation between MCT4 and somatic mutations in different cancer types.24 To investigate the prognostic role of MCT4 in LUAD, we conducted Kaplan–Meier and Cox regression analyses to determine its impact on overall survival. Additionally, ROC analysis was used to further evaluate its predictive performance. Immune cell infiltration was calculated for each individual based on seven currently popular algorithms (XCELL, TIMER, QUANTISEQ, MCPCOUNTER, EPIC, CIBERSORT-ABS, CIBERSORT).25,26 Then we analyze the influence of MCT4 expression on the infiltration of immune cells in LUAD. Furthermore, we calculated the scores of stromal and immune cells using the ESTIMATE algorithm. To investigate the effect of MCT4 expression on immunotherapy efficacy, we examined the association between MCT4 and immune checkpoint gene expression using the Pearson method and evaluated the influence of MCT4 expression on the immunophenotype scores (IPS) of patients with LUAD through the Cancer Immunome Atlas (TCIA) database.27
Cell Lines and Cell Culture
Human lung cancer cell lines A549, NCI-H522, NCI-H23, and normal lung cells BEAS-2B were originally purchased from the cell bank of the Chinese Academy of Sciences (Shanghai, China) and provided by the Department of Hepatobiliary Surgery, The First Affiliated Hospital of Anhui Medical University. The use of the cell lines was approved by the Medical Ethics Committee of the First Affiliated Hospital of Anhui Medical University (approval number: 2023494). All cells were cultured in RPMI-1640 medium (Gibco) supplemented with 10% fetal bovine serum (FBS, Gibco, USA). The cell cultivation conditions were 37°C with 5% CO2.
Study Population
This study retrospectively analyzed patients with stage IIIb to IV LUAD who were treated with PD-1/PD-L1 inhibitors at the First Affiliated Hospital of Anhui Medical University from January 2020 to February 2024. Inclusion criteria were as follows: (1) individuals aged 18 years or older; (2) patients with confirmed LUAD willing to provide tumor tissue for immunohistochemical examination; (3) patients with clinical stage IIIb to IV; (4) patients receiving monotherapy or combination therapy with a PD-1/PD-L1 inhibitor; (5) patients with a life expectancy greater than 3 months; (6) patients meeting the Response Evaluation Criteria In Solid Tumors 1.1 (RECIST 1.1), with at least one measurable or evaluable target lesion by CT or MRI; (7) Eastern Cooperative Oncology Group (ECOG) physical status score ≤2; (8) patients capable of complying with the study protocol and follow-up. Exclusion criteria were as follows: (1) history of other primary malignancies; (2) receipt of radiotherapy or surgical oncology within four weeks prior to immunotherapy; (3) fewer than two courses of treatment with a PD-1/PD-L1 inhibitors; (4) conditions that may compromise the safety of study treatment or compliance, such as psychiatric disorders, blood disorders, immune disorders, etc.; (5) incomplete clinical data or absence of essential information. Informed consent was obtained from all patients or their families, and this study was approved by the Ethics Review Committee of the First Affiliated Hospital of Anhui Medical University [Reference number: Quick-PJ 2023–05-62].
Data Collection
In retrospective study, the baseline clinical characteristics of 126 patients with LUAD were collected, including sex, age, clinical stage, lymphatic metastasis status, treatment regimens and smoking history. Serological index test results were obtained within 2 weeks before receiving antitumor therapy, including white blood cell count (WBC), neutrophil count (N), lymphocyte count (L), LDH, carcinoembryonic antigen (CEA), cytokeratin 19 fragment (CYFRA 21–1), and neuron-specific enolase (NSE). The calculation formulas were as follows: NLR = N/L; dNLR = N/(WBC-N). The cut-off values for both NLR and dNLR were defined as greater than 3, consistent with existing literature.18,28 The normal ranges of CEA, NSE, and CYFRA21-1 were 0–5 ng/mL, 0–15 ng/mL, and 0–4 ng/mL, respectively, with an upper limit of normal (ULN) set at 250 U/L for LDH. All patients were divided into high- and low-level groups based on whether they were above or below the upper limit of normal as determined by the institutional laboratory.
Immunohistochemistry
Paraffin-embedded samples of LUAD and paracancerous tissues were sectioned at 4-μm thickness and baked at 60°C for 40 minutes. Sections were then deparaffinized in xylene and dehydrated through an ethanol gradient. Antigen retrieval was performed by boiling the samples in ethylenediaminetetraacetic acid (EDTA) buffer (pH 9.0) in a microwave for 15 minutes. Immunohistochemical staining utilized the streptavidin-peroxidase (SP) method, with initial blocking of endogenous peroxidase activity using 3% hydrogen peroxide. Sections were subsequently incubated overnight at 4°C with a primary antibody against MCT4 (rabbit anti-MCT4 polyclonal antibody, 22787-1-AP, diluted 1:800, Proteintech). The next day, sections were incubated with a horseradish peroxidase-conjugated secondary antibody (GB23302, diluted 1:200, Servicebio) for 50 minutes at room temperature. After treatment with 3,3’-diaminobenzidine tetrahydrochloride (DAB) for 5 minutes, sections were counterstained with hematoxylin, dehydrated through an ethanol gradient, and mounted with neutral gum. Staining results were observed using a white light microscope, where hematoxylin-stained nuclei appeared blue, and positive DAB staining appeared yellow.
Western Blot
Samples were extracted using RIPA buffer (Beyotime, Shanghai, China). Subsequently, the proteins were combined with SDS-PAGE loading buffer (Invitrogen) and heated to 85 °C for 5 minutes. Equal amounts of cell lysates were resolved by SDS-polyacrylamide gel electrophoresis (PAGE) and transferred on a polyvinylidene difluoride (PVDF) membrane (Millipore, Bed-ford, MA, USA) followed by incubating with primary antibodies against MCT4 (rabbit anti-MCT4 polyclonal antibody, 22787-1-AP, diluted 1:800, Proteintech), as well as anti-rabbit secondary antibodies (1:3000; SA00001-4; Proteintech). The results were captured using a CLiNX ChemiScope 5000 imaging system.
Semi-Quantitative Method
The expression levels of MCT4 protein in LUAD samples were assessed through semi-quantitative immunohistochemical (IHC) analysis based on staining intensity and the percentage of positively stained cells. Two independent investigators evaluated staining intensity on a scale of 0–3 (0 = no staining, 1 = weak, 2 = moderate, 3 = strong). The percentage of positive cells was calculated using Image J software and categorized as follows: 0 for <5%, 1 for 5–25%, 2 for 26–50%, 3 for 51–75%, and 4 for >75%. The staining intensity score was multiplied by the percentage score to determine MCT4 expression level. Scores of 0–4 indicated low expression, while >4 indicated high expression.20,29,30 This scoring system was developed to establish a standardized and reproducible method for evaluating MCT4 protein expression.
Follow-Up
Patients’ survival was monitored through inpatient, outpatient, and telephone follow-ups until death from any cause or the study cut-off date (May 31, 2024). Enrolled patients received PD-1/PD-L1 inhibitors in 21-day treatment cycles and target tumor lesions were imaged after 2 cycles. Tumor response was assessed according to the Immunotherapy Response Evaluation Criteria In Solid Tumors (iRECIST), categorizing responses as progressive disease (PD), stable disease (SD), partial remission (PR), and complete remission (CR).31 The primary endpoint was overall survival (OS), with secondary endpoints including progression-free survival (PFS) and disease control rate (DCR). OS was defined as the time from the start of first-line immunotherapy to death from any cause or loss to follow-up. PFS was defined as the time from the start of first-line immunotherapy to tumor progression, death from any cause, or loss to follow-up. DCR was calculated as the sum of CR, PR, and SD cases divided by the total number of patients. The objective response rate (ORR) was calculated as the sum of CR and PR divided by the total number of patients.
Statistical Analysis
IBM SPSS Statistics (version 27.0) and R software (4.4.0) were used for data analysis and graphing. Categorical variables were represented by cases and ratios and compared by chi-square or Fisher’s exact test. Serial numbers with non-normal distribution were expressed as median with interquartile range. To reduce biases inherent to retrospective studies, double data entry was independently validated, strict inclusion and exclusion criteria were applied, and outcomes were assessed by blinded investigators. Missing data were handled using multiple imputation with the “mice” package. For survival analyses, the Kaplan-Meier method (K-M) was employed. The methodology employed for estimating survival functions and for comparing differences in survival curves between groups was the log-rank method. Univariate and multivariate analysis were used to pinpoint independent predictors, and a nomogram was developed based on the results of the overall survival (OS) multivariate Cox model. The model was evaluated through C-index, receiver operating characteristic (ROC) curve, calibration curve, and decision curve analysis (DCA). No multiple testing corrections were applied, as the study focused on model development and exploratory hypothesis generation rather than formal hypothesis testing. A P-value <0.05 indicated that the difference was statistically significant.
Results
Correlation of MCT4 to Survival and Immunotherapy Efficiency Based on Transcriptome Data
Firstly, we utilized The Cancer Genome Atlas (TCGA) project to analyze the expression status of MCT4 in various cancers. As shown in Figure 1A, MCT4 expression was dysregulated in most tumors, with elevated expression in many types of cancers except Kidney Renal Cell Carcinoma (KICH) and primary cardiac tumor (PRCAD). We then compared the MCT4 expression levels with tumor mutational burden (TMB) and microsatellite instability (MSI) across various cancers. The results illustrated that MCT4 expression was linked to TMB and MSI in 8 and 6 cancer types, respectively (Figure 1B).
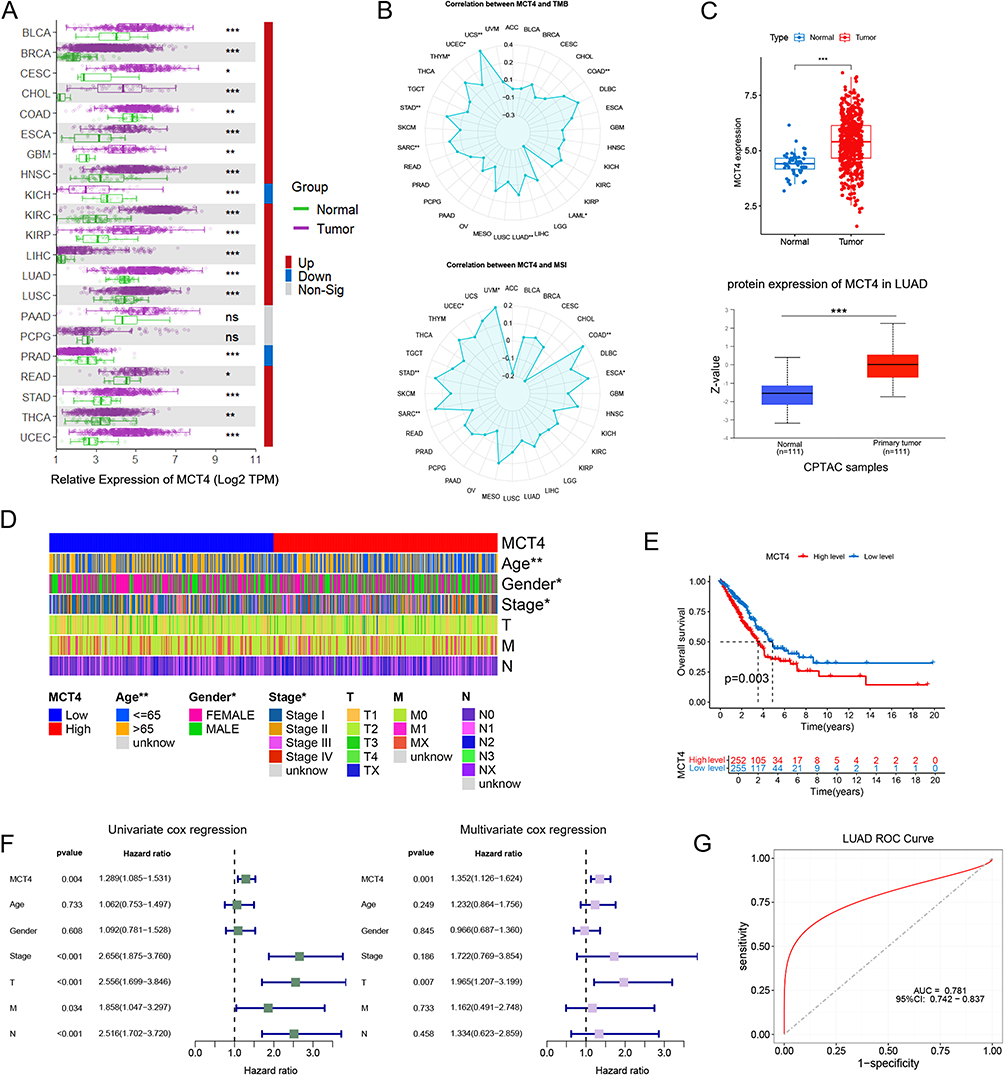 |
Figure 1 The expression level of monocarboxylate transporter 4 (MCT4) and its prognostic predictive performance. (A) MCT4 expression levels in 21 pan-cancer samples compared to corresponding paracancerous samples; (B) Correlation of MCT4 expression with tumor mutational burden (TMB) and microsatellite instability (MIS) across 33 pan-cancers; (C) Comparison of MCT4 RNA and protein levels in lung adenocarcinoma (LUAD) samples versus corresponding paracancerous samples; (D) Association analysis of MCT4 expression with clinical features; (E) Kaplan-Meier curve comparing low- and high-expression groups of MCT4; (F) Results of univariate and multivariate Cox regression analyses examining MCT4 expression and clinical features; (G) Receiver operating characteristic (ROC) curve evaluating the diagnostic performance of MCT4 expression for LUAD in The Cancer Genome Atlas (TCGA) cohort. Notes: ns as no significance, * as p <0.05, ** as p <0.01, *** as p <0.001. |
Subsequently, we comprehensively investigated the potential role of MCT4 in LUAD. Our further expression analysis showed that at both mRNA and protein levels, MCT4 was abnormally up-regulated in LUAD tissues compared to corresponding paracancerous tissues (Figure 1C). Moreover, MCT4 expression was associated with age, gender, and stage in patients with LUAD (Figure 1D). We then investigated its prognostic value using Kaplan–Meier and Cox analyses. The results of the survival analysis demonstrated that increased expression of MCT4 was linked to poor overall survival (Figure 1E and F). Additionally, ROC analysis showed strong performance for MCT4 to discriminate between patients with and without LUAD (Figure 1G).
To understand the impact of MCT4 on the tumor immune microenvironment, we estimated the infiltration of immune cells and the tumor microenvironment (TME) score in LUAD. As shown in Figure 2A, MCT4 expression levels were positively related to CD4+ T cells and macrophage M1, while negatively related to CD8+ T cells, B cells, and macrophage M2. Furthermore, patients with lower MCT4 levels had higher TME scores (Figure 2B). These findings indicate the important role of MCT4 in the tumor immune microenvironment. Finally, to investigate the potential role of MCT4 in immunotherapy efficacy, we analyzed the association of MCT4 with immune checkpoint genes. Our data showed a positive relationship between MCT4 and the expression of most immune checkpoint genes except CD40LG and TNFSF15 (Figure 2C). The subsequent IPS estimation revealed that in four patient cohorts (CTLA4-/PD1-, CTLA4+/PD1-, CTLA4-/PD1+, CTLA4+/PD1+), those with high MCT4 expression displayed a poor response to immunotherapy (Figure 2D).
 |
Figure 2 The correlation of MCT4 with the immune microenvironment landscape and immunotherapy response; (A) Bubble map showing the correlation of MCT4 expression with various immune cell types; (B) Tumor microenvironment (TME) scores (including stromal score, immune score, and ESTIMATE score) in MCT4 low- and high-expression groups; (C) Heat map depicting the correlation between MCT4 expression and immune checkpoint gene expression; (D) Immunophenotype scores (IPS) comparison between MCT4 low and high expression groups across four indicated patient categories. Notes: *** as p <0.001. |
The Correlation of MCT4 Expression and Clinical Variables
To further investigate the potential predictive value of MCT4 for prognosis and immune efficacy in LUAD, we subsequently conducted a retrospective study. We initially conducted IHC assay to verify the MCT4 expression in LUAD and paracancerous tissues. The results depicted in Figure 3A, MCT4 protein showed significant positive staining in the cytomembrane and cytoplasm of tumor cells. MCT4 was found to be highly expressed in NSCLC tissues and paracancerous tissues at a rate of 63.49% (80/126) and 20.00% (2/10), respectively. Consistently, our western blot assay revealed the upregulated levels of MCT4 in lung cancer cell lines (including A549, NCI-H522, NCI-H23) compared to BEAS-2B, a bronchial epithelial cell lines (Figure 3B). Based on the expression of MCT4 protein in LUAD tissues, all patients were divided into high and low expression groups. As shown in Table 1, our data indicated correlations between MCT4 expression levels and lymph node metastasis (χ²=5.38, P=0.020), clinical stage (χ²=5.48, P=0.019), and LDH (χ²=8.07, P=0.005) in patients with LUAD. In addition, MCT4 expression was significantly correlated with the efficacy of immunotherapy (χ²=10.00, P=0.007). While MCT4 expression did not correlate significantly with ORR (χ²=0.07, P=0.786), it showed a significant correlation with DCR (χ²=9.42, P=0.002). These findings suggest that MCT4 may serve as a potential biomarker for predicting the efficacy of immunotherapy and prognosis in patients with advanced LUAD.
 |
Table 1 The Distribution of Clinical Variables Between the MCT4 high-Expression and Low-Expression Groups |
 |
Figure 3 (A) Representative immunohistochemistry images showing the expression of MCT4 protein in paracancerous and tumor tissues. The magnification of the image is x200, and the scale bars are 0.100 mm; (B) MCT4 protein expression in BEAS-2B normal lung cell and three lung cancer cell lines (A549, NCI-H522, NCI-H23) by Western blot analysis; (C and D) Kaplan-Meier analysis of indicated factors with significant univariate Cox regression in progression free survival (PFS) (B) or overall survival (OS) (C). |
Impact of Clinicopathological Features on DCR
The significant correlation between MCT4 expression and DCR above inspired us to further investigate whether MCT4 could serve as a biomarker to predict the efficacy of immunotherapy in LUAD. To test this hypothesis, we first performed a univariate logistic regression analysis of the above variables. The results revealed that MCT4 expression, LDH, CEA and CYFRA 21–1 were all significantly associated with DCR. Then, the multivariate logistic regression analysis showed that MCT4 expression and CEA were independent risk factors for DCR. And the patients with high MCT4 levels were more likely to have poorer disease control than those with low MCT4 levels (HR = 9.01, 95% CI = 1.11 ~ 72.80, P =0.039) (Table 2).
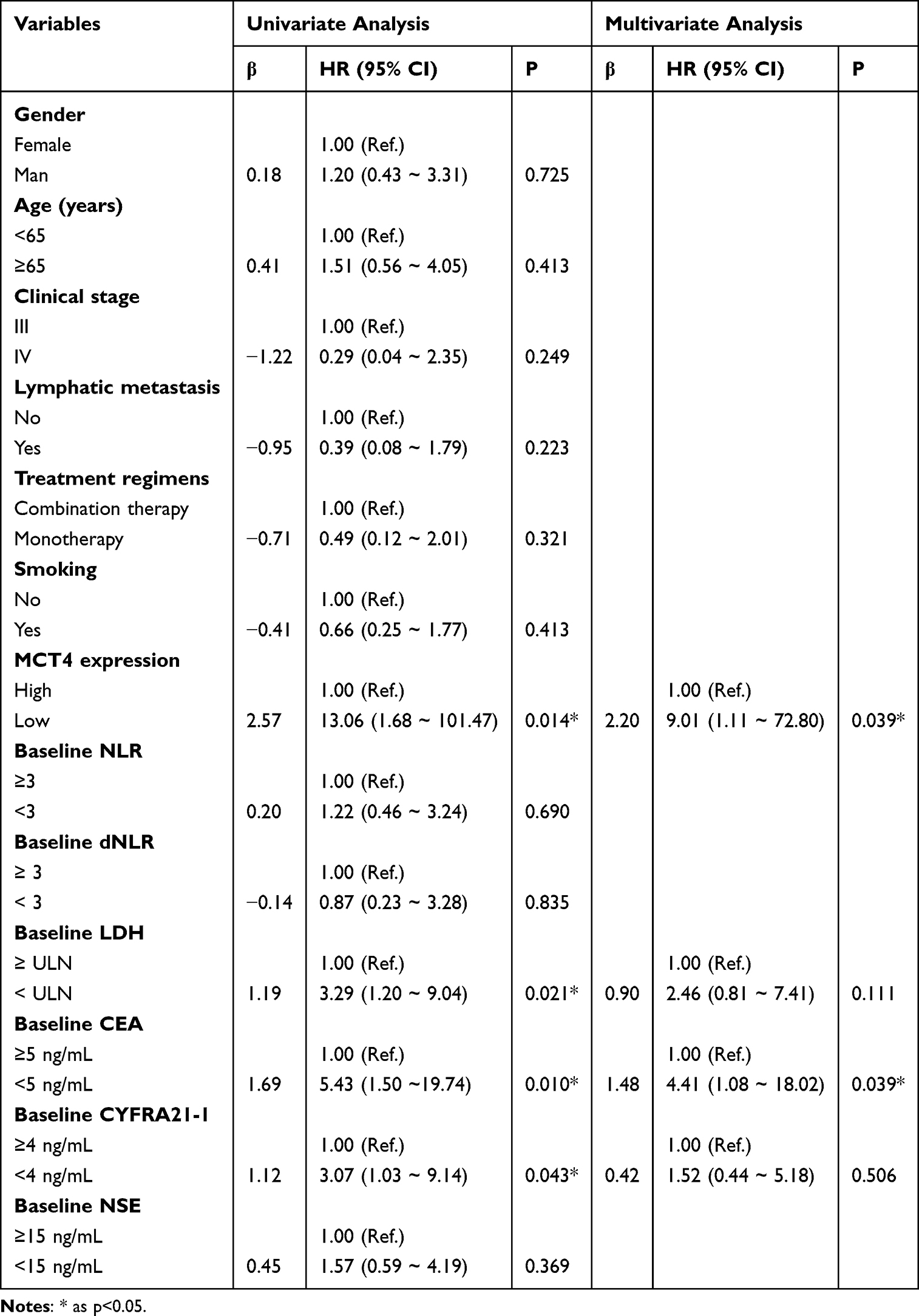 |
Table 2 Univariate and Multivariate Logistic Regression Analysis for DCR |
Influence of Clinicopathological Features on PFS
The overall mean follow-up period in this study was 24.43 (95% CI = 22.37 ~ 26.48) months, and 65 patients died during the follow-up period. The median PFS and OS periods of all patients were 11.00 (95% CI = 7.19 ~ 14.81) and 22.00 (95% CI =19.19 ~ 24.81) months, respectively.
Similarly, we performed univariate Cox regression analysis of the association of MCT4 expression and clinical features with PFS. Univariate Cox regression analysis showed that MCT4 expression, clinical stage, LDH, and CYFRA21-1 were significantly associated with PFS. Then the multivariate Cox regression analysis found that MCT4 expression, LDH and CEA remained significant on multivariate analysis. And the patients with high MCT4 levels were 0.94 times more likely to experience disease progression than those with low MCT4 levels (HR = 0.39, 95% CI = 0.23 ~ 0.66, P < 0.001) (Table 3).
 |
Table 3 Univariate and Multivariate Cox Regression Analysis for PFS |
Kaplan-Meier analysis demonstrated a significantly higher PFS rate in patients with low MCT4 expression compared to those with high MCT4 expression (P<0.001). Similar results were observed in the low LDH (P = 0.001), low CEA (P = 0.007), and low CYFRA21-1 (P = 0.006) groups compared to their respective high expression groups (Figure 3C).
Effect of Clinicopathological Features on OS
Also, given the significant correlation between MCT4 expression and the clinical stage of LUAD patients, we further investigated whether MCT4 protein could serve as a predictor of LUAD prognosis. To this end, we first performed univariate Cox regression analysis to assess the association of MCT4 expression and other clinicopathological characteristics with OS. The univariate Cox regression analysis showed that age, clinical stage, MCT4 expression, NLR, LDH and CEA were associated with OS. Then the multivariate Cox regression analysis confirmed that that age, clinical stage, MCT4 expression, NLR, LDH and CEA were independent risk factors for OS. And the patients with high MCT4 levels were 0.85 times more likely to experience disease-related death than those with low MCT4 levels (HR = 0.43, 95% CI = 0.23 ~ 0.78, P = 0.006) (Table 4).
 |
Table 4 Univariate and Multivariate Cox Regression Analysis for OS |
Kaplan-Meier analysis revealed a significantly higher OS rate in patients with low MCT4 expression compared to those with high MCT4 expression (P<0.001). The results were similar in the high NLR, high LDH and high CEA groups compared to the low NLR (P=0.035), low LDH (P=0.005) and low CEA groups(P=0.012) (Figure 3D).
Nomogram Development and Model Validation
We constructed a nomogram model using the 6 independent risk factors (age >65 years, stage IV, high MCT4 expression, NLR>3, LDH>250 U/L, and CEA>5 ng/mL) based on univariate and multivariate Cox regression analyses (Figure 4A).
 |
Figure 4 Construction and verification of nomogram for predicting prognosis. (A) Prognostic nomogram to estimate their probability of survival at 1-year and 2-year; (B) The C-index for the established model was 0.735 (95% CI=0.662 ~ 0.807); (C) The ROC curve of 1-year and 2-year OS; (D) The calibration curve of nomogram for 1-year and 2-year OS (bootstrap 1000 repetitions); (E) The decision curves analysis of nomogram for 1-year and 2-year OS. |
In the OS model, the C-index value was 0.735 (95% CI=0.662 ~ 0.807) (Figure 4B), and the area under the ROC curve (AUC) of the one-year and two-year for predicting OS were 0.757 (95% CI=0.652 ~ 0.861) and 0.841 (95% CI=0.750 ~ 0.932) (Figure 4C), respectively. Furthermore, the calibration curves of the nomogram showed a high degree of agreement between predicted and observed survival probabilities (Figure 4D), and DCA analysis showed that nomogram has great potential for clinical decision making (Figure 4E).
The risk score for individual patient was calculated based on the nomogram. Patients were then divided into high-risk or low-risk group according to the median risk score.32,33 Kaplan-Meier OS curves demonstrated that the high-risk group of patients has poor survival overall compared to that in low-risk group (P < 0.001) (Figure 3D). These results show that patients with a higher risk score tend to have a worse prognosis. Our findings have important implications for clinical treatment decisions, supporting the use of a nomogram to stratify patients by risk, guiding the selection of treatment strategies and promoting personalized, precision medicine.
Discussion
The MCT4 protein is predominantly expressed on the plasma membrane of cells and functions as a principal transporter of lactate, playing a pivotal role in lactate metabolism.12,16 The findings indicated that the expression of MCT4 protein in LUAD tissues and lung cancer cells was higher than that in paracancerous tissues and normal lung cells. Furthermore, it correlated with the clinical stage and lymph node metastasis, suggesting that MCT4 may be implicated in the development and progression of LUAD. Further multivariate regression analysis demonstrated that high MCT4 expression was associated with poorer PFS and OS, indicating that MCT4 expression level has significant prognostic value in LUAD patients treated with PD-1/PD-L1 inhibitors. Additionally, a nomogram based on MCT4 and clinicopathological parameters was successfully developed and validated for predicting the prognosis of LUAD patients.
More and more evidences demonstrated that MCT4 is highly expressed in a range of tumors, including breast cancer, hepatocellular carcinoma and melanoma. Consequently, it is regarded as a promising biomarker for predicting cancer prognosis.12 Notably, Tao et al observed a significant elevation in MCT4 expression in LUAD relative to normal tissue, which was markedly correlated with a poor prognosis.34 These findings corroborate the conclusions drawn from this study: elevated expression of the MCT4 protein is linked to the malignant biological behaviors and unfavorable prognosis in LUAD.
Lactate, a glycolysis byproduct, plays a crucial role in inducing an immunosuppressive microenvironment in tumor cells.6,7 MCT4, a key protein mediating cellular efflux of lactate and H+, potentially influences the tumor-induced immunosuppressive microenvironment.11 This study analyzed the association between MCT4 expression, immune microenvironment, and immunotherapy efficacy using TCGA-LUAD RNAseq data. Results indicate that MCT4 correlates with a tumor-promoting immune microenvironment and is significantly associated with poor immunotherapy efficacy. Furthermore, in our retrospective study cohort, MCT4 emerged as an independent prognostic factor for DCR in patients with LUAD, highlighting its predictive value in assessing immunotherapy efficiency.
NLR serves as a critical biomarker, indicating systemic inflammatory responses, with elevated levels commonly linked to adverse cancer outcomes.35,36 Such increases in NLR may serve as a reflection of the inflammatory environment within the tumor microenvironment, thereby suggesting a potential correlation with tumor invasiveness and metastatic capabilities. In addition to its function as an indicator of tumor burden, serum LDH has been identified as a multifaceted biomarker with a complex relationship to the activation of oncogenic signaling pathways and the metabolic, invasive, and immunogenic properties of numerous cancers. This makes it an attractive target for therapeutic intervention.21,37 CEA is a well-known tumor marker with broad-spectrum capabilities. It is elevated in a number of cancers, including colorectal, gastric, lung, and breast. Its elevation is associated with the presence, progression, and relapse of the disease in these cases. Furthermore, it can be employed for the monitoring of treatment responses and the assessment of prognosis.38,39 Our research substantiates that lower baseline levels of NLR, LDH, and CEA are correlated with superior responses to immunotherapy and enhanced clinical prognoses.
This research demonstrates a correlation between MCT4 and LDH in LUAD, indicating that they have a synergistic function within the tumor’s metabolic pathways. MCT4, which functions as a lactate transporter, facilitates the efflux of lactate from the cell, while LDH plays a pivotal role in the generation of lactate. This synergism may enable tumor cells to evade immune detection and promote tumor growth.16,40 A comprehensive understanding of the mechanisms underlying the roles of MCT4 and LDH in LUAD is crucial for the development of novel therapeutic strategies. Furthermore, the investigation of dual-target therapies for MCT4 and LDH offers promising prospects for the introduction of new treatment options for patients with LUAD.
The area under the ROC curve (AUC) is a key metric for assessing the accuracy of a model in predicting patient prognosis.41 We integrated all the essential information of a series of prognostic models in lung cancer, including author, year, and model characteristics, and the constructed AUC to verify the diagnostic performance of the model. After comparison, we found that the AUC of our model was 0.757 and 0.841 at 1 and 2 years, respectively, which was significantly than most predictive models (Table 5).42–46
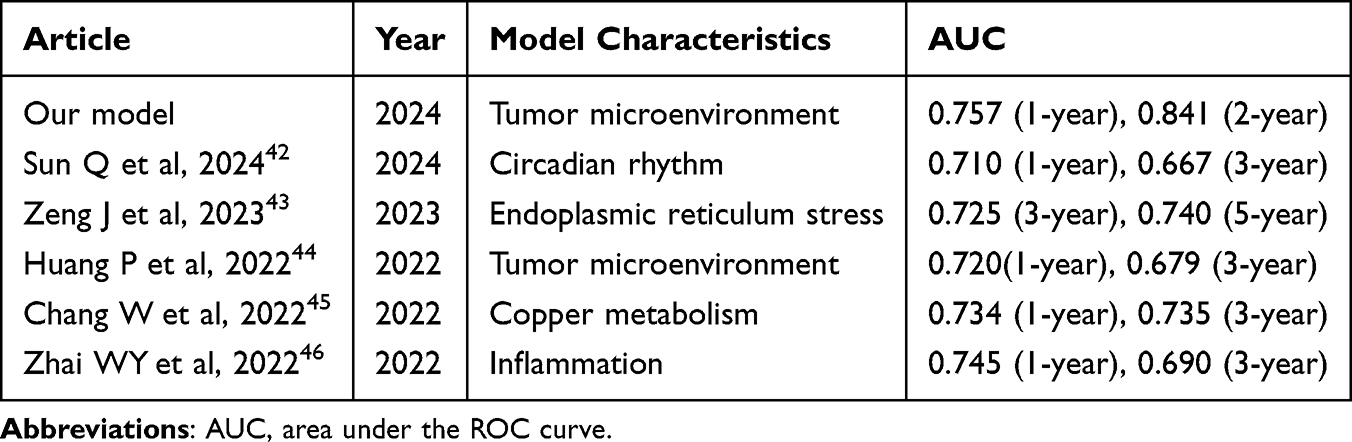 |
Table 5 Comparative AUC Analysis of Prognostic Models in Lung Cancer |
In our study, the model we constructed can be considered a suitable prognostic signal and its mechanism of action in lung cancer deserves further investigation and verification. MCT4 levels are determined using the widely accepted IHC scoring system, which ensures standardized and reproducible results. The blood test indicators included in our model are routine and easily accessible, enhancing the practicality of the model. Overall, the improved predictive performance and clinical applicability of our model will enable more accurate prognostic assessments and personalized treatment strategies, ultimately leading to better patient outcomes.
It should be acknowledged that this study has certain limitations. Firstly, as a retrospective study, it is subject to inherent bias, and some patients did not reach the pre-specified endpoints, necessitating extended follow-up. Additionally, the study sample lacks diversity in ethnicity, geographical representation, and clinical stages. Expanding the sample in future study to include a broader patient population through multicenter studies and additional validation cohorts could help address these limitations.
Conclusion
This study is one of the few that analyzed the correlation between MCT4 expression and prognosis in LUAD patients treated with PD-1/PD-L1 inhibitors. The study found that the expression level of MCT4 of patients was negatively correlated with DCR, PFS and OS. In addition, this study also demonstrated for the first time that the expression level of MCT4 was positively correlated with the clinical stage, lymph node metastasis and the expression level of LDH. The nomogram model incorporating age, clinical stage, MCT4 expression, NLR, LDH, and CEA may improve the predictive accuracy for the prognosis of LUAD patients treated with PD-1/PD-L1 inhibitors.
Data Availability Statement
The public data cohorts analyzed in this study can be found in TCGA (https://portal.gdc.cancer.gov/). The raw data supporting the conclusions of this article are available from the corresponding author on reasonable request.
Funding
This research was supported by the Anhui Hygiene and Health Research Project (No. AHWJ2022a001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature. 2018;553(7689):446–454. doi:10.1038/nature25183
3. Chen P, Liu Y, Wen Y, Zhou C. Non-small cell lung cancer in China. Cancer Commun. 2022;42(10):937–970. doi:10.1002/cac2.12359
4. Zhang X, Wu X, Huang H, et al. Research into the biological differences and targets in lung cancer patients with diverse immunotherapy responses. Front Immunol. 2022;13:1014333. doi:10.3389/fimmu.2022.1014333
5. Hiam-Galvez KJ, Allen BM, Spitzer MH. Systemic immunity in cancer. Nat Rev Cancer. 2021;21(6):345–359. doi:10.1038/s41568-021-00347-z
6. Ngwa VM, Edwards DN, Philip M, Chen J. Microenvironmental metabolism regulates antitumor immunity. Cancer Res. 2019;79(16):4003–4008. doi:10.1158/0008-5472.CAN-19-0617
7. Shang S, Wang MZ, Xing Z, He N, Li S. Lactate regulators contribute to tumor microenvironment and predict prognosis in lung adenocarcinoma. Front Immunol. 2022;13. doi:10.3389/fimmu.2022.1024925
8. Faubert B, Li KY, Cai L, et al. Lactate metabolism in human lung tumors. Cell. 2017;171(2):358–371.e9. doi:10.1016/j.cell.2017.09.019
9. Mai S, Liang L, Mai G, et al. Development and validation of lactate metabolism-related lncRNA signature as a prognostic model for lung adenocarcinoma. Front Endocrinol. 2022;13:829175. doi:10.3389/fendo.2022.829175
10. Qian Y, Galan-Cobo A, Guijarro I, et al. MCT4-dependent lactate secretion suppresses antitumor immunity in LKB1-deficient lung adenocarcinoma. Cancer Cell. 2023;41(7):1363–1380.e7. doi:10.1016/j.ccell.2023.05.015
11. Babl N, Decking SM, Voll F, et al. MCT4 blockade increases the efficacy of immune checkpoint blockade. J Immunother Cancer. 2023;11(10):e007349. doi:10.1136/jitc-2023-007349
12. Zhao M, Huang C, Yang L, et al. SYVN1-mediated ubiquitylation directs localization of MCT4 in the plasma membrane to promote the progression of lung adenocarcinoma. Cell Death Dis. 2023;14(10):666. doi:10.1038/s41419-023-06208-x
13. Reuss AM, Groos D, Ghoochani A, Buchfelder M, Savaskan N. MCT4 promotes tumor malignancy in F98 glioma cells. J Oncol. 2021;2021:6655529. doi:10.1155/2021/6655529
14. Yuan C, Zhang J, Lou J, et al. Comprehensive analysis of monocarboxylate transporter 4 (MCT4) expression in breast cancer prognosis and immune infiltration via integrated bioinformatics analysis. Bioengineered. 2021;12(1):3850–3863. doi:10.1080/21655979.2021.1951928
15. Yu T, Liu Z, Tao Q, et al. Targeting tumor-intrinsic SLC16A3 to enhance anti-PD-1 efficacy via tumor immune microenvironment reprogramming. Cancer Lett. 2024;589:216824. doi:10.1016/j.canlet.2024.216824
16. Singh M, Afonso J, Sharma D, et al. Targeting monocarboxylate transporters (MCTs) in cancer: how close are we to the clinics?. Semi Cancer Biol. 2023;90:1–14. doi:10.1016/j.semcancer.2023.01.007
17. Sung M, Jang WS, Kim HR, et al. Prognostic value of baseline and early treatment response of neutrophil-lymphocyte ratio, C-reactive protein, and lactate dehydrogenase in non-small cell lung cancer patients undergoing immunotherapy. Transl Lung Cancer Res. 2023;12(7):1506. doi:10.21037/tlcr-23-7
18. Criscitiello C, Marra A, Morganti S, et al. Pretreatment blood parameters predict efficacy from immunotherapy agents in early phase clinical trials. Oncologist. 2020;25(11):e1732–e1742. doi:10.1634/theoncologist.2020-0518
19. Jiang ZF, Wang M, Xu JL. Thymidine kinase 1 combined with CEA, CYFRA21-1 and NSE improved its diagnostic value for lung cancer. Life Sci. 2018;194:1–6. doi:10.1016/j.lfs.2017.12.020
20. Wang Y, Lu J, Wu C, Fei F, Chu Z, Lu P. Clinical markers predict the efficacy of several immune checkpoint inhibitors in patients with non-small cell lung cancer in China. Front Immunol. 2023;14:1276107. doi:10.3389/fimmu.2023.1276107
21. Claps G, Faouzi S, Quidville V, et al. The multiple roles of LDH in cancer. Nat Rev Clin Oncol. 2022;19(12):749–762. doi:10.1038/s41571-022-00686-2
22. Tran TO, Vo TH, Lam LHT, Le NQK. ALDH2 as a potential stem cell-related biomarker in lung adenocarcinoma: comprehensive multi-omics analysis. Comput Struct Biotechnol J. 2023;21:1921. doi:10.1016/j.csbj.2023.02.045
23. Dang HH, Ta HDK, Nguyen TTT, et al. Identifying GPSM family members as potential biomarkers in breast cancer: a comprehensive bioinformatics analysis. Biomedicines. 2021;9(9):1144. doi:10.3390/biomedicines9091144
24. Liao C, Wang X. TCGAplot: an R package for integrative pan-cancer analysis and visualization of TCGA multi-omics data. BMC Bioinf. 2023;24:483. doi:10.1186/s12859-023-05615-3
25. Sturm G, Finotello F, Petitprez F, et al. Comprehensive evaluation of transcriptome-based cell-type quantification methods for immuno-oncology. Bioinformatics. 2019;35(14):i436. doi:10.1093/bioinformatics/btz363
26. Chen B, Khodadoust MS, Liu CL, Newman AM, Alizadeh AA. Profiling tumor infiltrating immune cells with CIBERSORT. Methods Mol Biol. 2018;1711:243. doi:10.1007/978-1-4939-7493-1_12
27. Charoentong P, Finotello F, Angelova M, et al. Pan-cancer immunogenomic analyses reveal genotype-immunophenotype relationships and predictors of response to checkpoint blockade. Cell Rep. 2017;18(1):248–262. doi:10.1016/j.celrep.2016.12.019
28. Zheng X, Zhang L, Wu L, et al. Baseline C-reactive protein predicts efficacy of the first-line immune checkpoint inhibitors plus chemotherapy in advanced lung squamous cell carcinoma: a retrospective, multicenter study. BMC Cancer. 2023;23:1244. doi:10.1186/s12885-023-11737-x
29. Yong J, Huang L, Chen G, Luo X, Chen H, Wang L. High expression of Stabilin-2 predicts poor prognosis in non-small-cell lung cancer. Bioengineered. 2021;12(1):3426–3433. doi:10.1080/21655979.2021.1943109
30. Liu C, Huang Q, Ma W, et al. A combination of tumor and molecular markers predicts a poor prognosis in lung adenocarcinoma. Int J Clin Exp Pathol. 2019;12(5):1690–1701.
31. Seymour L, Bogaerts J, Perrone A, et al. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017;18(3):e143–e152. doi:10.1016/S1470-2045(17)30074-8
32. Zhang B, Xie L, Liu J, Liu A, He M. Construction and validation of a cuproptosis-related prognostic model for glioblastoma. Front Immunol. 2023;14:1082974. doi:10.3389/fimmu.2023.1082974
33. Liu YG, Jiang ST, Zhang JW, et al. Development and validation of web-based nomograms for predicting survival status in patients with intrahepatic cholangiocarcinoma depending on the surgical status: a SEER database analysis. Sci Rep. 2024;14:1568. doi:10.1038/s41598-024-52025-3
34. Tao Q, Li X, Zhu T, et al. Lactate transporter SLC16A3 (MCT4) as an onco-immunological biomarker associating tumor microenvironment and immune responses in lung cancer. IJGM. 2022;15:4465–4474. doi:10.2147/IJGM.S353592
35. Mosca M, Nigro MC, Pagani R, De giglio A, Di Federico A. Neutrophil-to-Lymphocyte Ratio (NLR) in NSCLC, gastrointestinal, and other solid tumors: immunotherapy and beyond. Biomolecules. 2023;13(12):1803. doi:10.3390/biom13121803
36. Russo E, Guizzardi M, Canali L, et al. Preoperative systemic inflammatory markers as prognostic factors in differentiated thyroid cancer: a systematic review and meta-analysis. Rev Endocr Metab Disord. 2023;24(6):1205–1216. doi:10.1007/s11154-023-09845-x
37. Yan C, Yang G, Zhang C, et al. A nomogram based on circulating CD8+ T cell and platelet-to-lymphocyte ratio to predict overall survival of patients with locally advanced nasopharyngeal carcinoma. Radiat Oncol. 2024;19:108. doi:10.1186/s13014-024-02500-y
38. Cedrés S, Nuñez I, Longo M, et al. Serum tumor markers CEA, CYFRA21-1, and CA-125 are associated with worse prognosis in advanced Non–Small-Cell Lung Cancer (NSCLC). Clin Lung Cancer. 2011;12(3):172–179. doi:10.1016/j.cllc.2011.03.019
39. Wang R, Xu B, Sun M, et al. Dynamic monitoring of serum CEA and CA19-9 predicts the prognosis of postoperative stage II colon cancer. Eur J Surg Oncol. 2023;49(12):107138. doi:10.1016/j.ejso.2023.107138
40. Draoui N, Feron O. Lactate shuttles at a glance: from physiological paradigms to anti-cancer treatments. Dis Model Mech. 2011;4(6):727–732. doi:10.1242/dmm.007724
41. Liang J, Wang X, Yang J, et al. Identification of disulfidptosis-related subtypes, characterization of tumor microenvironment infiltration, and development of a prognosis model in breast cancer. Front Immunol. 2023;14:1198826. doi:10.3389/fimmu.2023.1198826
42. Sun Q, Zheng S, Tang W, et al. Prediction of lung adenocarcinoma prognosis and diagnosis with a novel model anchored in circadian clock-related genes. Sci Rep. 2024;14:18202. doi:10.1038/s41598-024-68256-3
43. Zeng J, Wu Z, Luo M, et al. Development and validation of an endoplasmic reticulum stress long non-coding RNA signature for the prognosis and immune landscape prediction of patients with lung adenocarcinoma. Front Genetics. 2023;14:1024444. doi:10.3389/fgene.2023.1024444
44. Huang P, Xu L, Jin M, et al. Construction and validation of a tumor microenvironment-based scoring system to evaluate prognosis and response to immune checkpoint inhibitor therapy in lung adenocarcinoma patients. Genes. 2022;13(6):951. doi:10.3390/genes13060951
45. Chang W, Li H, Zhong L, et al. Development of a copper metabolism-related gene signature in lung adenocarcinoma. Front Immunol. 2022;13:1040668. doi:10.3389/fimmu.2022.1040668
46. Zhai WY, Duan FF, Chen S, et al. A novel inflammatory-related gene signature based model for risk stratification and prognosis prediction in lung adenocarcinoma. Front Genetics. 2022;12:798131. doi:10.3389/fgene.2021.798131
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comprehensive Analysis of the E2F Transcription Factor Family in Human Lung Adenocarcinoma
Wang Q, Liu J, Cheang I, Li J, Chen T, Li Y, Yu B
International Journal of General Medicine 2022, 15:5973-5984
Published Date: 2 July 2022
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
A Nomogram Based on SEER Database for Predicting Prognosis in Patients with Mucinous Ovarian Cancer: A Real-World Study
Zhang K, Feng S, Ge Y, Ding B, Shen Y
International Journal of Women's Health 2022, 14:931-943
Published Date: 26 July 2022
Expression, Clinical Significance, Immune Infiltration, and Regulation Network of miR-3940-5p in Lung Adenocarcinoma Based on Bioinformatic Analysis and Experimental Validation
Lin Z, Huang W, Xie Z, Yi Y, Li Z
International Journal of General Medicine 2022, 15:6451-6464
Published Date: 6 August 2022
Nomogram for the Preoperative Prediction of the Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma
Shan Y, Yu X, Yang Y, Sun J, Wu S, Mao S, Lu C
Journal of Hepatocellular Carcinoma 2022, 9:717-728
Published Date: 10 August 2022