")
Back to Journals » Journal of Inflammation Research » Volume 17
The Predictive Value of SII Combined with UHR for Contrast-Induced Acute Kidney Injury in Patients with Acute Myocardial Infarction After Percutaneous Coronary Intervention
Authors Wang L , Xu Y , Zhang X , Ding J, Jin J , Zong J, Li F, Qian W, Li W
Received 16 June 2024
Accepted for publication 25 September 2024
Published 2 October 2024 Volume 2024:17 Pages 7005—7016
DOI https://doi.org/10.2147/JIR.S482977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Linsheng Wang,1,* Yang Xu,2,* Xudong Zhang,1 Jiahui Ding,1 Jingkun Jin,1 Jing Zong,1 Fangfang Li,1 Weidong Qian,3 Wenhua Li1,4
1Institute of Cardiovascular Diseases, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of Cardiology, Xuzhou Central Hospital, Xuzhou, Jiangsu, People’s Republic of China; 3Department of Cardiology, Wujin Affiliated Hospital of Nanjing University of Chinese Medicine, Changzhou, Jiangsu, People’s Republic of China; 4Department of Cardiology, Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weidong Qian, Department of Cardiology, Wujin Affiliated Hospital of Nanjing University of Chinese Medicine, Changzhou, Jiangsu, People’s Republic of China, Email [email protected] Wenhua Li, Department of Cardiology, Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China, Email [email protected]
Background: Contrast-induced acute kidney injury (CI-AKI) refers to the acute renal dysfunction caused by the injection of contrast agents. CI-AKI is currently a common complication after percutaneous coronary intervention (PCI).
Objective: To investigate the predictive value of the combined systemic inflammatory index (SII) and urate/high-density lipoprotein cholesterol ratio (UHR) for CI-AKI after PCI in patients with AMI.
Methods: A total of 1222 patients with AMI who underwent PCI were randomly divided into a training group and a validation group in an 8:2 ratio. According to the definition of CI-AKI diagnostic criteria, the training group was divided into CI-AKI group and non-CI-AKI group. Collect patient’s blood and biochemical data, then calculate SII and UHR. The risk factors for CI-AKI were identified using LASSO and multivariate logistic regression analyses. A predictive column was created by using R language.Evaluate the predictive value of SII, UHR and their combination for CI-AKI after PCI using the area under the ROC curve (AUC).
Results: Diabetes, Cystatin C, Diuretics, UHR, and LnSII were independent risk factors for CI-AKI in AMI patients after PCI. The ROC curve showed that the AUC of UHR and SII combined for predicting CI-AKI in AMI patients after PCI was 0.761 (95% CI: 0.709– 0.812), with a sensitivity of 65.20% and a specificity of 76.70%, which was better than the prediction by either factor alone.
Conclusion: High SII and high UHR are risk factors for AMI, and their combination can improve the accuracy of predicting CI-AKI in AMI patients after PCI.The prognosis of CI-AKI in AMI patients is worse than in the general population.
Keywords: serum uric acid, high-density lipoprotein cholesterol, neutrophils, lymphocytes, systemic immune-inflammatory index, contrast-induced acute kidney injury
Introduction
Percutaneous Coronary Intervention (PCI) is a common approach for managing Acute Myocardial Infarction (AMI) presently.Contrast-induced acute kidney injury (CI-AKI) refers to iatrogenic acute renal dysfunction caused by the administration of contrast agents.1 Research has indicated that CI-AKI is associated with adverse clinical outcomes such as increased cardiovascular events, chronic kidney disease, renal replacement therapy, and elevated long-term mortality rates.2 Currently, there is a lack of targeted treatment strategies for CI-AKI, and clinical management primarily revolves around supportive care.3 Therefore, early identification of high-risk patients is paramount in preventing and managing CI-AKI and its severe complications.
 |
Figure 1 The flow chart describes the selection and statistical analysis of patients undergoing PCI for acute myocardial infarction. |
Inflammation is a defensive response of the body centered on vascular reactions, triggered by stimuli and injury factors. Research has confirmed that inflammation plays a pivotal role in the development of CI-AKI.4 The systemic immune-inflammation index (SII), as an effective indicator of overall inflammation status, was initially used for prognostic assessment in malignant tumor diseases.5 Recent research has found that it can also be utilized for early prediction of CI-AKI.6 The serum uric acid/high-density lipoprotein cholesterol ratio (UHR) is a newly discovered inflammatory marker closely associated with various inflammatory diseases such as thyroiditis, diabetic nephropathy, and non-alcoholic fatty liver disease.7 This study aims to investigate the combined predictive value of SII and UHR for CI-AKI in patients with AMI undergoing PCI, providing novel insights for early identification of CI-AKI patients in clinical practice.
Materials and Methods
Study Population
The study included clinical data from 1222 patients who underwent routine PCI at The Affiliated Hospital of Xuzhou Medical University between January 2020 and May 2023 due to AMI (Figure 1). The patients were randomly divided into a training group (n=977) and a validation group (n=245) in an 8:2 ratio. Inclusion criteria:Patients who meet the diagnostic criteria for AMI as outlined by the American College of Cardiology/American Heart Association (ACC/AHA) and undergo PCI after hospital admission.8 Exclusion criteria: (1) Patients with severe infection, electrolyte imbalances, severe heart failure, myocarditis, cardiomyopathy, or valvular heart disease. (2) Patients with malignant tumors, hematological diseases, autoimmune diseases, or thyroid diseases. (3) Patients with allergies to iodine and other contrast agents. (4) Patients who have recently taken nephrotoxic drugs. (5) Patients with estimated glomerular filtration rate (eGFR) <15mL/(min·1.73m2) at admission. (6) Patients who have been in contact with nephrotoxic or radioactive drugs within 48 hours before or after surgery. (7) Patients with incomplete clinical data collection.
Definition
The diagnostic criteria for CI-AKI: exclusion of other potential causes of renal damage, any acute kidney injury occurring 48–72 hours after administration of contrast agents, defined as an increase in serum creatinine (Scr) level ≥ 0.3 mg/dL (26.5 μmol/L) above baseline or reaching 1.5 times the baseline level.9 All patients were calculated for eGFR using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula.9 Since most patients did not have their urine output measured, this study did not use urine output criteria to determine the occurrence of CI-AKI. The SII is calculated by multiplying the platelet count by the neutrophil count and then dividing it by the lymphocyte count. The UHR was calculated as the preoperative serum uric acid value divided by high-density lipoprotein cholesterol value.
Data Collection and Therapeutic Schedule
All patients had their general information collected and underwent tests for blood routine, biochemistry, coagulation function, etc. After obtaining the patient’s medical history and analyzing the test results. Next, patients were immediately administered with aspirin 300mg, clopidogrel 300mg, or ticagrelor 180mg, followed by intravenous injection of heparin (100U/kg). All PCI procedures were performed by experienced experts at our hospital based on angiography results with stent implantation or balloon dilation.The procedure is conducted via radial or brachial artery puncture with appropriate catheter placement and administration of low-osmolality non-ionic iodinated contrast agent (iodixanol) for coronary angiography. Interventional therapy was then conducted according to lesion severity.Individualized fluid therapy was administered to patients based on their cardiac and renal function before and after PCI. Typically, 0.9% physiological saline was initiated 3 hours prior to the procedure and administered continuously via intravenous infusion at a rate of 1–2mL·kg−1·h−1 until 24 hours post-procedure, in accordance with individual patient needs.10
Statistical Analysis
Statistical analysis was conducted using SPSS 26.0 and the R software package (version 4.3.2). Normality tests were performed on metric data, with normally distributed continuous variables presented as mean±standard deviation ( ), and independent sample t-tests used to analyze inter-group differences. For non-normally distributed metric data, median (interquartile range) [M(Q1,Q3)] was utilized, and Mann–Whitney U-test employed for observing inter-group differences. Count data and categorical variables were represented by specific examples (percentages) [n(%)], with group comparisons conducted using the chi-square test. LASSO regression was carried out using the “glmnet” package, while multivariate Logistic regression utilized the “glm” package. The Nomogram was constructed using the “rms” package, ROC curves were plotted using “pROC” package, HL tests were performed employing the “ResourceSelection” package, calibration curves drawn utilizing val.prob function and calibrate in the “rms” package, and DCA curves created through use of the “dca.R” package. A significance level of P<0.05 denoted statistical significance.
), and independent sample t-tests used to analyze inter-group differences. For non-normally distributed metric data, median (interquartile range) [M(Q1,Q3)] was utilized, and Mann–Whitney U-test employed for observing inter-group differences. Count data and categorical variables were represented by specific examples (percentages) [n(%)], with group comparisons conducted using the chi-square test. LASSO regression was carried out using the “glmnet” package, while multivariate Logistic regression utilized the “glm” package. The Nomogram was constructed using the “rms” package, ROC curves were plotted using “pROC” package, HL tests were performed employing the “ResourceSelection” package, calibration curves drawn utilizing val.prob function and calibrate in the “rms” package, and DCA curves created through use of the “dca.R” package. A significance level of P<0.05 denoted statistical significance.
Results
Basic Information Comparison
There were statistically significant differences in age, gender distribution, presence of diabetes, left ventricular ejection fraction, and use of diuretics between the two groups (P < 0.05). No statistically significant differences were observed in other indicators (P > 0.05), as detailed in.Table 1
 |
Table 1 The Comparison of Basic Information Between the Two Groups of Patients |
Comparison of Preoperative Laboratory Data
The preoperative levels of serum urea, uric acid, serum creatinine, cystatin C, HDL-C, FPG, Hs-CRP, FIB, neutrophil count, lymphocyte count and monocyte count as well as hemoglobin and platelet distribution width showed statistically significant differences between the two groups (P<0.05), while no statistically significant differences were observed in other indicators (P>0.05). Please refer to Table 2 for details.
 |
Table 2 Laboratory Data of Patients in Both Groups Before PCI |
LASSO Clinical Feature Selection
We included 45 indicators as independent variables and whether CI-AKI occurred as the dependent variable. The optimal penalty coefficient λ was identified using 10-fold cross-validation, with a value of Lambda.1se at 0.04209988. Five variables were selected: diabetes mellitus, cystatin C level, diuretic, UHR, and LnSII (as shown in Figure 2A and B).
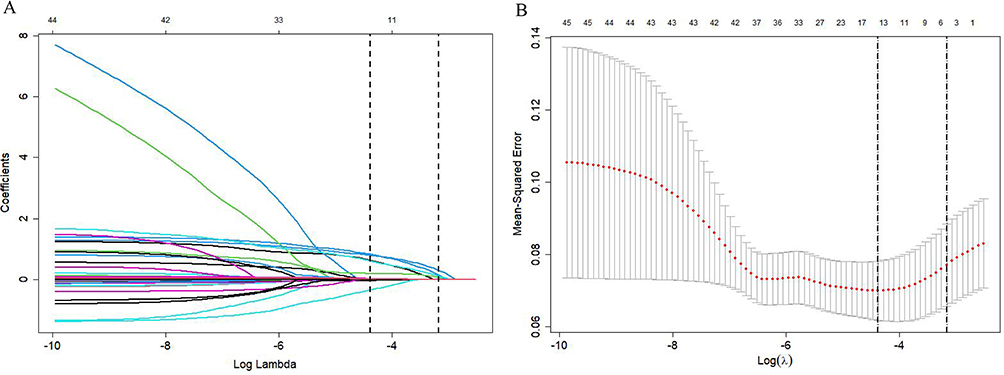 |
Figure 2 This is LASSO regression. (A)This graph shows the coefficient curve of the independent variable. (B)This graph shows the selection of the optimal independent variable by LASSO regression and 10-fold cross-validation. |
Analysis of Risk Factors for CI-AKI
The above-mentioned 5 variables selected by LASSO regression were included in the multivariate logistic regression. The results indicated that all 5 indicators were independent risk factors for the occurrence of CI-AKI in AMI patients after PCI (P<0.05). Please refer to Table 3 for details.
 |
Table 3 Multivariate Logistic Regression Analysis of CI-AKI Incidence |
Nomogram Construction and Prediction Analysis
Based on the results of the multivariate logistic regression, a prediction model was used to evaluate the factors in.Figure 3 The ROC curve for predicting CI-AKI occurrence in the training group had an area under the curve (AUC) of 0.842 (95% CI: 0.800–0.884), with a specificity of 78.00% and a sensitivity of 76.40%, demonstrating good discriminatory ability as depicted in.Figure 4A The Hosmer-Lemeshow test showed χ2 = 7.6112, P = 0.4723 in the training group, indicating good model fit; internal validation using Bootstrap sampling over 1000 iterations revealed that the calibration curve displayed strong consistency between predicted and actual risk, as shown in.Figure 5A
 |
Figure 3 This is a nomogram of CI-AKI in AMI patients after PCI. |
 |
Figure 4 These two graphs are ROC curves. (A)This graph shows ROC curves for predicting CI-AKI in AMI patients in training group. (B)This graph shows ROC curves for predicting CI-AKI in AMI patients in validation group. |
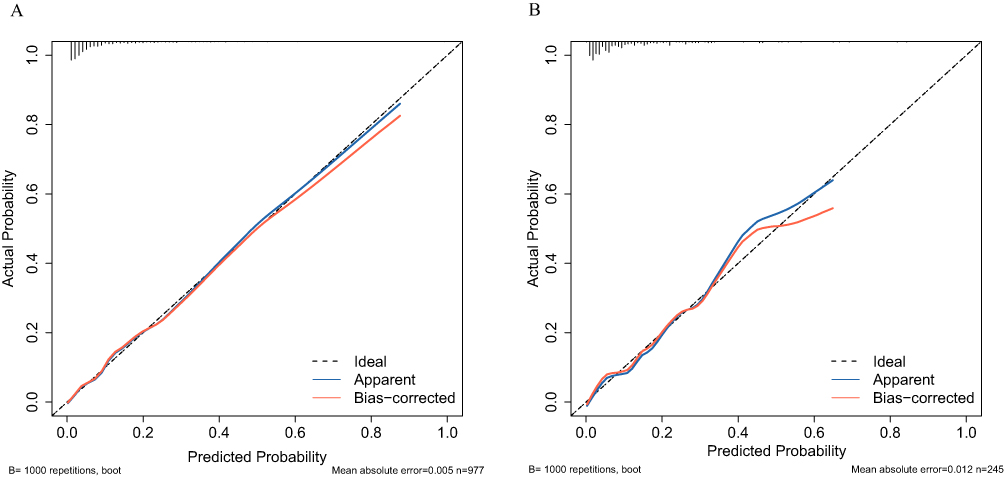 |
Figure 5 These two graphs are calibration curves. (A)This graph shows the calibration curve of CI-AKI in AMI patients after PCI in training group. (B)This graph shows the calibration curve of CI-AKI in AMI patients after PCI in validation group. |
Calibration Verification of the Nomogram
In the validation group, a total of 245 cases were included, with 27 (11.02%) developing CI-AKI. The area under the ROC curve (AUC) for predicting CI-AKI in the validation group was 0.831 (95% CI: 0.753–0.909), as depicted in.Figure 4B The Hosmer-Lemeshow test showed χ2 = 4.678, P = 0.791, indicating good model fit. Internal calibration through 1000 bootstrap resamplings demonstrated that the predicted values closely represented actual values, as illustrated in.Figure 5B
Decision Curve Analysis and Clinical Impact Curve
As depicted in Figure 6A and B the horizontal line on the DCA curve represents no intervention, with a net benefit of zero, and the sloping line represents intervention for all patients. The predictive model demonstrates a favorable net benefit. As depicted in the graph, the wide range of high-risk threshold probability is applicable to both the modeling and validation sets, indicating the practical utility of this model in clinical settings.The clinical impact curve in Figure 7 illustrates that among 1000 patients, the blue solid line represents the total number of patients considered high-risk at each risk threshold, while the red dashed line indicates how many of these are true positive cases.This figure also illustrates the clinical efficacy of the predictive model. When the threshold probability exceeds 64%, the model’s identification of high-risk CI-AKI individuals closely aligns with the actual incidence of CI-AKI, thereby confirming the high clinical efficacy of this predictive model.
 |
Figure 6 These two graphs are DCA curves. (A)This graph shows the DCA curve of CI-AKI in AMI patients after PCI in training group. (B)This graph shows the DCA curve of CI-AKI in AMI patients after PCI in validation group. |
 |
Figure 7 This is a CIC curve of CI-AKI in AMI patients after PCI. |
ROC Curve Analysis of Clinical Value of UHR, SII and Their Combination in Predicting CI-AKI After PCI
The UHR predicts an AUC of 0.701 (95% CI: 0.643–0.760, P<0.001) for CI-AKI after PCI, while the SII predicts an AUC of 0.692 (95% CI: 0.633–0.751, P<0.001). When combined, the two models yield a predictive AUC of 0.761 (95% CI: 0.709–0.812, P<0.001) for CI-AKI occurrence, with a sensitivity of 65.20% and specificity of 76.00%.
Comparison of Incidence Rates of CI-AKI Between Patients with Different Levels of UHR and SII
Based on the ROC curves of UHR and SII, the optimal cut-off values were determined to be 293.8 for UHR and 1622.5 for SII. Subsequently, all patients were categorized into three groups: low-risk group (401 cases, low UHR + low SII), moderate-risk group (443 cases, low UHR + high SII or high UHR + low SII), and high-risk group (133 cases, high UHR + high SII). The results revealed that the incidence of CI-AKI in the low-risk group, moderate-risk group, and high-risk group was 8 cases (2.00%), 45 cases (10.16%), and 36 cases (27.07%) respectively. Furthermore, there was a significant increase in the incidence of CI-AKI with escalating risk levels (χ2=76.906, P<0.001)(Table 4).
 |
Table 4 Comparison of Incidence Rates of CI-AKI Between Different Levels of UHR and SII |
Discussion
The iodine contrast agent used during PCI is excreted by the kidneys in 99% of cases.11 Therefore, as the number of PCI procedures for AMI patients increases, the incidence of CI-AKI, a negative event after PCI, also increases.CI-AKI has become the third most common cause of hospital-acquired renal failure, with an incidence rate ranging from 8.8% to 20%.12 In this study, the incidence rate of CI-AKI was approximately 9.1%, consistent with previous research findings. CI-AKI not only escalates patient medical costs but also inflicts physical and psychological trauma on patients.
The pathogenesis of CI-AKI is currently not well understood, and effective treatments for CI-AKI are still lacking.13,14 Therefore, early prediction and prevention are particularly important. Scr is a widely recognized diagnostic marker for CI-AKI in clinical practice, but its sensitivity is not high as it typically begins to rise 24 hours after the use of contrast agents.15,16 In recent years, some researchers have studied the use of markers such as neutrophil gelatinase-associated lipocalin and hepcidin regulatory protein for diagnosing CI-AKI, but their limited availability has hindered widespread usage.17,18 Thus, there is a need to identify early, specific, and sensitive predictors of renal injury that would hold significant clinical value in preventing CI-AKI.
UHR is an index that integrates uric acid and lipid levels, calculated from the combination of uric acid and HDL-C. Uric acid can be regarded as an oxidant in the body, inhibiting the release of nitric oxide (NO) by endothelial cells, leading to vasoconstriction and ischemia.19,20 Uric acid also activates the RAS system, inducing the production of angiotensin II in the body, stimulating vascular smooth muscle cell proliferation and causing inflammatory reactions.21,22 Additionally, uric acid crystals can deposit in vessel walls, triggering inflammatory responses and directly causing damage to renal vascular endothelial cells.23 Therefore, hyperuricemia may play a significant role in renal vascular inflammation and injury. HDL-C is a polymer composed of hundreds of proteins and lipids that transport cholesterol from extrarenal tissues and cells to the liver for degradation, exerting antioxidative and anti-atherosclerotic effects.24 It also reduces platelet aggregation and inhibits activation of the coagulation cascade, thereby maintaining low blood clotting status while reducing thrombus formation to protect renal vasculature.25,26 Furthermore, Jia C et al’s research indicated that HDL-C prevents early monocyte adhesion to endothelial cell surfaces by reducing expression levels of adhesion molecule 1 (VCAM-1), thus alleviating systemic inflammatory reactions.27 Park et al’s study demonstrated that low HDL-C is a high-risk factor for CI-AKI following PCI in patients with coronary heart disease.28
SII is a novel biomarker derived from the calculation of neutrophil count, platelet count, and lymphocyte count.29 It integrates the body’s inflammatory and immune responses and holds greater clinical utility than individual markers. During AMI occurrence, there is an enhanced inflammatory response in the patient’s body, leading to significant secretion of tissue proteases such as collagenase G and elastase by neutrophils, along with the release of oxygen free radicals.30 These inflammatory mediators enter endothelial cells in the kidneys, ultimately causing or exacerbating renal injury. Additionally, factors such as stress response lead to elevated levels of hormones like cortisol in the body while lymphocytes sequentially decrease.31 Furthermore, the release of anti-inflammatory factors also induces apoptosis in lymphocytes.32 Lymphocytes serve as representative cells in immune processes and play a role in maintaining stability within renal vascular endothelium while slowing down inflammation progression. A reduction in lymphocyte numbers results in decreased immune function within the body which further aggravates renal endothelial dysfunction.33 Moreover, the inflammatory response prompts excessive activation of platelets leading to their adhesion on inner walls of renal blood vessels causing microcirculation disturbances. During this process, platelets release substantial amounts of inflammatory factors thereby worsening damage to renal vascular endothelium.34 Consequently, elevated SII may impact CI-AKI occurrence through both inflammation and active coagulation pathways.
The results of this study indicate that UHR and SII can be used as reference indexes to predict CI-AKI in AMI patients after PCI. The ROC curve demonstrates that the combined prediction of these two indicators yields the largest AUC, with good sensitivity and specificity, providing greater value than using a single indicator for prediction and enhancing predictive accuracy.
Limitations
Firstly, it is important to note that this study is a single-center cross-sectional study with a small sample size, and some patients were excluded due to incomplete data, potentially introducing selection bias. Further validation through a multicenter, large-sample evidence-based study is warranted.Secondly, Patients were not followed up for future adverse events. Finally, due to the lack of accurate and complete urine volume, this study only used Scr to assess the occurrence of CI-AKI in patients, and some patients who only met the diagnostic criteria for CI-AKI urine volume were excluded.
Conclusion
This study demonstrates that the presence of diabetes, use of diuretics, cystatin C, UHR and SII are independent risk factors for the development of CI-AKI in AMI patients following PCI. When clinicians perform a comprehensive assessment of AMI patients before PCI, UHR and SII can serve as reference indicators to predict the occurrence of CI-AKI after PCI in AMI patients. The ROC curve demonstrates that the combined prediction of these two indicators yields the largest AUC, with good sensitivity and specificity, providing greater value than using a single indicator for prediction and enhancing predictive accuracy.
Ethic Approval
The study was approved by the Ethics Committee of The Affiliated Hospital of Xuzhou Medical University (ethics approval number: XYFY2022-KL122-01) and informed consent was obtained from all participants. Our study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors report no conflict of interest in this work.
References
1. Macdonald DB, Hurrell C, Costa AF, et al. Canadian Association of Radiologists Guidance on Contrast Associated Acute Kidney Injury. Can Assoc Radiol J. 2022;73(3):499–514. doi:10.1177/08465371221083970
2. Nakano M. Is Longer an Obstacle to Angiography and Intervention in Patients With Chronic Kidney Disease? Circ J. 2022;86(5):797–798. doi:10.1253/circj.CJ-22-0141
3. Sůva M, Kala P, Poloczek M, et al. Contrast-induced acute kidney injury and its contemporary prevention. Front Cardiovasc Med. 2022;9:1073072. doi:10.3389/fcvm.2022.1073072
4. Mehran R, Dangas GD, Weisbord SD. Contrast-Associated Acute Kidney Injury. N Engl J Med. 2019;380(22):2146–2155. doi:10.1056/NEJMra1805256
5. Jarmuzek P, Kozlowska K, Defort P, et al. Prognostic Values of Systemic Inflammatory Immunological Markers in Glioblastoma: a Systematic Review and Meta-Analysis. Cancers. 2023;15(13):3339. doi:10.3390/cancers15133339
6. Jiang H, Li D, Xu T, et al. Systemic Immune-Inflammation Index Predicts Contrast-Induced Acute Kidney Injury in Patients Undergoing Coronary Angiography: a Cross-Sectional Study. Front Med Lausanne. 2022;9:841601. doi:10.3389/fmed.2022.841601
7. Han X, Tan X, Liu M, et al. Association between serum uric acid/high-density lipoprotein cholesterol ratio and hypertension among reproductive-aged women. J Health Popul Nutr. 2023;42(1):123. doi:10.1186/s41043-023-00458-3
8. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction. Eur Heart J. 2019;40(3):237–269. doi:10.1093/eurheartj/ehy462
9. van der Molen AJ, Reimer P, Dekkers IA, et al. Post-contrast acute kidney injury - Part 1: definition, clinical features, incidence, role of contrast medium and risk factors: recommendations for updated ESUR Contrast Medium Safety Committee guidelines. Eur Radiol. 2018;28(7):2845–2855. doi:10.1007/s00330-017-5246-5
10. Andreucci M. Side effects of radiographic contrast media. Biomed Res Int. 2014;2014:872574. doi:10.1155/2014/872574
11. Andreucci M, Faga T, Pisani A, et al. Acute kidney injury by radiographic contrast media: pathogenesis and prevention. Biomed Res Int. 2014;2014:362725. doi:10.1155/2014/362725
12. Werner S, Bez C, Hinterleitner C, et al. Incidence of contrast-induced acute kidney injury (CI-AKI) in high-risk oncology patients undergoing contrast-enhanced CT with a reduced dose of the iso-osmolar iodinated contrast medium iodixanol. PLoS One. 2020;15(5):e0233433. doi:10.1371/journal.pone.0233433
13. Wang H, Gao T, Zhang R, et al. The intellectual base and global trends in contrast-induced acute kidney injury: a bibliometric analysis. Ren Fail. 2023;45(1):2188967. doi:10.1080/0886022X.2023.2188967
14. Li Y, Wang J. Contrast-induced acute kidney injury: a review of definition, pathogenesis, risk factors, prevention and treatment. BMC Nephrol. 2024;25(1):140. doi:10.1186/s12882-024-03570-6
15. Li Q, Huang Y, Shang W, et al. The Predictive Value of Urinary Kidney Injury Molecular 1 for the Diagnosis of Contrast-Induced Acute Kidney Injury after Cardiac Catheterization: a Meta-Analysis. J Interv Cardiol. 2020;2020:4982987. doi:10.1155/2020/4982987
16. Isaka Y, Hayashi H, Aonuma K, et al. Guideline on the use of iodinated contrast media in patients with kidney disease 2018. Jpn J Radiol. 2020;38(1):3–46. doi:10.1007/s11604-019-00850-2
17. Seibert FS, Heringhaus A, Pagonas N, et al. Biomarkers in the prediction of contrast media induced nephropathy - The BITCOIN study. PLoS One. 2020;15(7):e0234921. doi:10.1371/journal.pone.0234921
18. González-Nicolás MÁ, González-Guerrero C, Goicoechea M, et al. Biomarkers in Contrast-Induced Acute Kidney Injury: towards A New Perspective. Int J Mol Sci. 2024;25(6):3438. doi:10.3390/ijms25063438
19. Hu X, Yang X, Li X, et al. Elevated uric acid is related to the no-/slow-reflow phenomenon in STEMI undergoing primary PCI. Eur J Clin Invest. 2022;52(4):e13719. doi:10.1111/eci.13719
20. Yu W, Cheng JD. Uric Acid and Cardiovascular Disease: an Update From Molecular Mechanism to Clinical Perspective. Front Pharmacol. 2020;11:582680. doi:10.3389/fphar.2020.582680
21. South AM, Shaltout HA, Nixon PA, et al. Association of circulating uric acid and angiotensin-(1-7) in relation to higher blood pressure in adolescents and the influence of preterm birth. J Hum Hypertens. 2020;34(12):818–825. doi:10.1038/s41371-020-0335-3
22. Corry DB, Eslami P, Yamamoto K, et al. Uric acid stimulates vascular smooth muscle cell proliferation and oxidative stress via the vascular renin-angiotensin system. J Hypertens. 2008;26(2):269–275. doi:10.1097/HJH.0b013e3282f240bf
23. Cabău G, Crișan TO, Klück V, et al. Urate-induced immune programming: consequences for gouty arthritis and hyperuricemia. Immunol Rev. 2020;294(1):92–105. doi:10.1111/imr.12833
24. Kon V, Yang H, Fazio S. Residual Cardiovascular Risk in Chronic Kidney Disease: role of High-density Lipoprotein. Arch Med Res. 2015;46(5):379–391. doi:10.1016/j.arcmed.2015.05.009
25. Chiesa ST, Charakida M. High-Density Lipoprotein Function and Dysfunction in Health and Disease. Cardiovasc Drugs Ther. 2019;33(2):207–219. doi:10.1007/s10557-018-06846-w
26. Huang Y, Ge H, Wang X, et al. Association Between Blood Lipid Levels and Lower Extremity Deep Venous Thrombosis: a Population-Based Cohort Study. Clin Appl Thromb Hemost. 2022;28:10760296221121282. doi:10.1177/10760296221121282
27. Jia C, Anderson JLC, Gruppen EG, et al. High-Density Lipoprotein Anti-Inflammatory Capacity and Incident Cardiovascular Events[J]. Circulation. 2021;143(20):1935–1945. doi:10.1161/CIRCULATIONAHA.120.050808
28. Park HS, Kim CJ, Hwang BH, et al. HDL Cholesterol Level Is Associated with Contrast Induced Acute Kidney Injury in Chronic Kidney Disease Patients Undergoing PCI. Sci Rep. 2016;6:35774. doi:10.1038/srep35774
29. Erdoğan M, Erdöl MA, Öztürk S, et al. Systemic immune-inflammation index is a novel marker to predict functionally significant coronary artery stenosis. Biomarker Med. 2020;14(16):1553–1561. doi:10.2217/bmm-2020-0274
30. Silvestre-Roig C, Braster Q, Ortega-Gomez A, et al. Neutrophils as regulators of cardiovascular inflammation. Nat Rev Cardiol. 2020;17(6):327–340. doi:10.1038/s41569-019-0326-7
31. Sarli B, Baktir AO, Saglam H, et al. Neutrophil-to-lymphocyte ratio is associated with severity of coronary artery ectasia. Angiology. 2013;65(2):147–151. doi:10.1177/0003319713488932
32. Szondy Z, Sarang Z, Kiss B, et al. Anti-inflammatory Mechanisms Triggered by Apoptotic Cells during Their Clearance. Front Immunol. 2017;8:909. doi:10.3389/fimmu.2017.00909.
33. Butt K, D’Souza J, Yuan C, et al. Correlation of the Neutrophil-to-Lymphocyte Ratio (NLR) and Platelet-to-Lymphocyte Ratio (PLR) with Contrast-Induced Nephropathy in Patients With Acute Coronary Syndrome Undergoing Percutaneous Coronary Interventions. Cureus. 2020;12(12):e11879. doi:10.7759/cureus.11879
34. Targoński R, Sadowski J, Price S, et al. Sodium-induced inflammation-an invisible player in resistant hypertension. Hypertens Res. 2020;43(7):629–633. doi:10.1038/s41440-020-0428-y
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.