")
Back to Journals » Clinical Ophthalmology » Volume 19
The Relationship of Frailty with Surgical and Laser Treatment for Patients with Glaucoma
Authors Groothoff JD, Rhead JA, Miller IJ, De la Osa ND, Perry JA, Duy WS, Evans JK, Thompson AC
Received 5 January 2025
Accepted for publication 31 March 2025
Published 30 April 2025 Volume 2025:19 Pages 1455—1465
DOI https://doi.org/10.2147/OPTH.S514689
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jonathan D Groothoff,1 James A Rhead,1 Isaiah J Miller,1 Nicholas D De la Osa,1 Jordan A Perry,1 Walter S Duy,1 Joni K Evans,2 Atalie C Thompson1,3
1Department of Ophthalmology, Wake Forest University School of Medicine, Winston-Salem, NC, USA; 2Department of Biostatistics and Data Science, Wake Forest University School of Medicine, Winston-Salem, NC, USA; 3Division of Gerontology and Geriatric Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, USA
Correspondence: Atalie C Thompson, Department of Ophthalmology, Division of Gerontology and Geriatric Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, 27517, USA, Email [email protected]
Introduction: The purpose of this study was to determine whether frailty, quantified by an electronic Frailty Index (eFI), was associated with the likelihood of receiving surgery or laser treatment in patients with glaucoma.
Methods: Single-center retrospective review of patients presenting with glaucoma who had a calculable eFI. A repeated measures multivariable logistic regression model was used to determine the relationship between eFI score and the likelihood of having glaucoma surgery, and a multivariable survival model was also created to assess time to glaucoma surgery. Similar models were constructed for laser treatment (LT). Models were adjusted for age, race/ethnicity, sex, baseline intraocular pressure, and severity based on mean deviation.
Results: A total of 1168 patients (2248 eyes) were included in this study. Glaucoma surgery was significantly more likely among those with severe [OR=2.89] or moderate glaucoma [OR=1.89] (p< 0.001). Older age (per 10 year increase) was associated with a significantly lower likelihood of receiving glaucoma surgery [OR=0.581, p< 0.001], longer times to glaucoma surgery [HR=0.719, p=0.007], and lower likelihood of LT [OR=0.774, p=0.05]. For every 0.1 unit increase in eFI, indicating greater frailty, there was a significantly reduced likelihood of receiving surgical treatment [OR=0.672, p< 0.001], longer time to surgery [HR=0.670, p=0.001], and lower likelihood of LT [OR=0.725, p=0.010], independent of IOP, glaucoma severity, age, sex, or race.
Conclusion: Increased age and frailty scores are associated with reduced likelihood of receiving glaucoma surgery or LT and longer time to glaucoma surgery, even after controlling for baseline IOP and glaucoma severity. Future studies should investigate whether frailty impacts surgical outcomes in glaucoma.
Keywords: frailty, electronic frailty index, glaucoma surgery
Précis
Greater frailty and older age are associated with lower likelihood of receiving glaucoma surgery or laser therapy and longer times to surgical intervention.
Introduction
Glaucoma is a leading cause of irreversible blindness that is estimated to affect 4.2 million people in the United States and 57.5 million people worldwide.1,2 Previous research has highlighted the importance of early intervention in limiting glaucomatous progression.3 Medications that increase trabecular outflow or reduce aqueous fluid production are the first-line therapy, though treatment outcomes often suffer from poor patient adherence.4–6 Laser treatments such as trabeculoplasty, iridotomy, and diode cyclophotocoagulation may also be used as adjunctive therapies to lower intraocular pressure (IOP).5,7–10 In cases of glaucoma that fail to respond to medical management, surgery is often indicated to lower the IOP and decrease risk of progression. Historically, trabeculectomy and tube shunt surgeries have served as the primary surgical procedures for treating glaucoma refractory to medications; however, micro-invasive glaucoma surgeries (MIGS) are increasing in popularity due to their safety and low risk profile.11–13
Frailty is a multidimensional pathological condition affecting older individuals that is characterized by decreased physiological reserve, resulting in an increased susceptibility to adverse health events.14–17 Among older individuals, frailty has been shown to correlate with increased healthcare expenditures and can predict the risk of future hospitalization.18–20 Estimates regarding the prevalence of frailty vary. A meta-analysis by O’Caoimh et al21 reported a pooled prevalence of 24% in patients evaluated through a frailty index, compared to 12% in studies that measured frailty based on phenotypic characterization. In institutionalized populations, up to 68% of patients are estimated to be frail.22 As the population ages, the overall prevalence of frailty is expected to increase.23 Previous studies have evaluated the association between glaucoma prevalence and patient frailty, as well as disease severity, with some studies suggesting a link between frailty and glaucoma risk.24,25 However, limited research describes the influence of frailty on the management of glaucoma.
The purpose of this study was to determine whether frailty, as measured by eFI score, was associated with the likelihood of receiving incisional glaucoma surgery. Laser treatment was evaluated as a secondary outcome. Since older adults who experience frailty may be less inclined to pursue elective treatment and frailty may contribute to the perception of greater patient surgical risk, it was hypothesized that higher eFI scores would be associated with a lower likelihood of incisional glaucoma surgery and laser treatment.
Methods
Study Design
This was a retrospective, single-center cohort study of adult patients who presented to Wake Forest Baptist Medical Center (WFBMC) for treatment of glaucoma between 10/1/2015 and 10/1/2017 and who had a calculable eFI as of 10/1/2017. The starting date was selected to align with our institution’s conversion from ICD-9 to ICD-10 codes on 10/1/2015 and provided the necessary two-year lookback period to calculate eFI scores utilizing ICD-10 codes from at least two outpatient encounters. Wake Forest University Institutional Review Board (IRB) approval was obtained prior to data collection (IRB00079324) and the research process adhered to the standards put forward in the Declaration of Helsinki. A waiver of informed consent was obtained due to the retrospective nature of the study.
Patient Selection and Data Collection
ICD-10 codes H40.0–H40.9 were queried to identify patients with glaucoma. Patient charts and testing were then manually reviewed to determine if patients had glaucomatous optic neuropathy and the presence of a reproducible glaucomatous visual field defect. Individuals were excluded from the study if they did not have a reproducible visual field, a diagnosis of glaucoma, experienced less than two years of follow-up from the date of initial presentation, or lacked a calculable eFI. Patients with ocular hypertension or who were listed as “glaucoma suspect” were not included in this study. Follow-up appointments included any clinic visits with ophthalmologists within the Wake Forest Baptist Health system or satellites whose notes were available in the EMR.
Baseline demographic and ocular characteristics were collected from patient charts, including age, sex, race, baseline intraocular pressure (IOP), and prior glaucoma surgeries. Baseline glaucoma stage was categorized using mean deviation (MD) from Humphrey visual fields (Zeiss Meditec, Inc).: mild (MD ≥ −6 dB), moderate (MD: −6.01 to −12 dB), and severe (MD < −12).26
Numerous tools have been developed in an attempt to operationalize frailty.14 However, these models often rely on self-reported patient data and are thus more difficult to scale.27 Furthermore, these tools may miss subclinical factors that influence patient frailty and drive early intervention.14 To objectively measure frailty, Clegg et al28 developed the electronic Frailty Index (eFI), a validated composite metric within the electronic medical record (EMR) that predicts adverse health outcomes based on 36 functional deficits. This was adapted by Pajewski et al14 and expanded to incorporate 54 deficits from the EMR, including laboratory results, medication records, diagnostic codes, and Medicare Annual Wellness Visit (AWV) data. In this model, a “deficit” refers to a medical characteristic, such as a diagnosis, lab, or medication. Each deficit is binary (present or absent) and possesses equal weight. An eFI score is determined by calculating the ratio of total deficits present to total deficits considered and is reported as a unitless value between 0.1 and 1.0, with higher scores indicating greater frailty. We selected the eFI for this study due to its internal and external validity, varied metrics, and use across diverse research contexts. Previous large-scale studies have employed an eFI to compare differences in diabetes management, inpatient surgical outcomes, and healthcare utilization among various patient populations.29–31 While some frailty indexes within the EMR rely on claims-based data, this approach can be vulnerable to incomplete or delayed data acquisition. The eFI addresses these weaknesses by calculating a frailty score based on data across multiple domains including blood pressure, weight, bone disorders, diabetes, basic metabolic profile results, kidney function, and liver enzyme tests. The eFI was used as a continuous variable in the primary analysis. In addition, categories for frailty were secondarily considered, with patients classified as Fit (eFI ≤ 0.10), Pre-Frail (0.10 < eFI ≤ 0.21), or Frail (eFI > 0.21).14,32
Included patients were followed through June 2024 to determine whether they underwent any subsequent glaucoma surgeries or laser treatments. Treatment characteristics such as the types of surgery, total number of surgeries, and date of a patient’s most recent surgery were then recorded. Surgeries were classified as trabeculectomy, tube, or other, such as goniotomy or concurrent phacoemulsification and MIGS. A person was considered to have had LT if they received any of the following procedures: argon laser trabeculoplasty (ALT), selective laser trabeculoplasty (SLT), laser peripheral iridotomy (LPI), diode cyclophotocoagulation (CPC), and micropulse transscleral cyclophotocoagulation (mTS-CPC). Time to event was determined by calculating the number of days between a patient’s initial presentation with glaucoma and incisional surgery or laser treatment.
Statistical Methods
The associations of eFI score with baseline demographic and clinical characteristics were determined using a Kruskal–Wallis test. Separate mixed effects logistic regression models were used to determine the relationship between baseline eFI and the odds of either incisional glaucoma surgery or LT among glaucoma patients. Separate repeated measures survival models with mixed effects, also known as a frailty model, were created to assess the association between eFI and either the time to incisional glaucoma surgery or the time to laser treatment.
Next, in a sensitivity analysis, we assessed the competing risk of death with regard to the relationship of continuous eFI with time to surgery or time to laser treatment. To do this, it was necessary to first redefine the outcomes as time to first surgery (or first laser treatment) from the earliest presentation. The baseline IOP and glaucoma severity used in these models were selected based on the eye of first surgery or laser treatment; if both eyes had surgery, or if neither eye had surgery, the eye with the most severe glaucoma at initial presentation was selected. In the standard proportional hazards model, if the patient did not have surgery, their time to surgery was censored at either date of death or date of final contact. In the competing risk model, deaths were identified separately from those alive at last contact with no surgery.33
Multivariate models adjusted for baseline age, IOP, sex, race/ethnicity, and glaucoma severity in each eye. Statistical analysis was performed in SAS version 9.4 (SAS Institute Inc., Cary, NC). A p < 0.05 was considered statistically significant.
Results
The initial query identified 1268 patients with glaucoma who presented between 10/1/2015 and 12/31/2017 and possessed a calculable eFI score. After manual review of the EMR to confirm the diagnosis of glaucoma, 1168 patients (2248 eyes; 1080 with both eyes and 88 with one eye) were included in the analysis. Of these, 474 patients (40.6%) were male and 694 patients (59.4%) were female. Table 1 displays the baseline demographic and ocular characteristics of patients. The mean age was 74.0 ± 7.4 years (range: 55–100 years), and 81.3% of patients (n = 949) were between 65 and 85 years of age. Mean and median eFI were greater among female (p = 0.035) and Black patients (p < 0.001). The most common type of glaucoma was primary open-angle glaucoma (88.9%). At initial presentation, 130 eyes had received a prior glaucoma surgery. Baseline IOP, glaucoma type, mean deviation, or previous glaucoma surgery were not associated with differences in eFI score (p > 0.05).
 |
Table 1 Estimated eFI by Patient Characteristics |
During the treatment period, 248 eyes received surgical treatment and 230 eyes were treated with lasers. Trabeculectomy (n = 108) was the most common incisional surgery received, followed by tube shunt (n = 64) and goniotomy (n = 33). The mean time between presentation and glaucoma surgery was 4.5 ± 2.9 years. Selective laser trabeculoplasty (n = 112) and argon laser trabeculoplasty (n = 80) were the most common laser treatments, and mean time to LT was 4.8 ± 3.4 years.
Table 2 displays odds ratios for the likelihood of receiving surgical treatment, and Table 3 displays hazard ratios for time to surgery based on patient characteristics. In multivariable models, an increase in age of 10 years was associated with a significantly decreased likelihood of incisional glaucoma surgery [odds ratio (OR) = 0.581 (95% CI: 0.461, 0.733), p < 0.001] and with significantly longer times to surgery [hazard ratio (HR) = 0.719 (95% CI: 0.554, 0.935), p = 0.007]. For each 1 unit increase in baseline IOP, the likelihood of incisional surgery significantly increased [OR = 1.064 (95% CI: 1.037, 1.092), p < 0.001] and the time to surgery was significantly shorter [HR 1.110 (95% CI: 1.082, 1.138), p < 0.001]. Having severe [OR = 2.889 (95% CI: (1.953, 4.272)] or moderate glaucoma [OR = 1.894 (95% CI: 1.354, 2.650)] also was associated with a significant increase in the likelihood of incisional surgery (p < 0.001), and with a significantly shorter time to surgery relative to patients with mild glaucoma (p < 0.001). Every 0.1 unit increase in eFI was associated with a significantly reduced likelihood of surgical treatment [OR = 0.672, (95% CI: 0.535, 0.845), p < 0.001] and significantly longer time to first surgery after presentation [HR = 0.670 (95% CI: 0.519, 0.866), p = 0.001], independent of IOP, glaucoma severity, age, sex, or race. In a sensitivity analysis, we examined the time to first surgery at the person-level rather than the eye-level using standard proportional hazards [HR = 0.738 (95% CI: 0.592, 0.920), p = 0.007] and refit this model including death as a competing risk [HR = 0.703 (95% CI: 0.565, 0.874), p = 0.002]. In both cases every 0.1 unit increase in eFI was associated with a similarly longer time to first surgery. When examining the categories of eFI, there was no statistically significant difference in likelihood of surgery or time to surgery (see Supplemental Tables 1 and 2).
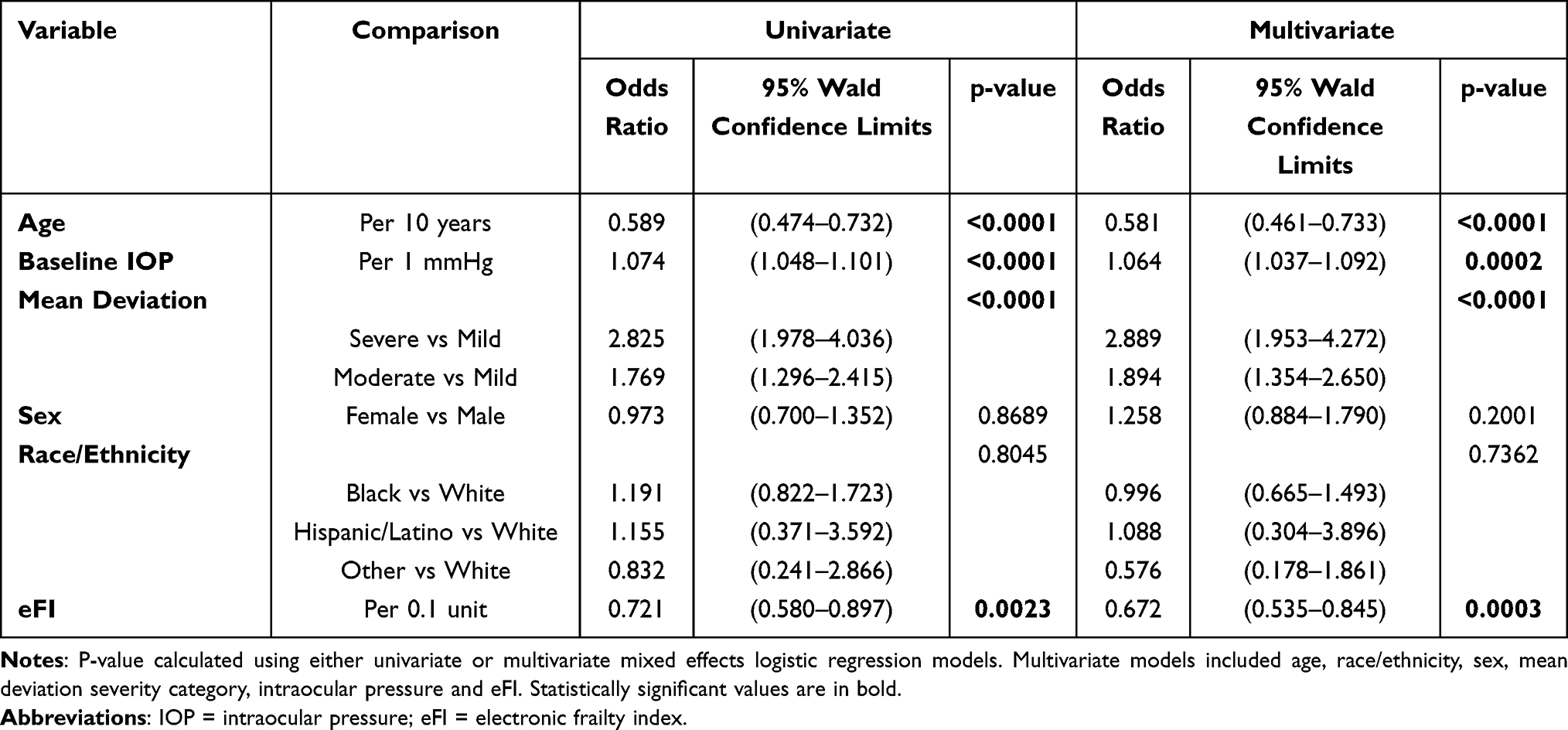 |
Table 2 Repeated Measures Logistic Regression Model for Likelihood of Glaucoma Surgery |
 |
Table 3 Repeated Measures Survival Model for Time to Glaucoma Surgery |
Table 4 and Table 5 display odds ratios and hazard ratios for the secondary outcome of LT. Increased age was associated with a significantly decreased likelihood of receiving LT [OR = 0.774 (95% CI: 0.596, 1.006), p = 0.050] but did not affect time to LT (p = 0.532). Severe [OR = 1.760 (95% CI: 1.076, 2.881)] and moderate [OR = 1.378 (95% CI: 0.867, 2.191)] glaucoma were associated with significantly shorter times to LT (p = 0.041) but had no impact on the likelihood of receiving LT (p = 0.141). Greater eFI was associated with a significantly reduced likelihood of LT [OR = 0.725 (95% CI: 0.561, 0.938), p = 0.010] and slightly longer time to LT [HR = 0.743, p = 0.060], though the latter was not statistically significant. This could be because Frail patients had longer times to LT [HR = 0.617] than Fit patients but Pre-Frail patients [HR = 1.221] had shorter times (p = 0.044). In a sensitivity analysis, we examined the time to first LT at the person-level rather than the eye-level using standard proportional hazards [HR = 0.780 (95% CI: 0.629, 0.967), p = 0.024] and refit this model [HR = 0.747 (95% CI: 0.603, 0.927), p = 0.008], and in both cases every 0.1 unit increase in eFI was associated with a similarly longer time to first LT. There was no significant association of frailty and pre-frailty categories with likelihood of LT (p = 0.053) (see Supplemental Tables 3 and 4).
 |
Table 4 Repeated Measures Logistic Regression Model for Laser Treatment |
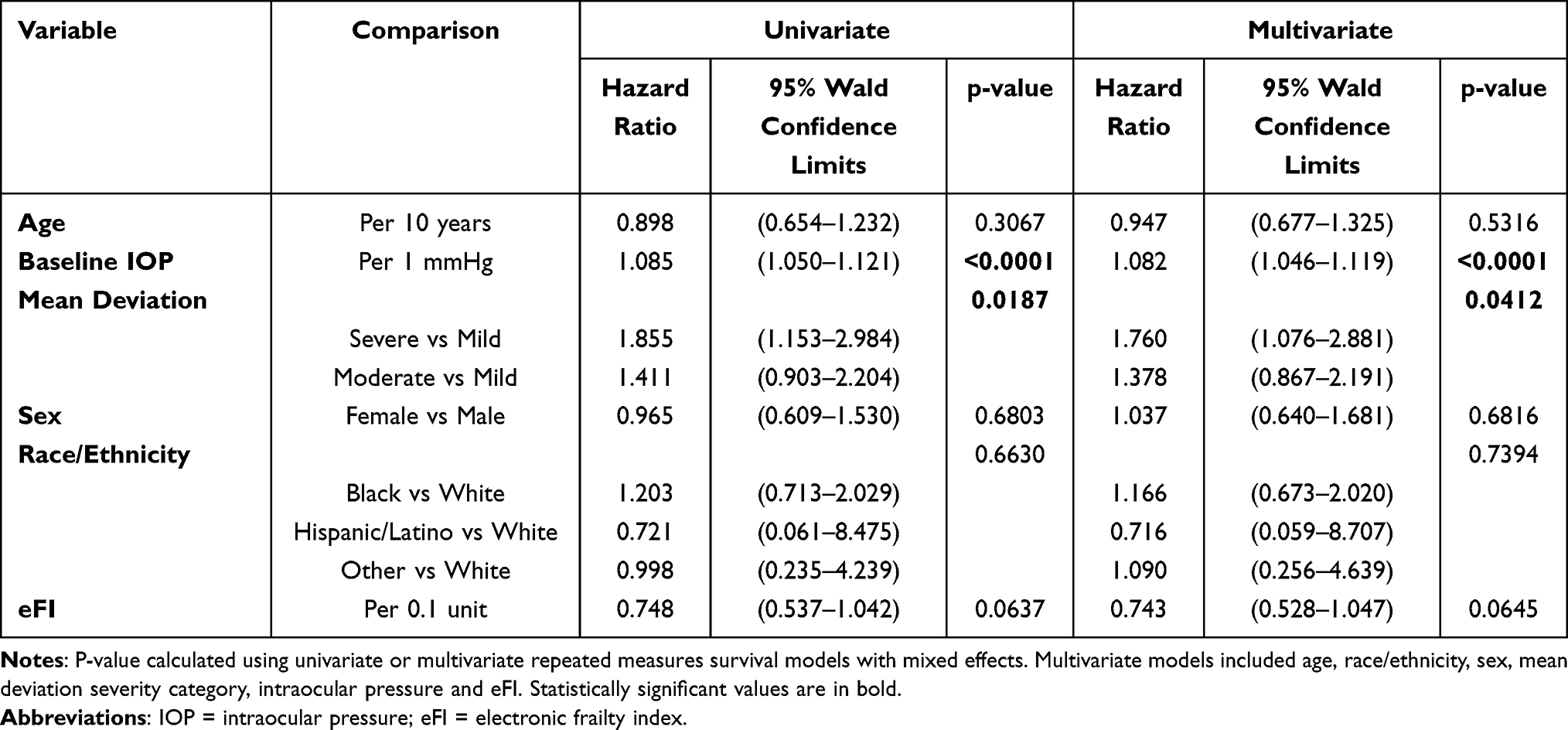 |
Table 5 Repeated Measures Survival Model for Time to Laser Treatment |
Discussion
Few studies have explored the relationship between frailty and surgical or laser treatment of patients with glaucoma. In this study, higher eFI scores were independently associated with a lower likelihood of receiving incisional surgery for glaucoma, even after controlling for other potential confounders. Similar findings were observed for lasers, with higher frailty levels being associated with reduced likelihood of LT. While reasons for this observation are not known and few studies have explored this topic, we hypothesize that this may be related to the perception of higher surgical risks or limited functional improvements among frail individuals. Frail patients are more likely to experience postoperative complications and possess greater mortality rates, even after minimally invasive surgeries.17,27,34–37 Inflammation is also greater in frail patients.38 Previous research has shown that prolonged inflammation and dysregulated macrophage activity delay wound healing, though literature specific to ophthalmic outcomes is limited.39–41 Nevertheless, for ophthalmologists, this increased risk profile may create hesitancy even when considering elective outpatient procedures. We also explored if the higher mortality associated with frailty may explain our main study findings. However, increasing frailty score was also associated with a longer time to first surgery and longer time to first LT even after accounting for the competing risk of death. It is possible that frail individuals may be less likely to pursue elective interventions that are associated with an increased number of follow-up appointments, or may be more hesitant to pursue supplemental procedures, even relatively low-risk outpatient procedures such as laser trabeculoplasty. Ophthalmologists may want to consider goals of care discussions with older adults, especially if frail, to ensure they are taking into account the impact of procedures on their quality of life.
Furthermore, frail patients may face barriers to accessing care, which could include concerns about needing transportation to clinical appointments, especially if visually impaired. Though frailty is associated with more emergency department visits and acute surgeries, primary care services are utilized less often.42 Halawa et al43 found that Medicare beneficiaries classified as moderately or severely frail were more likely to receive ophthalmologic treatment in inpatient settings compared to non-frail patients. This suggests that frail populations are more likely to engage healthcare services during times of urgent need, rather than benefitting from preventative outpatient care focused on limiting chronic disease progression. Ocular changes caused by glaucoma are typically gradual; thus, visual acuity may be preserved until later stages of disease progression, delaying presentation for care.
Our findings also suggest that as patients age, there is a lower likelihood of receiving surgical or laser treatment for glaucoma, even after controlling for eFI, IOP, and glaucoma severity. As glaucoma is a neurodegenerative disease, its prevalence increases with age, which may make this finding seem counterintuitive.44,45 However, we hypothesize that this may be partially related to a trend of the last decade, in which patients are undergoing surgical intervention at younger ages and when they have less advanced disease.46 Potential causes for this shift include earlier detection through advanced imaging modalities such as optical coherence tomography and earlier intervention with safer surgical techniques. Nevertheless, Duman et al47 reported that surgical outcomes following trabeculectomy were comparable between patients younger and older than 80 years, which suggests that age alone should not be a contraindication for surgical treatment. Little work has been done to examine patient or physician factors that may impact decisions for surgical care in glaucoma, especially in older adults, and it will be important to understand how to best support glaucoma patients in these decisions as they age.
We also observed that increasing levels of frailty were associated with a lower likelihood of LT. This was an unexpected finding as LT is a relatively safe, fast, and effective first-line treatment for glaucoma.48–51 Moreover, the LiGHT Trial52 found that SLT not only improved IOP in eyes with open angle glaucoma or ocular hypertension, but also reduced the risk for glaucoma progression and the need for incisional surgery. After six years, 70% of eyes had experienced a 20% or greater reduction in IOP without any use of eye drops. Unsurprisingly, LT is associated with greater benefit for patients with higher baseline IOP and may be particularly effective for patients for who experience barriers to regular monitoring.53,54 As research has shown that frail patients are less likely to receive outpatient care, LT may be a useful approach for early intervention among frail patients with glaucoma. Thus, understanding why frailty is associated with lower likelihood of LT will be important future work.
The results of this study indicate that higher IOP and more severe glaucomatous visual field loss at baseline predict a higher likelihood of receiving surgical treatment, and that those patients experience shorter times to surgery independent of their eFI or other covariates. These findings are not surprising and should be reassuring because patients with more advanced disease or poorly controlled IOP were still more likely to receive timely surgical treatment, which can lower the risk of progression.
The popularity of MIGS has been steadily increasing due to shorter recovery times and fewer complications.11 In our sample, 55 eyes were treated with MIGS. However, trabeculectomy was the most common surgical procedure performed in this study population. Trabeculectomy serves as a definitive surgical treatment for patients with glaucoma that is unresponsive to medications and laser procedures.11 This finding likely reflects the practice pattern at our institution, which is a tertiary referral center where many patients present with moderate and severe glaucoma.
This study has several limitations. As a retrospective review, we were limited by the data type and quality available within patient records. Long-term data quantifying surgical outcomes among patients was not captured but will be the focus of future work. Frailty and other factors such as visual field and intraocular pressure were considered at baseline so we could look at predictions for events like surgery or LT. Consideration of the complex relationship between trends of IOP or frailty over time was beyond the scope of this analysis but could be considered in the future. Finally, while this study did not evaluate appointment frequency, future studies could evaluate whether higher eFI scores are associated with gaps in care for glaucoma.
Conclusions
Increasing frailty, as measured by eFI score, and increasing age are associated with a reduced likelihood of incisional glaucoma surgery and laser treatment, as well as longer time to receiving surgery in patients with glaucoma. Future research should investigate how characteristics like age and frailty influence patient and physician decision making for surgical care of patients with ophthalmologic conditions.
Consent to Participate
IRB approval was obtained from the Wake Forest University Institutional Review Board. As a retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties. The risk of harm or discomfort that might occur as a result of taking part in this research study is not more than in daily life. The rights of subjects were protected through measures to maintain the confidentiality of study information.
Funding
Wake Forest University School of Medicine Medical Student Research Program.
Disclosure
The authors do not report any conflicts of interest.
References
1. Ehrlich JR, Burke-Conte Z, Wittenborn JS, et al. Prevalence of glaucoma among US adults in 2022. JAMA Ophthalmol. 2024;142(11):1046. doi:10.1001/jamaophthalmol.2024.3884
2. Allison K, Patel D, Alabi O. Epidemiology of glaucoma: the past, present, and predictions for the future. Cureus. 2020;12(11):e11686. doi:10.7759/cureus.11686
3. Leske MC, Heijl A, Hyman L, Bengtsson B. Early manifest glaucoma trial: design and baseline data. Ophthalmology. 1999;106(11):2144–2153. doi:10.1016/s0161-6420(99)90497-9
4. Law SK. First-line treatment for elevated intraocular pressure (IOP) associated with open-angle glaucoma or ocular hypertension: focus on bimatoprost. Clin Ophthalmol. 2007;1(3):225–232.
5. Sarenac T, Becic Turkanovic A, Ferme P, Gracner T. A review of selective laser trabeculoplasty: “the hype is real”. J Clin Med. 2022;11(13):3879. doi:10.3390/jcm11133879
6. Reardon G, Kotak S, Schwartz GF. Objective assessment of compliance and persistence among patients treated for glaucoma and ocular hypertension: a systematic review. Patient Prefer Adher. 2011;5:441–463. doi:10.2147/PPA.S23780
7. Garg A, Gazzard G. Selective laser trabeculoplasty: past, present, and future. Eye. 2018;32(5):863–876. doi:10.1038/eye.2017.273
8. The Glaucoma Laser Trial Research Group. The glaucoma laser trial (GLT). 2. Results of argon laser trabeculoplasty versus topical medicines. Ophthalmology. 1990;97(11):1403–1413.
9. Garcia GA, Nguyen CV, Yelenskiy A, et al. Micropulse transscleral diode laser cyclophotocoagulation in refractory glaucoma: short-term efficacy, safety, and impact of surgical history on outcomes. Ophthalmol Glaucoma. 2019;2(6):402–412. doi:10.1016/j.ogla.2019.08.009
10. Bloom PA, Tsai JC, Sharma K, et al. “Cyclodiode”. Trans-scleral diode laser cyclophotocoagulation in the treatment of advanced refractory glaucoma. Ophthalmology. 1997;104(9):1508–1519. discussion 1519-20. doi:10.1016/s0161-6420(97)30109-2
11. Higginbotham EJ, Alexis D. Is newer necessarily better? The evolution of incisional glaucoma surgery over the last 100 years. Am J Ophthalmol. 2018;191:xxv–xxix. doi:10.1016/j.ajo.2018.04.009
12. Khan M, Saheb H, Neelakantan A, et al. Efficacy and safety of combined cataract surgery with 2 trabecular microbypass stents versus ab interno trabeculotomy. J Cataract Refract Surg. 2015;41(8):1716–1724. doi:10.1016/j.jcrs.2014.12.061
13. Ma AK, Lee JH, Warren JL, Teng CC. GlaucoMap - distribution of glaucoma surgical procedures in the United States. Clin Ophthalmol. 2020;14:2551–2560. doi:10.2147/OPTH.S257361
14. Pajewski NM, Lenoir K, Wells BJ, Williamson JD, Callahan KE. frailty screening using the electronic health record within a medicare accountable care organization. J Gerontol Ser A. 2019;74(11):1771–1777. doi:10.1093/gerona/glz017
15. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
16. Robinson TN, Eiseman B, Wallace JI, et al. Redefining geriatric preoperative assessment using frailty, disability and co-morbidity. Ann Surg. 2009;250(3):449–455. doi:10.1097/SLA.0b013e3181b45598
17. Panayi AC, Orkaby AR, Sakthivel D, et al. Impact of frailty on outcomes in surgical patients: a systematic review and meta-analysis. Am J Surg. 2019;218(2):393–400. doi:10.1016/j.amjsurg.2018.11.020
18. Bandeen-Roche K, Seplaki CL, Huang J, et al. Frailty in older adults: a nationally representative profile in the United States. J Gerontol a Biol Sci Med Sci. 2015;70(11):1427–1434. doi:10.1093/gerona/glv133
19. Hoffman GJ, Hays RD, Shapiro MF, Wallace SP, Ettner SL. The costs of fall-related injuries among older adults: annual per-faller, service component, and patient out-of-pocket costs. Health Serv Res. 2017;52(5):1794–1816. doi:10.1111/1475-6773.12554
20. Kinosian B, Wieland D, Gu X, Stallard E, Phibbs CS, Intrator O. Validation of the JEN frailty index in the national long-term care survey community population: identifying functionally impaired older adults from claims data. BMC Health Serv Res. 2018;18(1):908. doi:10.1186/s12913-018-3689-2
21. O’Caoimh R, Sezgin D, O’Donovan MR, et al. Prevalence of frailty in 62 countries across the world: a systematic review and meta-analysis of population-level studies. Age Ageing. 2021;50(1):96–104. doi:10.1093/ageing/afaa219
22. Gonzalez-Vaca J, de la Rica-Escuin M, Silva-Iglesias M, et al. Frailty in INstitutionalized older adults from ALbacete. The final study: rationale, design, methodology, prevalence and attributes. Maturitas. 2014;77(1):78–84. doi:10.1016/j.maturitas.2013.10.005
23. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
24. Shang X, Wu G, Wang W, et al. Associations of vision impairment and eye diseases with frailty in community-dwelling older adults: a nationwide longitudinal study in China. Br J Ophthalmol. 2024;108(2):310–316. doi:10.1136/bjo-2022-322048
25. Chen J, Cao X, Zhuo X, et al. Relationships between frailty and the risk of glaucoma in middle-aged and older adults. Ophthalmol Glaucoma. 2024. doi:10.1016/j.ogla.2024.09.006
26. Susanna R Jr, Vessani RM. Staging glaucoma patient: why and how? Open Ophthalmol J. 2009;3:59–64. doi:10.2174/1874364100903020059
27. Khanna AK, Motamedi V, Bouldin B, et al. Automated electronic frailty index-identified frailty status and associated postsurgical adverse events. JAMA Network Open. 2023;6(11):e2341915. doi:10.1001/jamanetworkopen.2023.41915
28. Clegg A, Bates C, Young J, et al. Development and validation of an electronic frailty index using routine primary care electronic health record data. Age Ageing. 2018;47(2):319. doi:10.1093/ageing/afx001
29. Callahan KE, Clark CJ, Edwards AF, et al. Automated Frailty Screening At-Scale for Pre-Operative Risk Stratification Using the Electronic Frailty Index. J Am Geriatr Soc. 2021;69(5):1357–1362. doi:10.1111/jgs.17027
30. Callahan KE, Lenoir KM, Usoh CO, et al. Using an electronic health record and deficit accumulation to pragmatically identify candidates for optimal prescribing in patients with type 2 diabetes. Diabetes Spectr. 2022;35(3):344–350. doi:10.2337/ds21-0068
31. Lenoir KM, Paul R, Wright E, et al. the association of frailty and neighborhood disadvantage with emergency department visits and hospitalizations in older adults. J Gen Intern Med. 2024;39(4):643–651. doi:10.1007/s11606-023-08503-x
32. Pajewski NM, Williamson JD, Applegate WB, et al. Characterizing frailty status in the systolic blood pressure intervention trial. J Gerontol a Biol Sci Med Sci. 2016;71(5):649–655. doi:10.1093/gerona/glv228
33. Fine JPG, Gray RJ. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J Am Stat Assoc. 1999;94(466):496. doi:10.2307/2670170
34. Shinall MC Jr, Arya S, Youk A, et al. Association of preoperative patient frailty and operative stress with postoperative mortality. JAMA Surg. 2020;155(1):e194620. doi:10.1001/jamasurg.2019.4620
35. George EL, Hall DE, Youk A, et al. Association between patient frailty and postoperative mortality across multiple noncardiac surgical specialties. JAMA Surgery. 2020:e205152. doi:10.1001/jamasurg.2020.5152
36. Hui LT, St Pierre D, Miller RS. Frail patients undergoing optimization before surgery: preliminary results. J Am Coll Surg. 2024;238(4):577–586. doi:10.1097/XCS.0000000000000965
37. Tang VL, Covinsky K. Frailty and surgical decision making. Ann Internal Med. 2016;165(9):669. doi:10.7326/m16-1866
38. Walston J, McBurnie MA, Newman A, et al. Frailty and activation of the inflammation and coagulation systems with and without clinical comorbidities: results from the cardiovascular health study. Arch Intern Med. 2002;162(20):2333–2341. doi:10.1001/archinte.162.20.2333
39. Khanna S, Biswas S, Shang Y, et al. Macrophage dysfunction impairs resolution of inflammation in the wounds of diabetic mice. PLoS One. 2010;5(3):e9539. doi:10.1371/journal.pone.0009539
40. Koh TJ, DiPietro LA. Inflammation and wound healing: the role of the macrophage. Exp Rev Mol Med. 2011;13. doi:10.1017/s1462399411001943
41. Holzer-Geissler JCJ, Schwingenschuh S, Zacharias M, et al. The impact of prolonged inflammation on wound healing. Biomedicines. 2022;10(4):856. doi:10.3390/biomedicines10040856
42. Ge L, Yap CW, Heng BH, Tan WS. Frailty and healthcare utilisation across care settings among community-dwelling older adults in Singapore. BMC Geriatr. 2020;20(1). doi:10.1186/s12877-020-01800-8
43. Halawa OA, Kang J, Parikh AA, et al. Relationship between claims-based frailty index and eye care utilization among medicare beneficiaries with glaucoma. Ophthalmology. 2023;130(6):646–654. doi:10.1016/j.ophtha.2023.01.015
44. Liu B, McNally S, Kilpatrick JI, Jarvis SP, O’Brien CJ. Aging and ocular tissue stiffness in glaucoma. Surv Ophthalmol. 2018;63(1):56–74. doi:10.1016/j.survophthal.2017.06.007
45. Zhang N, Wang J, Li Y, Jiang B. Prevalence of primary open angle glaucoma in the last 20 years: a meta-analysis and systematic review. Sci Rep. 2021;11(1):13762. doi:10.1038/s41598-021-92971-w
46. Palma A, Covello G, Posarelli C, Maglionico MN, Agnifili L, Figus M. Is the advent of new surgical procedures changing the baseline features of patients undergoing first-time glaucoma surgery? J Clin Med. 2024;13(11):3342. doi:10.3390/jcm13113342
47. Duman F, Waisbourd M, Faria B, et al. Trabeculectomy in patients with glaucoma over 80 years of age: relatively short-term outcomes. J Glaucoma. 2016;25(3):e123–7. doi:10.1097/IJG.0000000000000230
48. Young JW, Caprioli J. Laser trabeculoplasty as first-line glaucoma treatment. Lancet. 2019;393(10180):1479–1480. doi:10.1016/S0140-6736(18)32553-4
49. Katz LJ, Steinmann WC, Kabir A, et al. Selective laser trabeculoplasty versus medical therapy as initial treatment of glaucoma: a prospective, randomized trial. J Glaucoma. 2012;21(7):460–468. doi:10.1097/IJG.0b013e318218287f
50. Belitsky Y, Skiljic D, Zetterberg M, Kalaboukhova L. Evaluation of selective laser trabeculoplasty as an intraocular pressure lowering option. Acta Ophthalmol. 2019;97(7):707–713. doi:10.1111/aos.14067
51. Ang M, Tham CC, Sng CCA. Selective laser trabeculoplasty as the primary treatment for open angle glaucoma: time for change? Eye. 2020;34(5):789–791. doi:10.1038/s41433-019-0625-6
52. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Laser in Glaucoma and Ocular Hypertension (LiGHT) trial: six-year results of primary selective laser trabeculoplasty versus eye drops for the treatment of glaucoma and ocular hypertension. Ophthalmology. 2023;130(2):139–151. doi:10.1016/j.ophtha.2022.09.009
53. Hirabayashi M, Ponnusamy V, An J. Predictive factors for outcomes of selective laser trabeculoplasty. Sci Rep. 2020;10(1). doi:10.1038/s41598-020-66473-0
54. Philippin H, Matayan E, Knoll KM, et al. Selective laser trabeculoplasty versus 0·5% timolol eye drops for the treatment of glaucoma in Tanzania: a randomised controlled trial. Lancet Glob Health. 2021;9(11):e1589–e1599. doi:10.1016/s2214-109x(21)00348-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.