")
Back to Journals » Journal of Inflammation Research » Volume 18
The Prognostic Role of Naples Prognostic Score in Patients with Coronary Artery Disease
Authors Jiang Y, Chen Y, Lu W, Peng Y, Chen L, Lin Y
Received 2 April 2025
Accepted for publication 21 May 2025
Published 30 May 2025 Volume 2025:18 Pages 6999—7012
DOI https://doi.org/10.2147/JIR.S527868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Yan Jiang,1 Yaqin Chen,1 Wen Lu,1 Yanchun Peng,2 Liangwan Chen,3,4 Yanjuan Lin2,3
1School of Nursing, Fujian Medical University, Fuzhou, Fujian, People’s Republic of China; 2Department of Nursing, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China; 3Department of Cardiovascular Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China; 4Fujian Provincial Special Reserve Talents Laboratory, Fuzhou, Fujian, People’s Republic of China
Correspondence: Liangwan Chen, Department of Cardiovascular Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China, Email [email protected] Yanjuan Lin, Department of Nursing, Fujian Medical University Union Hospital, Fuzhou, Fujian, People’s Republic of China, Email [email protected]
Background and Objective: The Naples Prognostic Score (NPS) is a tool for assessing inflammation and nutrition, widely used in outcome evaluation. However, its association with adverse outcomes in patients with coronary artery disease (CAD) has not been explored. This study aims to investigate the prognostic value of NPS in CAD patients.
Methods: This retrospective cohort study included 2453 patients with CAD who visited the Fujian Heart Medical Center between 2017 and 2022. Patients were divided into three groups based on NPS. The NPS was calculated based on serum albumin, total cholesterol, neutrophil-to-lymphocyte ratio, and lymphocyte-to-monocyte ratio. Univariate and multivariate regression analyses, along with Cox models, were used to assess the impact of NPS on adverse outcomes. Receiver operating characteristic (ROC) curves evaluated NPS’s accuracy in predicting all-cause in-hospital mortality.
Results: Patients with lower NPS scores are less likely to have comorbidities such as hyperlipidemia and chronic kidney disease. Additionally, they tend to use fewer medications for treatment. Multivariate analysis revealed that elevated NPS levels were independently associated with poorer clinical outcomes. Compared to group 1, the risk of all-cause mortality was significantly higher in groups 2 and 3 [group 2, adjusted odds ratio (aOR)=0.33; group 3, aOR=1.82; P=0.037], the risk of acute myocardial infarction was higher (group 2, aOR=2.41; group 3, aOR=4.05; P< 0.001), and the risk of stroke was also higher (group 2, aOR=1.26; group 3, aOR=1.80; P=0.039). ROC curve analysis showed that NPS could independently predict the risk of all-cause mortality in patients with CAD.
Conclusion: This study suggests that the NPS, a novel metric integrating inflammation and nutritional status, is closely associated with the prognosis of CAD.
Keywords: naples prognostic score, outcomes, coronary artery disease, prognosis
Introduction
Atherosclerotic cardiovascular disease (ASCVD) is a major non-communicable chronic disease that significantly threatens the health and life expectancy of China’s population. It is characterized by high incidence, disability, mortality, and economic burden.1,2 Coronary artery disease (CAD), which accounts for approximately 40%–50% of total ASCVD cases, is a leading contributor. In 2019, CAD was responsible for 1.87 million deaths in China, making it the second leading cause of death.3,4 With an aging population and the ongoing prevalence of risk factors, the challenges of CAD prevention and control are intensifying. Despite the increasing use of percutaneous coronary intervention (PCI) as an essential treatment for CAD, numerous studies have shown that while PCI can improve long-term outcomes, the short-term risks of adverse events such as contrast-induced nephropathy and major adverse cardiovascular and cerebrovascular events (MACCEs) remain high. These complications significantly elevate patient mortality and hospital readmission rates.5,6 Wang et al conducted a one-year follow-up study of PCI patients and reported a 41.5% incidence of MACCEs post-procedure.7 Given this, identifying reliable markers that can predict patient outcomes is crucial for early intervention in high-risk individuals, with the aim of reducing complications and improving patients’ quality of life.
Inflammation plays a key role in the onset and progression of CAD, contributing to endothelial dysfunction, cytokine production, and immune cell activation.8–10 Several inflammation-related markers, such as the neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), and platelet-to-lymphocyte ratio (PLR), have been proposed as potential biomarkers for the severity and prognosis of CAD.11–16 While elevated total cholesterol (TC), particularly low-density lipoprotein cholesterol (LDL-C), is traditionally considered a major risk factor for atherosclerotic cardiovascular disease, emerging evidence suggests that low TC may also be associated with adverse outcomes in certain clinical settings.17 This paradox may be explained by the fact that low TC can reflect underlying malnutrition or systemic inflammation, both of which are linked to poor prognosis. For instance, studies in patients with chronic heart failure and coronary slow flow have shown that lower cholesterol levels are associated with higher mortality, potentially due to cholesterol’s involvement in immune regulation and cellular repair.18 Nevertheless, findings across studies remain inconsistent, and the optimal cut-off values for these biomarkers have not been clearly established. In addition to inflammatory indices, nutritional markers—such as the prognostic nutritional index and the triglyceride-glucose index—have also been associated with the risk and complications of CAD.19,20 Nevertheless, the causal associations between these indices and CAD are not well-established, and the underlying mechanisms remain poorly understood. Thus, it is essential to further investigate the roles of inflammation and nutritional markers in CAD and assess their prognostic value. Individual inflammatory markers such as NLR, MLR, and PLR, as well as nutritional indicators like the prognostic nutritional index and the triglyceride-glucose index, typically reflect only isolated aspects of a disease and fail to provide a comprehensive assessment of a patient’s overall physiological condition. This limitation highlights the need for a more integrated approach, such as the NPS, to better capture the multifaceted nature of a patient’s health status. The NPS is a novel multidimensional assessment system that integrates both inflammatory and nutritional status based on four parameters: albumin, total cholesterol, NLR, and lymphocyte-to-monocyte ratio (LMR).21 The NPS offers several advantages over relying on individual biomarkers. By combining inflammatory and nutritional parameters, NPS provides a more comprehensive view of a patient’s health, capturing interactions between these factors that may not be apparent when assessed separately. While biomarkers like NLR, MLR and PLR offer valuable insights into specific aspects of a patient’s condition, they may not fully reflect the complexity of the overall prognosis.11–16 As a composite score, NPS has been shown to offer superior prognostic accuracy, better predicting patient outcomes than individual markers. Additionally, NPS simplifies clinical decision-making by providing a single, easy-to-interpret score, reducing the need to monitor multiple parameters. Thus, NPS enhances both the reliability and practicality of patient risk assessment, making it a valuable tool in clinical practice. Currently, The NPS has been validated in various cancers and non-malignant conditions. In patients with ampullary carcinoma and colorectal cancer, NPS independently predicts both short-term and long-term outcomes, with higher scores correlating with poorer survival. Additionally, in adult asthma patients, elevated NPS scores are associated with an increased risk of acute exacerbations and poorer disease control. These findings demonstrate that NPS not only holds prognostic value in cancer but also effectively predicts outcomes in non-malignant diseases, highlighting its broad potential for clinical application.21–23 However, its prognostic value in CAD has not yet been explored.
Therefore, this study aims to evaluate the predictive value of the NPS, as a novel multidimensional inflammatory and nutritional assessment tool, for the prognosis of CAD. By providing a more precise assessment, the NPS may help identify high-risk patients with poor outcomes, facilitating more accurate and timely clinical decision-making.
Methods
Study Design and Population
This retrospective study included 2,453 hospitalized patients diagnosed with CAD at the Fujian Heart Medical Center in Fuzhou, China, between May 2017 and December 2022. The inclusion criteria were: (1) patients aged 18 years or older; (2) all patients met the diagnostic criteria for CAD, defined as having at least one major coronary artery (left main coronary artery, left anterior descending artery, circumflex artery, or right coronary artery) or its branches with a lumen diameter stenosis of ≥70%, along with indications for interventional therapy.24 The exclusion criteria were: (1) patients with severe underlying diseases or major complications; (2) chronic liver disease or abnormal liver function suggestive of hepatic insufficiency; (3) incomplete clinical data; and (4) those diagnosed with COVID-19 (Figure 1).
 |
Figure 1 Inclusion/exclusion flowchart for the study group. |
Data Collection
Venous blood samples were collected within 24 hours of hospital admission, with all samples drawn after fasting for more than 8 hours. If multiple blood tests were performed within the 24-hour window, the results from the first test were used. All laboratory data included in this study were measured by the clinical laboratory of Fujian Medical University Union Hospital, and the data were obtained from the hospital’s electronic medical record system. Baseline data comprised demographic information, admission and discharge diagnoses, laboratory results, medications, surgical procedures, and discharge status.
Definition of the NPS
The NPS is defined based on the levels of serum albumin, total cholesterol, NLR, and LMR.21,25 the scoring system assigns points as follows: a serum albumin level ≥4 mg/dL is assigned 0 points, while <4 mg/dL is assigned 1 point. For total cholesterol, a concentration >180 mg/dL is assigned 0 points, and ≤180 mg/dL is assigned 1 point. A NLR ≤2.96 receives 0 points, while >2.96 is assigned 1 point. For LMR, values >4.44 are given 0 points, and ≤4.44 are assigned 1 point. The NPS total score is calculated as the sum of these parameter scores. Based on the NPS, patients are classified into three groups: low NPS, moderate NPS, and high NPS. The low NPS group has a total score of 0, the moderate NPS group scores between 1 and 2, and the high NPS group scores between 3 and 4. Serum albumin, total cholesterol, NLR and LMR values were calculated from untreated admission reports (Figure 2).26
 |
Figure 2 The formula for the Naples prognostic score. Abbreviation: NPS, Naples Prognostic Score. |
Outcomes Measured
The primary endpoint of this study was the occurrence of MACCEs, which included all-cause in-hospital mortality, new-onset atrial fibrillation (AF), acute myocardial infarction (AMI), and stroke. All-cause in-hospital mortality was defined as death from any cause during hospitalization. New-onset AF was characterized by the absence of prior atrial fibrillation history and was diagnosed through routine electrocardiograms (ECG), Holter monitoring, or bedside ECG monitors during outpatient or inpatient care. AMI was defined as elevated serum cardiac enzyme levels, accompanied by symptoms of myocardial ischemia and hypoxia, along with electrocardiographic changes. The diagnosis of acute myocardial infarction (AMI) is based on elevated cardiac enzyme levels, including troponin I/T (above the 99th percentile) and CK-MB (greater than twice the upper limit of normal), in conjunction with clinical symptoms of myocardial ischemia and electrocardiographic changes, such as ST-segment elevation or new left bundle branch block.27 Stroke diagnosis is based on clinical neurological symptoms (eg, sudden onset of weakness or speech difficulties), confirmed through brain imaging with either CT or MRI. Ischemic stroke is characterized by hypodense areas on CT or hyperintense lesions on diffusion-weighted MRI, while hemorrhagic stroke is diagnosed by the presence of blood on either CT or MRI scans.28 Secondary endpoints included all-cause readmission rates. Readmission events for any cause were confirmed by reviewing medical records or contacting the patient or their treating physician. The average follow-up period for this study was one year.
Statistical Analysis
Continuous variables were presented as weighted means±standard deviations (SD), while categorical variables were expressed as frequencies (percentages). Group differences were assessed using Student’s t-test, Mann–Whitney U-test, and χ²-test, as appropriate. Univariate and multivariate regression analyses, along with Cox proportional hazards models, were employed to evaluate the association between NPS, all-cause mortality, and other adverse outcomes. To reduce potential confounding, sensitivity analyses were performed by adjusting for covariates in a stepwise manner (Model 1–2). Model 1 was adjusted for age and sex, while Model 2 further accounted for smoking history, previous interventions, BMI, hypertension, length of hospital stay, hyperlipidemia, medication use (calcium channel blockers, statins, dual antiplatelet therapy, diuretics), triglycerides, HDL cholesterol, LDL cholesterol, serum potassium, serum sodium, blood glucose, glomerular filtration rate, hemoglobin, total cholesterol (TC), cardiac ejection fraction, and serum creatinine. Time-dependent receiver operating characteristic (ROC) curve analysis and the area under the curve (AUC) were used to assess the accuracy of NPS in predicting all-cause in-hospital mortality risk in coronary artery disease patients. Subgroup analyses explored the association between NPS and mortality, as well as its interaction across different subgroups. In the subgroup analysis, due to the lack of widely accepted standardized cutoff values, all continuous variables were divided based on their median values. All statistical analyses were conducted using SPSS version 26.0, with statistical significance set at P<0.05.
Ethical Approval and Informed Consent
This study received approval from the Ethics Committee of Fujian Medical University Union Hospital (No: 2023KY032). Given that the research solely involved the retrospective collection of anonymized patient data from electronic medical records, the Ethics Committee waived the requirement for informed consent. The use of research data began on May 28, 2023. Throughout the data collection process, the authors did not have access to any information that could identify individual participants. This study adhered to the principles outlined in the revised Declaration of Helsinki from 2013.
Results
Baseline Characteristics of the Study Population
This study included a total of 2,453 patients with an average age of 64.50±10.59 years. Among these patients, 530 (21.6%) were female, 943 (38.4%) had hypertension, and 1,573 (64.1%) had a history of diabetes. Based on the NPS, the patients were categorized into three groups: low NPS (n=177), moderate NPS (n=1,132), and high NPS (n=1,144). From a demographic perspective, patients in the low NPS group generally exhibited higher body mass index (BMI) and ejection fraction, shorter hospital stays, and a lower proportion of prior PCI compared to those in the high NPS group. Additionally, individuals in the low NPS group were less likely to be smokers. In terms of comorbidities, the low NPS group had a lower likelihood of hyperlipidemia and chronic kidney disease. Regarding medication history, patients in the high NPS group were prescribed a greater number of medications, including diuretics, antihypertensives, statins, and dual antiplatelet therapy (DAPT). Biochemical analyses revealed that the low NPS group had higher levels of hemoglobin, serum albumin, total cholesterol, and triglycerides, along with a tendency for elevated high-density lipoprotein (HDL) and low-density lipoprotein (LDL) levels, as well as higher concentrations of serum sodium and potassium. Conversely, the high NPS group exhibited higher serum creatinine (Scr) and blood glucose levels, alongside a lower estimated glomerular filtration rate (eGFR) (Table 1).
 |
Table 1 Baseline Characteristics in Patients with Coronary Heart Disease |
Association Between NPS and the Risk of Adverse Outcomes in Patients with CAD
In the study population, the incidence of MACCEs was relatively high. Specifically, 33 patients (1.3%) experienced all-cause mortality, 845 patients (34.4%) had acute AMI, and 285 patients (11.6%) suffered a stroke (Table 2).
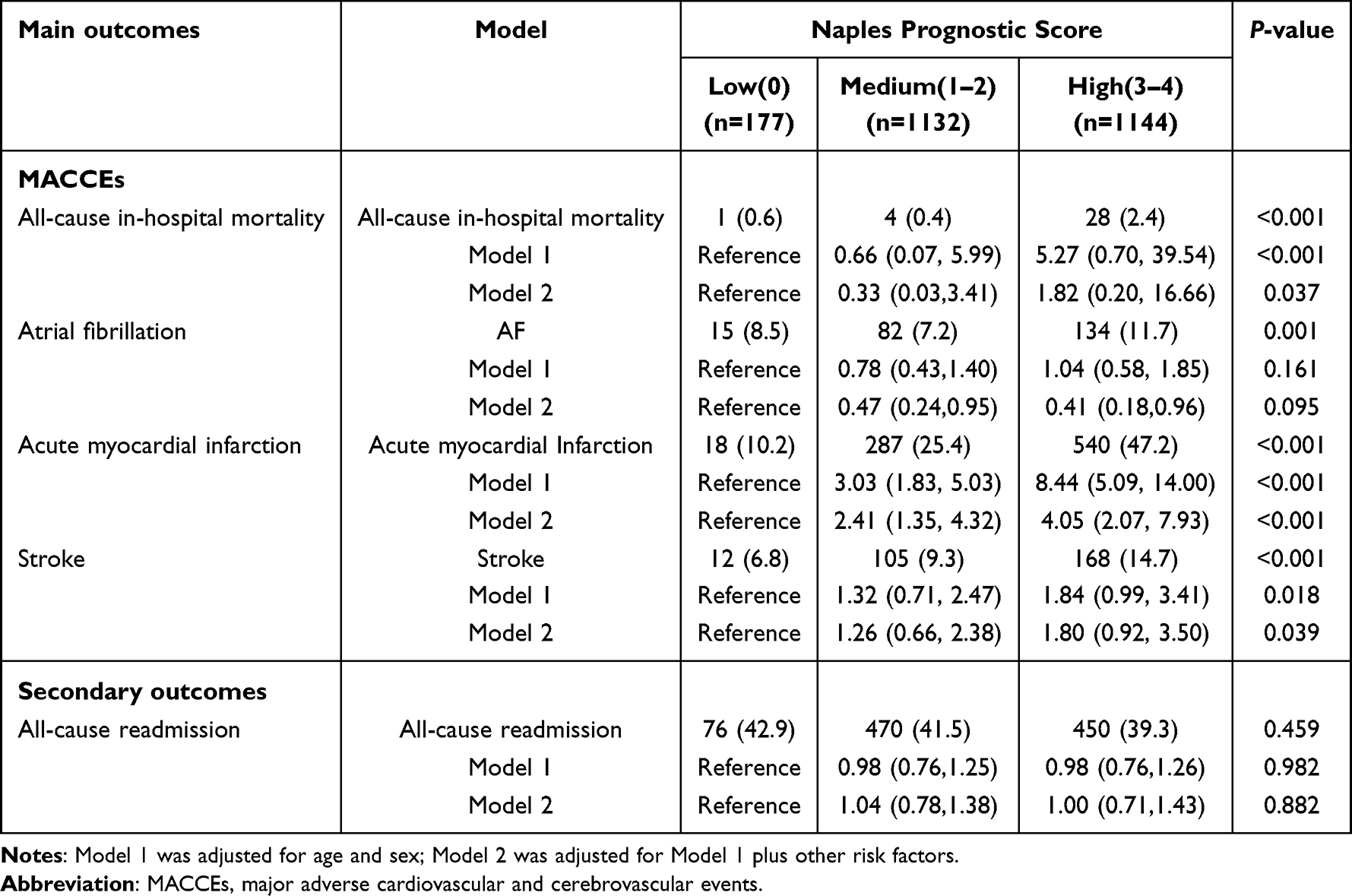 |
Table 2 The Risk of Clinical Outcomes in Patients with Coronary Heart Disease |
The study demonstrated a strong positive association between NPS levels and the risk of all-cause mortality. (P<0.001). In the unadjusted model (Model 1), each unit increase in NPS was associated with a 4.27-fold increase in the risk of all-cause mortality in CAD patients (OR=5.27, 95% CI=0.70–39.54, P<0.001). In the fully adjusted model (Model 2), patients in the high NPS group had an 82% higher risk of all-cause mortality compared to those in the low NPS group (OR=1.82, 95% CI=0.20–16.66, P<0.001). Although we controlled for multiple confounding factors through adjusted analyses, some of the adjusted odds ratios (aORs) exhibit wide 95% confidence intervals due to the limited sample size. This wide confidence interval is typically a result of the small number of death events (Table 2).
Additionally, there was a significant positive association between NPS levels and the risk of acute myocardial infarction (10.2% vs 25.4% vs 47.2%, P<0.001). After adjusting for confounding factors in Model 1, this association remained unchanged, indicating that a higher NPS was associated with an increased risk of AMI. Notably, even after controlling for all confounding factors in Model 2, the association remained statistically significant (OR=4.05, 95% CI=2.07–7.93, P<0.001) (Table 2).
Moreover, NPS levels were independently associated with the risk of stroke, with patients in the high NPS group having the highest risk of stroke, and there was a statistically significant difference between the groups (6.8% vs 9.3% vs 14.7%, P<0.001). After adjusting for confounders in Model 1, it was observed that a higher NPS was associated with an increased risk of stroke. Compared to the low NPS group, the moderate NPS group and high NPS group had a 82% (OR=1.82, 95% CI=0.71–2.47, P<0.05) and 84% (OR=1.84, 95% CI=0.99–3.41, P<0.05) higher risk of all-cause mortality, respectively. After full adjustment for confounders, multivariable logistic regression further confirmed this association. (OR=1.80, 95% CI=0.92–3.50, P<0.05) (Table 2).
It is worth noting that our study found no difference in the risk of atrial fibrillation and all-cause readmission among patients with coronary artery disease across the three different NPS levels. This conclusion was further confirmed after adjusting for confounding factors (P>0.05) (Table 2).
Predictive Value Between NPS and Risk of All-Cause Mortality in Patients with CAD
ROC analysis was used to evaluate the predictive value of the NPS for all-cause mortality in CAD patients. The results demonstrated that NPS could independently predict the risk of all-cause mortality in these patients, with a moderate discriminative ability. The AUC was 0.739 (95% CI, 0.660–0.817, P<0.001) (Figure 3).
 |
Figure 3 Estimation of mortality by ROC curve of NPS. Abbreviations AUC, area under the curve; NPS, Napoli prognostic score; ROC, receiver operating characteristic. |
Subgroup Analysis Between NPS and Risk of Adverse Outcomes in Patients with CAD
A subgroup analysis of high-risk patients for all-cause mortality indicated that statin use was associated with a 6% reduction in the risk of death compared to those not using statins. Furthermore, a left ventricular ejection fraction (LVEF) ≥59.74% was identified as a protective factor against all-cause mortality, whereas a blood glucose level ≥5.48 mmol/L was linked to an increased risk of mortality. Additionally, each extra day of hospitalization was associated with a 4% increase in the risk of all-cause mortality. Elevated serum creatinine levels (≥79 μmol/L) were also found to be a significant risk factor for all-cause mortality (Figure 4).
 |
Figure 4 Forest plot for the effects sizes of individual predictors of all-cause mortality risk in patients with coronary heart disease. |
In the stratified analysis by age, sex, smoking status, and history of hypertension, a significant association was observed between the NPS score and the risk of AMI in CAD patients. Smoking and hyperlipidemia were identified as risk factors for AMI, whereas the use of DAPT, diuretics, a history of chronic heart failure, prior PCI, hospital stays ≥7 days, and LVEF ≥59.74% were found to be protective factors (Figure 5).
 |
Figure 5 Forest plot for the effects sizes of individual predictors of AMI risk in patients with coronary heart disease. Abbreviations: AMI, acute myocardial infarction; DAPT, dual antiplatelet therapy; PCI, percutaneous coronary intervention; EF, ejection fraction. |
Moreover, the association between NPS score and stroke risk remained consistent after subgroup analysis. The analysis of stroke risk factors revealed several key findings. Hyperlipidemia and prior PCI history were not significantly associated with stroke risk. In contrast, the use of CCBs was strongly associated with an increased risk of stroke, suggesting that CCBs may be a significant risk factor. Additionally, a LVEF ≥59.74% was modestly associated with an increased risk of stroke, while age ≥ 65 years showed a consistent, significant increase in stroke risk. These findings highlight the importance of age, LVEF, and CCB use in stroke risk assessment, with age over 65 and CCB use standing out as key risk factors. Further research is needed to explore the underlying mechanisms, particularly regarding CCB use and LVEF in stroke outcomes (Figure 6).
 |
Figure 6 Forest plot for the effects sizes of individual predictors of stroke risk in patients with coronary heart disease. Abbreviations: PCI, percutaneous coronary intervention; CCB, Calcium Channel Blockers; EF, ejection fraction. |
Discussion
To our knowledge, this is the first large-scale study to assess the prognostic value of the novel NPS in patients with acute myocardial infarction. Based on 2,453 CAD cases, our findings suggest that NPS may serve as a practical tool for risk stratification and outcome prediction in this population.
The pathogenesis of CAD mainly involves atherosclerosis and coronary spasm, with atherosclerosis being the key driver.29 Inflammation contributes to plaque formation and poor outcomes.30 NLR and LMR are well-established inflammatory markers for prognosis, but single markers may be affected by confounders.31,32 A combined approach offers better predictive value. Nutritional status also impacts CAD progression. Serum albumin (SA) and TC are linked to disease severity.33,34 Low albumin reflects malnutrition and systemic inflammation and is associated with poor outcomes,35,36 likely due to its anti-inflammatory, antioxidant, and antithrombotic properties.37–41 Elevated TC has also been linked to increased CAD mortality.34 Thus, both serum albumin and TC can serve as indicators of nutritional status in patients with CAD. It is worth noting that, although high TC, particularly LDL-C, is traditionally recognized as a risk factor for cardiovascular disease, decreased TC levels in certain patients may reflect malnutrition or an underlying inflammatory state—both of which are associated with poor prognosis. This paradox is captured in the NPS, where lower TC is associated with higher risk. Recent studies employing modified NPS models, including those involving patients with coronary slow flow, support this interpretation and suggest that in the context of systemic illness, low TC may serve as a marker of vulnerability rather than protection.18
Our study shows that patients in moderate and high NPS groups face increased all-cause mortality risk compared to those in the low NPS group, aligning with previous findings.42,43 This risk may reflect reduced SA and TC, elevated NLR, and decreased LMR—indicating systemic inflammation and poor nutrition. SA, a negative acute-phase reactant, declines during inflammation and is associated with markers like CRP and WBC.44–46 TC also plays a complex role; while generally linked to higher mortality, paradoxically, hypercholesterolemia may lower short-term mortality after myocardial infarction.47 NLR and LMR reflect multiple inflammatory cell types, offering better prognostic accuracy than individual markers.48,49 Although each NPS component has been used to assess STEMI risk, combining them into a single, calculable score may improve short-term mortality prediction. Subgroup analysis further found statin use reduced mortality risk. Statins, as HMG-CoA reductase inhibitors, improve lipid control and plaque stability, contributing to CAD mortality reduction.50,51 These findings emphasize the value of NPS and the need for closer surveillance of high-risk patients.
This study found that AMI incidence increases with higher NPS scores; each one-unit rise in NPS corresponds to a 3.05-fold increased AMI risk in CAD patients. AMI is closely linked to immune and inflammatory responses, with inflammation intensity associated with infarct size and adverse ventricular remodeling.52,53 Malnutrition, common in CAD, is also linked to poor outcomes,54 and low serum albumin reflects both poor nutrition and systemic inflammation in atherosclerosis.55,56 Thus, NPS—a composite of inflammatory and nutritional markers—can be a useful indicator for AMI risk. Interestingly, subgroup analysis revealed that, contrary to conventional expectations, the presence of heart failure appeared to exert a protective effect against AMI. This finding may be partially attributed to the fact that patients with comorbid heart failure often receive more intensive monitoring and timely medical interventions during hospitalization, which could reduce the risk of AMI. In addition, the limited sample size and the heterogeneity of heart failure, including variations between acute and chronic conditions as well as differences in ejection fraction levels, may have influenced the observed outcomes. Further research is needed to investigate the potential mechanisms behind this association.
In our cohort of 2,453 CAD patients, elevated NPS levels were significantly associated with an increased risk of in-hospital stroke. Neuroinflammation plays a key role in stroke pathophysiology, where ischemic injury triggers neuronal death and DAMPs release, activating immune responses and promoting inflammatory cell infiltration into the brain.57–60 Peripheral immune cells, especially lymphocytes, may exert complex effects—some studies suggest neurotoxicity, while others report potential protective roles.61,62 Nutritional status is also closely linked to stroke risk. Cholesterol fluctuations may destabilize atherosclerotic plaques, increasing stroke susceptibility.63 Serum albumin, known for its antioxidant and anti-inflammatory properties, helps maintain vascular volume and reduce cerebral edema, contributing to better stroke outcomes.64,65 Thus, NPS, integrating inflammatory and nutritional markers, may serve as a useful predictor for stroke in CAD patients. Subgroup analysis found short-acting CCB use to be a stroke risk factor. Literature suggests that such formulations can induce reflex sympathetic activation and BP variability, increasing the risk of plaque rupture and subsequent stroke events.66 These findings merit further investigation into the mechanisms linking NPS and stroke risk.
Traditional CAD risk assessment relies on single indicators like blood pressure and cholesterol,67 which may not fully capture a patient’s overall condition. In contrast, the NPS—a composite score based on albumin, cholesterol, NLR, and LMR—offers a more holistic view of inflammatory and nutritional status, both of which are key drivers of CAD progression.11,19 In clinical settings, NPS allows for more accurate risk stratification. High NPS scores identify patients at greater risk, prompting early intervention with anti-inflammatory therapy, nutritional support, and close monitoring. Conversely, patients with low scores may benefit from less intensive management. Beyond prognosis, NPS also informs treatment decisions, as elevated scores are linked to higher readmission and mortality rates. Incorporating NPS into routine assessment may improve outcomes by guiding personalized therapy focused on inflammation and nutrition.
Our study benefits from a large sample size and rigorous adjustment for confounders. As NPS is calculated from routine tests such as blood count, albumin, and cholesterol, it can be easily integrated into primary care workflows, supporting early detection and follow-up of CAD patients in community settings. Nonetheless, several limitations should be considered. First, the retrospective single-center design may introduce residual confounding, even after statistical adjustments. Second, the limited number of mortality events led to wide confidence intervals for some adjusted odds ratios, which may affect the precision of the estimates. Third, the study did not explore the relationship between NPS and other relevant biomarkers that could provide additional insights into underlying mechanisms. Fourth, although the NPS showed prognostic value, it was not directly compared with widely used risk stratification tools such as the GRACE or SYNTAX scores. This is a recognized limitation, and we are currently planning comparative validation studies. Finally, the NPS was assessed only at admission, which restricts interpretation regarding its changes over time and their clinical implications. Further prospective, multicenter research is needed to validate and extend these findings.
Conclusion
The NPS serves as a comprehensive indicator for multidimensional assessments of nutritional and inflammatory status. This study highlights its potential as an easily accessible, cost-effective, and reliable prognostic tool for patients with CAD. These findings provide a valuable addition to existing prognostic indicators for CAD, enhancing risk stratification and improving integrated management strategies. Ultimately, the implementation of NPS may help prevent adverse outcomes in this patient population.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request (Please contact Yanjuan Lin, [email protected]).
Acknowledgments
The authors thank all participants who were involved with this study. All authors approved the submission of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Yan Jiang and Yaqin Chen should be considered joint first authors.
Funding
This study was supported by the fund of the Fifth Batch of Hospital Key Discipline Construction Projects (2022YYZDXK01) of Fujian Medical University Union Hospital.
Disclosure
No potential conflict of interest was reported by the author(s).
References
1. National Center for Cardiovascular Diseases. Report on Cardiovascular Health and Diseases in China 2021. Chinese Circulation Journal. 2022;36:553–578.
2. GBD. 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
3. National Health and Family Planning Commission of China. China Health and Family Planning Statistical Yearbook 2021. Beijing (China): Peking Union Medical College Press; 2022.
4. Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2019 (GBD 2019) Data Resources. IHME. 2019.
5. Testa L, Latib A, Bollati M, et al. Unprotected left main revascularization: percutaneous coronary intervention versus coronary artery bypass. An updated systematic review and meta-analysis of randomised controlled trials. PLoS One. 2017;12(6):e0179060. doi:10.1371/journal.pone.0179060
6. Patel KV, Pandey A, de Lemos JA. Conceptual Framework for Addressing Residual Atherosclerotic Cardiovascular Disease Risk in the Era of Precision Medicine. Circulation. 2018;137(24):2551–2553. doi:10.1161/CIRCULATIONAHA.118.035289
7. Wang HJ, Wang XJ, Ma LJ. Analysis of risk factors for MACE in STEMI patients within one year after PCI. J Yan’an Univ. 2021;19(4):4.
8. Aird WC. Endothelium as an organ system. Crit Care Med. 2004;32(5 Suppl):S271–S279. doi:10.1097/01.CCM.0000129669.21649.40
9. Moore KJ, Tabas I. Macrophages in the pathogenesis of atherosclerosis. Cell. 2011;145(3):341–355. doi:10.1016/j.cell.2011.04.005
10. Wang W, Liang M, Wang L, et al. Role of prostaglandin E2 in macrophage polarization: insights into atherosclerosis. Biochem Pharmacol. 2023;207:115357. doi:10.1016/j.bcp.2022.115357
11. Li X, Ji Y, Kang J, Fang N. Association between blood neutrophil-to-lymphocyte ratio and severity of coronary artery disease: evidence from 17 observational studies involving 7017 cases. Medicine. 2018;97(39):e12432. doi:10.1097/MD.0000000000012432
12. Wada H, Dohi T, Miyauchi K, et al. Pre-procedural neutrophil-to-lymphocyte ratio and long-term cardiac outcomes after percutaneous coronary intervention for stable coronary artery disease. Atherosclerosis. 2017;265:35–40. doi:10.1016/j.atherosclerosis.2017.08.007
13. Chen H, Li M, Liu L, et al. Monocyte/lymphocyte ratio is related to the severity of coronary artery disease and clinical outcome in patients with non-ST-elevation myocardial infarction. Medicine. 2019;98(26):e16267.
14. Song FH, Zheng YY, Tang JN, et al. A Correlation Between Monocyte to Lymphocyte Ratio and Long-Term Prognosis in Patients With Coronary Artery Disease After PCI. Clin Appl Thromb Hemost. 2021;27:1076029621999717. doi:10.1177/1076029621999717
15. Li XT, Fang H, Li D, et al. Association of platelet to lymphocyte ratio with in-hospital major adverse cardiovascular events and the severity of coronary artery disease assessed by the Gensini score in patients with acute myocardial infarction. Chin Med J. 2020;133(4):415–423. doi:10.1097/CM9.0000000000000650
16. Drugescu A, Roca M, Zota IM, et al. Value of the Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio in Predicting CPET Performance in Patients with Stable CAD and Recent Elective PCI. Medicina. 2022;58(6):814. doi:10.3390/medicina58060814
17. Rauchhaus M, Doehner W, Francis DP, et al. Plasma cytokine parameters and mortality in patients with chronic heart failure. Circulation. 2000;102(25):3060–3067. doi:10.1161/01.CIR.102.25.3060
18. Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459–2472. doi:10.1093/eurheartj/ehx144
19. Ma M, Liu Y, Liu F, et al. Relationship Between Prognostic Nutrition Index and New York Heart Association Classification in Patients with Coronary Heart Disease: a RCSCD-TCM Study. J Inflamm Res. 2022;15:4303–4314. doi:10.2147/JIR.S371045
20. Zhang R, Shi S, Chen W, et al. Independent effects of the triglyceride-glucose index on all-cause mortality in critically ill patients with coronary heart disease: analysis of the MIMIC-III database. Cardiovasc Diabetol. 2023;22(1):10. doi:10.1186/s12933-023-01737-3
21. Galizia G, Lieto E, Auricchio A, et al. Naples Prognostic Score, Based on Nutritional and Inflammatory Status, is an Independent Predictor of Long-term Outcome in Patients Undergoing Surgery for Colorectal Cancer. Dis Colon Rectum. 2017;60(12):1273–1284. doi:10.1097/DCR.0000000000000961
22. Jin J, Wang H, Peng F, et al. Prognostic significance of preoperative Naples prognostic score on short- and long-term outcomes after pancreatoduodenectomy for ampullary carcinoma. Hepatobiliary Surg Nutr. 2021;10(6):825–838. doi:10.21037/hbsn-20-741
23. Zhu N, Lin S, Yu H, et al. Naples prognostic score as a novel prognostic prediction indicator in adult asthma patients: a population-based study. World Allergy Organ J. 2023;16(10):100825. doi:10.1016/j.waojou.2023.100825
24. Wang B, Li Y, Han Y. Guidelines for the Diagnosis and Treatment of Stable Coronary Artery Disease. Chin J Cardiovas Dis. 2018;46(09):680–694.
25. Galizia G, Auricchio A, de Vita F, et al. Inflammatory and nutritional status is a predictor of long-term outcome in patients undergoing surgery for gastric cancer. Validation of the Naples prognostic score. Ann Ital Chir. 2019;90:404–416.
26. Li A, He K, Guo D, et al. Pretreatment blood biomarkers predict pathologic responses to neo-CRT in patients with locally advanced rectal cancer. Future Oncol. 2019;15(28):3233–3242. doi:10.2217/fon-2019-0389
27. Thygesen JSA, Jaffe AS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 2018;138(20):e618–651. doi:10.1161/CIR.0000000000000617
28. Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(8):e239.
29. Dong W, Gong Y, Zhao J, et al. A combined analysis of TyG index, SII index, and SIRI index: positive association with CHD risk and coronary atherosclerosis severity in patients with NAFLD. Front Endocrinol. 2024;14:1281839. doi:10.3389/fendo.2023.1281839
30. Fioranelli M, Bottaccioli AG, Bottaccioli F, et al. Stress and Inflammation in Coronary Artery Disease: a Review Psychoneuroendocrineimmunology-Based. Front Immunol. 2018;9:2031. doi:10.3389/fimmu.2018.02031
31. Song S, Chen L, Yu R, et al. Neutrophil-to-lymphocyte ratio as a predictor of all-cause and cardiovascular mortality in coronary heart disease and hypertensive patients: a retrospective cohort study. Front Endocrinol. 2024;15:1442165. doi:10.3389/fendo.2024.1442165
32. Dabla PK, Shrivastav D, Mehra P, et al. Role of lymphocyte-to-monocyte ratio as a predictive marker for diabetic coronary artery disease: a cross-sectional study. World J Methodol. 2024;14(3):92807. doi:10.5662/wjm.v14.i3.92807
33. Hou XZ, Liu EQ, Liu SQ, et al. The negative association between serum albumin levels and coronary heart disease risk in adults over 45 years old: a cross-sectional survey. Sci Rep. 2023;13(1):672. doi:10.1038/s41598-023-27974-w
34. Satoh M, Ohkubo T, Asayama K, et al. A Combination of Blood Pressure and Total Cholesterol Increases the Lifetime Risk of Coronary Heart Disease Mortality: EPOCH-Japan. J Atheroscler Thromb. 2021;28(1):6–24. doi:10.5551/jat.52613
35. Benjamin EJ, Virani SS, Callaway CW, et al. Heart Disease and Stroke Statistics-2018 Update: a Report From the American Heart Association. Circulation. 2018;137(12):e67–e492. doi:10.1161/CIR.0000000000000558
36. Lin Z, Zhao Y, Xiao L, et al. Blood urea nitrogen to serum albumin ratio as a new prognostic indicator in critical patients with chronic heart failure. ESC Heart Fail. 2022;9(2):1360–1369. doi:10.1002/ehf2.13825
37. Arques S. Serum albumin and cardiovascular disease: state-of-the-art review. Ann Cardiol Angeiol. 2020;69(4):192–200. doi:10.1016/j.ancard.2020.07.012
38. Arques S. Human serum albumin in cardiovascular diseases. Eur J Intern Med. 2018;52:8–12. doi:10.1016/j.ejim.2018.04.014
39. Roche M, Rondeau P, Singh NR, et al. The antioxidant properties of serum albumin. FEBS Lett. 2008;582(13):1783–1787. doi:10.1016/j.febslet.2008.04.057
40. Paar M, Rossmann C, Nusshold C, et al. Anticoagulant action of low, physiologic, and high albumin levels in whole blood. PLoS One. 2017;12(8):e0182997. doi:10.1371/journal.pone.0182997
41. Arques S, Ambrosi P. Human serum albumin in the clinical syndrome of heart failure. J Card Fail. 2011;17(6):451–458. doi:10.1016/j.cardfail.2011.02.010
42. Erdoğan O, Erdoğan T, Panç C, et al. Naples prognostic score as a predictor of mortality in surgical aortic valve replacement. Biomarker Med. 2024;18(15–16):675–683. doi:10.1080/17520363.2024.2389035
43. Zhang X, Zhang JK, Wu X, et al. Predictive Value of the Naples Prognostic Score for Cardiovascular Outcomes in Patients With Chronic Kidney Disease Receiving Percutaneous Coronary Intervention. Angiology. 2024. doi:10.1177/00033197241285970
44. Danesh J, Collins R, Appleby P, et al. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: meta-analyses of prospective studies. JAMA. 1998;279(18):1477–1482. doi:10.1001/jama.279.18.1477
45. Don BR, Kaysen G. Serum albumin: relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
46. Oduncu V, Erkol A, Karabay CY, et al. The prognostic value of serum albumin levels on admission in patients with acute ST-segment elevation myocardial infarction undergoing a primary percutaneous coronary intervention. Coron Artery Dis. 2013;24(2):88–94. doi:10.1097/MCA.0b013e32835c46fd
47. Lee KL, Woodlief LH, Topol EJ, et al. Predictors of 30-day mortality in the era of reperfusion for acute myocardial infarction. Results from an international trial of 41,021 patients. GUSTO-I Investigators Circulation. 1995;91(6):1659–1668.
48. Zhang S, Diao J, Qi C, et al. Predictive value of neutrophil to lymphocyte ratio in patients with acute ST segment elevation myocardial infarction after percutaneous coronary intervention: a meta-analysis. BMC Cardiovasc Disord. 2018;18(1):75. doi:10.1186/s12872-018-0812-6
49. Kiris T, Çelik A, Variş E, et al. Association of Lymphocyte-to-Monocyte Ratio With the Mortality in Patients With ST-Elevation Myocardial Infarction Who Underwent Primary Percutaneous Coronary Intervention. Angiology. 2017;68(8):707–715. doi:10.1177/0003319716685480
50. Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339(19):1349–1357. doi:10.1056/NEJM199811053391902
51. Antoniou GA, Hajibandeh S, Hajibandeh S, Vallabhaneni SR, Brennan JA, Torella F. Meta-analysis of the effects of statins on perioperative outcomes in vascular and endovascular surgery. J Vasc Surg. 2015;61(2):519–532.e1. doi:10.1016/j.jvs.2014.10.021
52. Cui Y, Yu Y, Cui Y, et al. The relationship between inflammation, oxidative stress, and acute myocardial infarction and its clinical significance. China Modern Doctor. 2011;49(31):157–158+160.
53. Ong SB, Hernández-Reséndiz S, Crespo-Avilan GE, et al. Inflammation following acute myocardial infarction: multiple players, dynamic roles, and novel therapeutic opportunities. Pharmacol Ther. 2018;186:73–87. doi:10.1016/j.pharmthera.2018.01.001
54. Wada H, Dohi T, Miyauchi K, et al. Prognostic impact of nutritional status assessed by the Controlling Nutritional Status score in patients with stable coronary artery disease undergoing percutaneous coronary intervention. Clin Res Cardiol. 2017;106(11):875–883. doi:10.1007/s00392-017-1132-z
55. Kurtul A, Murat SN, Yarlioglues M, et al. Usefulness of Serum Albumin Concentration to Predict High Coronary SYNTAX Score and In-Hospital Mortality in Patients With Acute Coronary Syndrome. Angiology. 2016;67(1):34–40. doi:10.1177/0003319715575220
56. Suzuki S, Hashizume N, Kanzaki Y, et al. Prognostic significance of serum albumin in patients with stable coronary artery disease treated by percutaneous coronary intervention. PLoS One. 2019;14(7):e0219044. doi:10.1371/journal.pone.0219044
57. Iadecola C, Buckwalter MS, Anrather J. Immune responses to stroke: mechanisms, modulation, and therapeutic potential. J Clin Invest. 2020;130(6):2777–2788. doi:10.1172/JCI135530
58. Jayaraj RL, Azimullah S, Beiram R, et al. Neuroinflammation: friend and foe for ischemic stroke. J Neuroinfla. 2019;16:142.
59. Shi K, Tian DC, Li ZG, et al. Global brain inflammation in stroke. Lancet Neurol. 2019;18(11):1058–1066. doi:10.1016/S1474-4422(19)30078-X
60. Stuckey SM, Ong LK, Collins-Praino LE, et al. Neuroinflammation as a key driver of secondary neurodegeneration following stroke? Int J Mol Sci. 2021;22(23):13101. doi:10.3390/ijms222313101
61. Jones KA, Maltby S, Plank MW, et al. Peripheral immune cells infiltrate into sites of secondary neurodegeneration after ischemic stroke. Brain Behav Immun. 2018;67:299–307. doi:10.1016/j.bbi.2017.09.006
62. Dinkel K, Dhabhar FS, Sapolsky RM. Neurotoxic effects of polymorphonuclear granulocytes on hippocampal primary cultures. Proc Natl Acad Sci USA. 2004;101(1):331–336. doi:10.1073/pnas.0303510101
63. Bangalore S, Breazna A, DeMicco DA, et al. Visit-to-visit low-density lipoprotein cholesterol variability and risk of cardiovascular outcomes: insights from the TNT trial. J Am Coll Cardiol. 2015;65(15):1539–1548. doi:10.1016/j.jacc.2015.02.017
64. Belayev L, Liu Y, Zhao W, et al. Human Albumin Therapy of Acute Ischemic Stroke Marked Neuroprotective Efficacy at Moderate Doses and with a Broad Therapeutic Window. Stroke. 2001;32(2):553–560. doi:10.1161/01.STR.32.2.553
65. Manolis AA, Manolis TA, Melita H, et al. Low serum albumin: a neglected predictor in patients with cardiovascular disease. Eur J Intern Med. 2022;102:24–39. doi:10.1016/j.ejim.2022.05.004
66. Furberg CD, Psaty BM, Nifedipine Meyer JV. Dose‐related increase in mortality in patients with coronary heart disease. Circulation. 1995;92(5):1326–1331. doi:10.1161/01.CIR.92.5.1326
67. Wang N, Mustafa R, Zuber V, Rodgers A, Dehghan A. Association between systolic blood pressure and low-density lipoprotein cholesterol with coronary heart disease according to age. PLoS One. 2023;18(12):e0295004. doi:10.1371/journal.pone.0295004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics, Outcomes and Prognostic Factors for Critical Illness in Hospitalized COVID-19 Patients in Saudi Arabia: A Retrospective Cohort Study
El-Kady AM, Aldakheel FM, Allemailem KS, Almatroudi A, Dbas Alharbi R, Al Hamed H, Alsulami M, Alshehri WA, El-Ashram S, Kreys E, Mohamed K, Al-Megrin WAI, Elshabrawy HA
International Journal of General Medicine 2022, 15:6945-6963
Published Date: 31 August 2022
Systemic Immune-Inflammation Index Predicts Long-Term Outcomes in Patients with Three-Vessel Coronary Disease After Revascularization: Results from a Large Cohort of 3561 Patients
Zhao J, Lv H, Yin D, Zhou X, Zhu H, Guo L, Wang J
Journal of Inflammation Research 2022, 15:5283-5292
Published Date: 12 September 2022
Elevated HsCRP in Chronic Obstructive Pulmonary Disease: A Prospective Study of Long-Term Outcomes After Percutaneous Coronary Intervention
Zheng Y, Qi Y, Seery S, Yang J, Li C, Wang W, Gao J, Meng X, Shao C, Tang YD
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2517-2528
Published Date: 7 October 2022
Association Between Systemic Immune Inflammation Level and Poor Prognosis Across Different Glucose Metabolism Status in Coronary Artery Disease Patients
Xu X, Xie Y, Gu X, Zhou Y, Kang Y, Liu J, Lai W, Lu H, Chen S, Xu J, Lin F, Liu Y
Journal of Inflammation Research 2023, 16:4031-4042
Published Date: 12 September 2023
Discordance Between Neutrophil to Lymphocyte Ratio and High Sensitivity C-Reactive Protein to Predict Clinical Events in Patients with Stable Coronary Artery Disease: A Large-Scale Cohort Study
He J, Song C, Zhang R, Yuan S, Li J, Dou K
Journal of Inflammation Research 2023, 16:5439-5450
Published Date: 20 November 2023