")
Back to Journals » Journal of Inflammation Research » Volume 18
The Relationship of Insulin Resistance and Systemic Inflammation with Cardiovascular Outcomes in Non-Diabetic Patients Undergoing Coronary Artery Bypass Grafting
Authors Xie Y, Chen H, Gao Y, He H, Wang Z, Zhang Y, Zhou Q, Liu L, Zheng J
Received 20 February 2025
Accepted for publication 6 June 2025
Published 10 July 2025 Volume 2025:18 Pages 9031—9043
DOI https://doi.org/10.2147/JIR.S514852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yingying Xie,1– 3,* Hao Chen,2,4,* Yanxiang Gao,3 Haoming He,3 Zhe Wang,3 Yaru Zhang,3 Qiaochu Zhou,3 Ling Liu,2 Jingang Zheng1,3
1Department of Cardiology, China-Japan Friendship Hospital (Institute of Clinical Medical Sciences), Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Cardiology, The Second Xiangya Hospital of Central South University, Changsha, People’s Republic of China; 3Department of Cardiology, China-Japan Friendship Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 4Department of Cardiology, The Second Affiliated Hospital of South China University, Hengyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingang Zheng, Department of Cardiology, China-Japan Friendship Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, No. 2 East Yinghua Road, Chaoyang District, Beijing, 100029, People’s Republic of China, Fax +86-010-84205026, Email [email protected] Ling Liu, Department of Cardiovascular Medicine, The Second Xiangya Hospital, Central South University, No. 139 Renmin Road, Changsha, Hunan, 410011, People’s Republic of China, Fax +860731-85295407, Email [email protected]
Background: Insulin resistance (IR) is linked to adverse cardiovascular outcomes, but its mechanisms are not fully understood. This study investigates the relationship between IR and systemic inflammation and evaluates how systemic inflammation affects the correlation between IR and prognosis in non-diabetic patients undergoing coronary artery bypass grafting (CABG).
Methods: This study enrolled 1,658 patients post-CABG. IR was assessed via the estimated glucose disposal rate (eGDR), and systemic inflammation was measured by C-reactive protein (CRP) levels. The correlation between eGDR and CRP was analyzed using linear regression. Associations of eGDR and CRP with major adverse cardiovascular and cerebrovascular events (MACCEs) were evaluated through the Kaplan–Meier method, restricted cubic splines (RCS), and adjusted Cox regression analyses. A novel two-stage regression method for survival data was used in the mediation analysis.
Results: Over a median follow-up period of 60.9 months, 414 MACCEs cases were documented. The RCS analysis revealed an L-shaped association between eGDR and MACCEs with an approximate threshold of 8 mg/kg/min, whereas CRP exhibited a linear positive dose-response relationship with MACCEs. Compared with individuals in the high eGDR and low CRP group (eGDR > 8 and CRP < 3), those in the low eGDR and high CRP group (eGDR ≤ 8 and CRP ≥ 3) showed the highest risk for MACCEs (hazard ratio [HR] = 2.282, 95% confidence interval [CI] 1.749– 2.978). Mediation analysis indicated that CRP levels mediated 12.3% of the correlation between eGDR and MACCEs.
Conclusion: eGDR showed a negative correlation with CRP levels, and their synergistic relationship enhanced the prediction of MACCEs in non-diabetic patients undergoing CABG. Additionally, CRP levels partially mediated the association between eGDR and MACCEs. Anti-inflammatory treatment for non-diabetic individuals with high IR who underwent CABG may offer further benefits.
Keywords: insulin resistance, systemic inflammation, non-diabetic, coronary artery bypass grafting
Introduction
Coronary artery disease (CAD) remained the primary cause of mortality and posed a growing public health challenge globally.1,2 Coronary artery bypass grafting (CABG) served as the cornerstone of CAD management and was preferred for patients with complex CAD, left main disease, or multi-vessel disease.3,4 However, the long-term prognosis post-CABG remained suboptimal. Recent studies demonstrated that bypass grafts had high failure rates, with 3.6% occluding at 5 years and approximately 11% failing at 8 years after CABG.5,6 Consequently, the early identification of high-risk patients and management of pertinent risk factors were critical for improving postoperative outcomes.
Insulin resistance (IR), characterized by diminished responsiveness of target tissues to insulin stimulation,7 was not only recognized as an independent risk factor for atherosclerotic cardiovascular disease8,9 but also associated with elevated susceptibility to adverse cardiovascular events.10 The estimated glucose disposal rate (eGDR), a novel non-insulin-based surrogate marker for IR, integrated blood pressure and waist circumference rather than relying solely on fasting glucose and insulin levels.11,12 This approach provided a more comprehensive assessment of metabolic health compared to traditional measures like glycated hemoglobin (HbA1c)12 or homeostasis model assessment of insulin resistance (HOMA-IR).13 Prior studies indicated that eGDR exhibited stronger predictive power for cardiovascular risk than HbA1c14 or HOMA-IR,13 particularly in non-diabetic populations.15–17 Nevertheless, the prognostic value of eGDR in CAD patients undergoing CABG remained unclear.
Inflammatory response played a pivotal role in CAD pathogenesis.18 C-reactive protein (CRP), a classic inflammatory biomarker, was confirmed as an independent CAD risk factor, with predictive utility comparable to lipid profiles or blood pressure.18,19 Both the Centers for Disease Control and Prevention and the American Heart Association (AHA) recommended CRP > 3.0 mg/L as a high-risk threshold for guiding cardiovascular risk stratification.20,21 Importantly, IR was frequently associated with elevated CRP levels in prior studies,22,23 suggesting potential mechanistic interplay. However, the combined impact of IR and inflammation on cardiovascular outcomes after CABG had not been systematically investigated.
Therefore, in the present study, we sought to investigate the relationship between IR assessed by the eGDR and the inflammation evaluated by CRP levels with long-term cardiovascular outcomes in non-diabetic patients undergoing CABG. Specifically, 1) to evaluate the relationship between eGDR and CRP in non-diabetic individuals undergoing CABG. 2) to examine whether eGDR and CRP have a synergistic effect in predicting the prognosis of CABG patients; 3) to assess whether inflammation mediates the relationship between IR and cardiovascular outcomes.
Methods
Study Population
A total of 1658 patients diagnosed with CAD and undergoing CABG surgery were consecutively enrolled at the Second Xiangya Hospital of Central South University (Changsha, China) from April 2011 to December 2020. The diagnosis of CAD was based on typical angina pectoris, and severe stenosis of ≥1 of the coronary arteries, as indicated by coronary angiography. The exclusion criteria were as follows: 1) a history of diabetes; 2) those aged ≥80 years; 3) patients who underwent aortic valve replacement, mitral valve replacement, aortic root replacement surgery for aortic root aneurysm and aortic dissection, or complex congenital heart disease surgery at the same time; 4) those who died during index hospitalization or within 1 year after discharge; 5) and those lost to follow-up or with missing baseline or follow-up data. This study was approved by the ethics committee of the Second Xiangya Hospital of Central South University and strictly complied with the Declaration of Helsinki, and informed consent was waived due to the retrospective nature of the study and the anonymized processing of patient data.
Data Collection and Definitions
All anthropometric parameters, clinical history, and laboratory test results were acquired from electronic medical records. The anthropometric characteristics included age, sex, body mass index (BMI), waist circumference (WC) and smoking status. The clinical history included hypertension, chronic kidney disease (CKD), diabetes, prior percutaneous coronary intervention (PCI), myocardial infarction (MI) ACS/CCS prevalence and number and types of grafts. Antiplatelet, lipid-lowering, antihypertensive, and antidiabetic medications have also been recorded.
Fasting venous blood samples were collected to measure the plasma levels of hemoglobin, glycosylated hemoglobin A1c (HbA1c), serum creatinine (Scr), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and serum creatinine employing standard laboratory methods. The left ventricular ejection fraction (LVEF) was measured using the two-dimensional modified Simpson’s method.
The diagnosis of CAD was based on typical angina pectoris, and severe stenosis of ≥ 1 of the coronary arteries, as indicated by coronary angiography.24 The identification of diabetes was based on either the self-reported use of antidiabetic medications or elevated blood glucose readings, characterized by casual blood glucose levels of 11.1 mmol/L or higher, fasting blood glucose levels of 7.0 mmol/L or higher, or 2-hour postprandial levels exceeding 11.1 mmol/L following a 75 g oral glucose tolerance test.25 Hypertension was identified through a consistent record of blood pressure readings of 140/90 mmHg or above, or the ongoing use of antihypertensive medication.26
eGDR was determined using the formula: 21.158 - (0.09 × waist circumference [cm]) − (3.407 × hypertension [yes 1 or no 0]) − (0.551 × glycated hemoglobin A1c [HbA1c] [%]).12
Follow-up and Endpoints
The clinical follow‐up data after CABG were collected by reviewing serial records of patients who visited outpatient clinics and telephone interviews with all other patients. The primary end point was major adverse cardiovascular and cerebrovascular events (MACCEs), which were defined as a composite of cardiac death, nonfatal MI, any revascularization, including native coronary arteries and bypass grafts (internal mammary artery, radial artery, and saphenous vein grafts), cardiac rehospitalization (admission because of angina or heart failure), and nonfatal stroke.
Statistical Analysis
Continuous variables were characterized by the mean ± SD or the median with interquartile range (IQR), based on the data’s distribution normality. Group differences were analyzed using t-tests or Mann–Whitney U-tests accordingly. Categorical variables were summarized as frequencies and percentages, and comparisons between groups were performed using the chi-square (χ2) test or Fisher’s exact test. Spearman coefficients and linear regression models were performed to assess the association between eGDR and CRP. The incidence of MACCEs in different groups was assessed by the Kaplan–Meier method based on the eGDR or CRP groups, respectively.
The dose-response association between the eGDR, CRP, and MACCEs in patients after CABG was illustrated through restricted cubic splines (RCS) curve. Cox regression models were employed to assess the relationship between the eGDR, CRP, and the incident MACCEs. Receiver operating characteristic (ROC) curves and the area under the curves (AUC) were constructed to compare the predictive value of eGDR and CRP for MACCEs. Additionally, C-statistics, a net reclassification index (NRI), and an integrated discrimination improvement (IDI) to evaluate the incremental predictive value of the individual and combined eGDR and CRP. Subgroup analyses were conducted to explore whether the predictive utility of the eGDR and CRP remained consistent across patients with diverse demographic characteristics or comorbidities. In mediation analysis, we employed VanderWeele’s two-stage regression method to obtain survival data. Specifically, we utilized Cox proportional hazards regression to analyze the outcome (MACCEs) and linear regression for the mediator (CRP), evaluating the significance of the mediating effect through examination of 1000 bootstrap samples.
In liner and COX regression analysis and mediation analysis, we employed multiple adjusted models, adjusting various covariates independently, to thoroughly evaluate the robustness and reliability of the findings. Model I was adjusted for age and sex. Model II was adjusted for age, sex, CKD, LVEF, smoker, previous MI, previous PCI and SYNTAX scores. Model III was adjusted for age, sex, CKD, LVEF, smoker, previous MI, previous PCI, SYNTAX scores, statins, Aspirin, P2Y12 inhibitors, ACEI/ARB, β-blockers, TC, LDL-C, HDL-C, TG and Scr. The associations were further assessed with the inverse probability of censoring weighted (IPCW) method as a sensitivity analysis.27 In the IPCW model, the probability for predicting complete data was generated based on all non-diabetic patients undergoing CABG regardless of missing data. The results were considered statistically significant when the 2-sided P value was <0.05. R version 4.0.5 (R Foundation for Statistical Computing) in RStudio version 1.1.463 (RStudio, Inc) and Prism version 8.0.2 were used to perform all statistical analyses.
Results
Baseline Characteristics
The final cohort consisted of 1658 participants who were eligible for the final analysis (aged 60.8 ± 8.3 years; 76.7% men). Over a median follow-up period of 60.9 months, 414 MACCEs cases were observed. Baseline characteristics of the study population are presented in Table 1. No significant differences were observed in sex distribution, ACS/CCS prevalence, diabetes markers HbA1c, smoking status, renal function parameters, or perioperative medication use (all P > 0.05). Surgical characteristics including graft numbers and conduit types showed comparable distributions between groups.
 |
Table 1 Baseline Characteristics of Participants Stratified by the Occurrence of MACCEs |
Patients who experienced MACCEs were generally older and exhibited higher levels of BMI, WC, TC, LDL-C, TG, CRP and SYNTAX score and incidence of hypertension (all P < 0.05). They also had significantly lower LVEF, eGDR index and HDL-C level (all P < 0.05).
Association Between eGDR and CRP
Patients were divided into Tertile 1 group (eGDR ≤ 7.36), Tertile 2 group (7.36 < eGDR ≤ 8.78) and Tertile 3 group (eGDR > 8.78) according to eGDR tertiles. The CRP levels decreased with increasing tertiles of eGDR index (Figure 1A). CRP levels were negatively associated with eGDR index (R = -0.45, P < 2.2e−16; Figure 1B). Additionally, regarding linear regression models measuring eGDR as a continuous variable, each SD increment in eGDR was associated with a 0.51 mg/L decrease in CRP levels (95% CI: −0.61– −0.40; P < 0.001) after adjusting for all covariates (Table S1). Likewise, the categorical analysis revealed that, compared with the Tertile1 group, the Tertile3 group was significantly associated with a 1.72 mg/L (95% CI: −2.15 – −1.29; P < 0.001) decrease (Table S1).
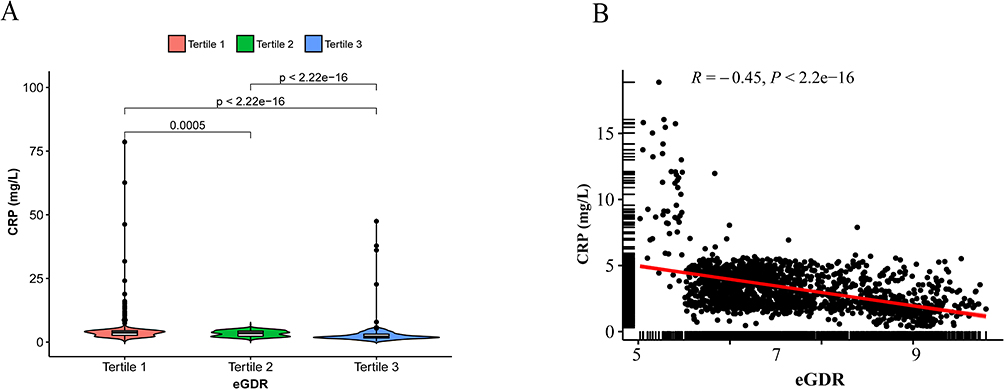 |
Figure 1 Association between eGDR and CRP. (A) Violin plot showing the distribution of CRP among groups categorized by eGDR tertiles; (B) scatter plot. Abbreviations: eGDR, estimated glucose disposal rate; CRP, C-reactive protein. |
Association Between the eGDR Index, CRP Levels, and the Incident MACCEs
Patients were further divided into Tertile1 group (CRP ≤ 2.28 mg/L), Tertile 2 group (2.28 < CRP ≤ 3.87 mg/L) and Tertile 3 group (CRP > 3.87 mg/L) according to CRP tertiles. Kaplan–Meier survival curves of eGDR and CRP for long-term MACCEs are plotted in Figure 2. The MACCEs incidence increased with increasing tertile of the CRP levels and decreasing tertile of eGDR (all log-rank P < 0.001). When analyzed as continuous variables, an decreased eGDR (HR: 0.792, 95% CI: 0.749–0.875, P < 0.001; Table 2) and increased CRP levels (HR: 1.042, 95% CI: 1.029–1.054, P < 0.001; Table S2) were independently associated with MACCEs in the fully adjusted model. Similarly, when analyzed as categorical variables, the Tertile 3 group of eGDR exhibited a lower incidence (HR: 0.523, 95% CI: 0.409–0.668, P < 0.001; Table 2), whereas the Tertile 3 group of CRP showed a higher incidence of MACCEs (HR: 1.747, 95% CI: 1.364–2.238, P < 0.001; Table S2). In the sensitivity analysis considering the potential bias due to missing data of the eGDR or CRP with the IPCW method, the association between the eGDR or CRP and MACCEs remained unchanged (IPCW model in Table 2 and Table S2).
 |
Table 2 Association of the eGDR with the Risk of MACCEs in Non-Diabetic Patients Undergoing CABG |
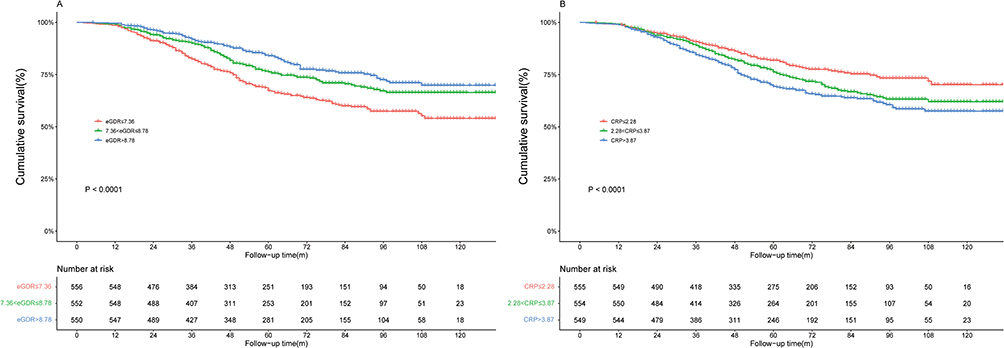 |
Figure 2 Cumulative incidence of MACCEs during follow-up stratified by the eGDR (A) and CRP levels (B). Abbreviations: eGDR, estimated glucose disposal rate; CRP, C-reactive protein; MACCEs, major adverse cardiovascular and cerebrovascular events. |
Subgroup analyses were conducted to assess whether the predictive value of the eGDR and CRP remained consistent across diverse demographic characteristics or comorbidities. After stratifying by sex, age, BMI, hypertension, smoking status and ACS/CCS distribution, both decreased eGDR (Figure S1) and elevated CRP (Figure S2) emerged as significant predictors of MACCEs across various subgroups.
Synergistic Effect of eGDR and CRP on Prediction of Incident MACCEs
According to the RCS analyses, the association between eGDR and MACCEs followed a L-shape and the risk of MACCEs significantly increased when eGDR was lower than 8 mg/kg/min (Figure 3A). While a positive dose–response relationship between the CRP and MACCEs was observed (Figure 3B). To evaluate the addictive effect of eGDR and CRP in predicting MACCEs, the patients were re-categorized by a combination of eGDR (ie 8 mg/kg/min) based on the values obtained by RCS and CRP according to AHA (ie 3 mg/L).21 In comparison with the group with eGDR > 8 and CRP < 3, the group with eGDR ≤ 8 and CRP ≥ 3 had approximately 2.28 times the risk of incident MACCEs (HR: 2.282, 95% CI: 1.749–2.978, P < 0.001; Table 3) after adjusting for all covariates. Sensitivity analysis suggested that the synergistic effect remained unchanged (IPCW model in Table 3). ROC curves of eGDR, CRP, and their combination are plotted in Figure 4. The combination of eGDR and CRP performed better than eGDR (0.645 vs 0.624, P = 0.0382) and CRP (0.645 vs 0.612, P = 0.0251) alone in predicting incident MACCEs. Furthermore, C-statistics, NRI, and IDI were analyzed. Adding eGDR and CRP to the basic model simultaneously further improved C-statistics (0.626, 95% CI: 0.604-0.645 vs 0.556, 95% CI:0.539–0.573, P < 0.001). Additionally, the risk reclassification and discriminatory power also appeared to be substantially better, with an IDI of 0.023 (95% CI: 0.011–0.037; P < 0.001), and a NRI of 0.036 (95% CI: 0.021–0.071; P < 0.001) (Table S3). These findings indicated that combining eGDR and CRP improved the prediction efficiency for MACCEs.
 |
Table 3 Association Between the Combination of the eGDR and CRP and MACCEs in Non-Diabetic Patients Undergoing CABG |
 |
Figure 3 Dose-responsive relationship of eGDR (A) and CRP (B) with the risk of with MACCEs in non-diabetic individuals undergoing CABG. Abbreviations: eGDR, estimated glucose disposal rate; CRP, C-reactive protein; MACCEs, major adverse cardiovascular and cerebrovascular events; CABG, coronary artery bypass grafting; HR, hazard ratio; CI, confidence interval. |
 |
Figure 4 Receiver operating characteristic curves of eGDR, CRP, and their combination in predicting incident MACCEs. Abbreviations: eGDR, estimated glucose disposal rate; CRP, C-reactive protein; MACCEs, major adverse cardiovascular and cerebrovascular events; CABG, coronary artery bypass grafting; AUC, area under curve. |
Mediating Effects of CRP on the Association Between eGDR and Incident MACCEs
As demonstrated in Tables 4 and 5, the mediation analysis revealed that the CRP levels, exerted a significant partial mediating effect on the relationship between IR, as reflected by the eGDR, and the incidence of MACCEs across multiple adjusted models. Specifically, the mediation proportions of an elevated CRP levels were 11.8% (CI: 5.6–17.9%, P < 0.001), 12.8% (CI: 3.0–22.6%, P = 0.011), 12.5% (CI: 2.6–22.4%, P = 0.017) and 12.3% (CI: 3.8–20.8%, P = 0.004) in the crude, adjusted Model I, adjusted Model II, and adjusted Model III, respectively.
 |
Table 4 Decomposition of the Total Association of the eGDR and the Risk of MACCEs in Nondiabetic Patients Undergoing CABG Into Direct and Indirect Associations Mediated by Baseline CRP |
 |
Table 5 Decomposition of the Total Association of the eGDR and the Risk of MACCEs in Non-Diabetic Patients Undergoing CABG Into Direct and Indirect Associations Mediated by Baseline CRP |
Discussion
The principal findings of the present investigation were as follows: 1) eGDR was negatively correlated with plasma CRP levels. 2) A significant association was found between decreased eGDR, elevated CRP levels and a higher incidence of MACCEs post CABG, which remained in different models, sensitivity and subgroup analyses. 3) There was a potential synergistic effect of eGDR and CRP on MACCEs. The combination of eGDR ≤ 8 and CRP ≥ 3 can effectively identify individuals at the highest risk of MACCEs undergoing CABG. 4) Increased CRP levels partly mediated the connection between eGDR and MACCEs, in non-diabetic patient following CABG.
IR is a metabolic disorder significantly related to the occurrence and development of atherosclerotic cardiovascular disease. The current gold standard for analyzing IR is the hyperinsulinemic-euglycemic clamp,28 but it is not suitable for clinical practice and large cohort studies due to its invasiveness and cost. Previous studies have defined insulin resistance using the HOMA-IR index, which is calculated based on fasting glucose and fasting insulin.29 However, routine measurement of fasting insulin levels is not common in standard clinical management of CABG, especially in non-diabetic patients undergoing CABG. eGDR, based on patient’s body size, HbA1c, and presence of hypertension, all of which are included in routine assessments of CAD patients upon hospital admission, is more suitable for secondary prevention in patients following CABG. Sun et al discovered a correlation between eGDR and arterial stiffness and found that it could predict long-term all-cause mortality.30 A large-scale population study emphasized that eGDR can enhance the diagnostic accuracy of ischemic heart disease in the general population.31 In a retrospective study involving non-diabetic patients with non-ST-segment elevation acute coronary syndrome, the findings indicated that low eGDR were a significant risk factor for adverse cardiovascular events.17 Consistent with existing research, this present study illustrated an independent association between a lower eGDR and MACCEs in different models and subgroup analyses in non-diabetic patients after CABG. There was a L-shaped relationship between eGDR and mortality, with cutoff values > 8, which is similar to the cut-values recommended by previous studies for eGDR (<4, 4–6, 6–8, and ≥ 8mg/kg/min).12,32
Atherosclerotic cardiovascular disease has been characterized as a chronic inflammatory condition, highlighting the significant role of inflammation in its pathogenesis and progression. CRP is a systemic inflammatory marker, which activates multiple processes of atherosclerosis, including but not limited to monocyte cytokine expression, adhesion molecule expression, and platelet aggregation.33 Prior studies have demonstrated that the serum CRP levels are higher in patients with acute myocardial infarction patients compared to those with stable angina patient, and CAD patients with higher concentrations of CRP have poorer cardiovascular prognosis.34,35 In line with these findings, an significantly positive association between CRP levels and MACCEs in different models and subgroup analyses was observed. While CRP served as a pragmatic marker of systemic inflammation in this cohort, emerging biomarkers like growth differentiation factor-15 (GDF-15)36 and lipoprotein-associated phospholipase A2 (Lp-PLA2),37 which directly reflect plaque vulnerability and vascular stress-merit investigation in future studies to unravel tissue-specific inflammatory mechanisms underlying IR-driven cardiovascular risk.
IR plays a crucial role as a potential mechanism for increasing CVD risk by activating inflammation-related genes and lead to chronic inflammation, thereby impairing vascular health and promoting CVD.38 A cross-sectional study showed that serum high sensitive CRP was positively correlated with HbA1c and HOMA-IR in patients with subclinical atherosclerosis.39 Similarly, we found a significantly negative correlation between eGDR and CRP in non-diabetic individuals following CABG.
Additionally, in our study, we observed the synergistic effects of eGDR and CRP on long-term MACCEs. Combining them may help further risk stratification for non-diabetic individuals undergoing CABG. The ROC curve demonstrated that the predicting ability for MACCEs using a combination of the eGDR and CRP is greater than that of either index alone. This phenomenon arises from the eGDR index primarily evaluating insulin resistance levels, while CRP reflects factors such as inflammatory burden, thereby resulting in a complementary effect. Consistent with our findings, Li et al reported that IR and systemic inflammation synergistically increase the risk of cardiovascular events in patients with chronic coronary syndrome.40
More importantly, this study clarified the mediating role of CRP levels in linking the eGDR to MACCEs, consolidating previous findings into a comprehensive pathway to guide clinical decision-making. To our knowledge, this study is the first evidence on the causal pathways of insulin resistance, inflammatory markers, and cardiovascular adverse outcomes in non-diabetic patients undergoing CABG. Despite the precise mechanism of mediation interaction remaining unclear, some previous studies provided valuable mechanistic insights. Prior studies suggested that systemic inflammation partially mediates the association between IR and clinical outcomes.40,41 These observational findings provide epidemiological evidence supporting the biologically plausible notion that inflammation could serve as a mediator in the association between IR and adverse outcomes.42 Mechanistically, IR can activate the NOD-like receptor protein 3 inflammasome, which is a key component in the pathogenesis of atherosclerosis, and CRP is a downstream marker.43 Therefore, IR, represented by decreased eGDR, might exacerbate atherosclerosis by up-regulating the NLRP3 signaling pathway, represented by CRP. Additional research is warranted to investigate the potential mechanisms that underlie the causal relationship between eGDR and cardiovascular events. Clinical trials have demonstrated the potential of anti-inflammatory therapy in improving cardiovascular outcomes in secondary prevention of CAD.44,45 However, incorporating anti-inflammatory therapy into CAD management still poses challenges. One obstacle is the need for more precise risk stratification to enhancing cost-effectiveness. This study proposes that utilizing eGDR and CRP in combination can aid in identifying patients at significantly elevated cardiovascular risk. Furthermore, the relationship between low eGDR and adverse cardiovascular outcomes may be mediated by CRP. In addition to directly reducing systemic inflammation, anti-inflammatory treatment targeting these individuals may offer additional benefits, including reducing the synergistic and mediating effects of inflammation on the adverse outcomes of IR.
Limitation
Although offering valuable insights, this study also presents limitations that require thoughtful consideration. First, exclusion criteria for the study included patients without data for the eGDR and CRP, potentially introducing selection bias. Nevertheless, sensitivity analyses utilizing IPCW methods to address missing data yielded results consistent with the primary findings. Second, the limitation of a single-center observational design hinders our ability to establish causal relationships between the eGDR, CRP levels, and MACCEs post-CABG. Third, while many important confounding factors were considered in the multivariable analysis, the impact of unmeasured or unknown confounders on outcomes cannot be entirely ruled out. Forth, the eGDR and CRP data were mostly obtained upon patient admission, thus we were unable to ascertain the impact of dynamic changes in eGDR and CRP on prognosis. Finally, although our study reveals an inverse association between eGDR and CRP levels, future human studies using direct IR measurements (eg, hyperinsulinemic-euglycemic clamps) and other inflammatory marker assessments (eg, GDF-15, Lp-PLA2, interleukin-6) are needed to determine whether IR drives inflammation.
Data Sharing Statement
The dataset analyzed during the current study is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the ethics committee of Second Xiangya Hospital of Central South University, with a waiver of informed consent.
Acknowledgments
Yingying Xie and Hao Chen are co-first authors for this study. The authors would like to acknowledge the patient participants and their relatives, the clinical and research teams, and the nursing teams at all hospitals for their contribution to the study without financial compensation.
Funding
This work was supported by National High Level Hospital Clinical Research Funding (2024-NHLHCRF-YS-01). National Natural Science Foundation of China (No. 82270352). National High Level Hospital Clinical Research Funding (2024-NHLHCRF-JBGS-WZ-06). National Key Clinical Specialty Construction Project (No. 2020-QTL-009). National High Level Hospital Clinical Research Funding (2023-NHLHCRF-YXHZ-ZRMS-09).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
2. Vos T, Lim SS, Abbafati C, et.al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
3. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165. doi:10.1093/eurheartj/ehy394
4. Mohr FW, Morice M-C, Kappetein AP, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet. 2013;381(9867):629–638. doi:10.1016/S0140-6736(13)60141-5
5. Kim MS, Hwang HY, Kim JS, et al. Saphenous vein versus right internal thoracic artery as a Y-composite graft: five-year angiographic and clinical results of a randomized trial. J Thorac Cardiovasc Surg. 2018;156(4):1424–1433.e1. doi:10.1016/j.jtcvs.2018.04.123
6. Xenogiannis I, Zenati M, Bhatt DL, et al. Saphenous vein graft failure: from pathophysiology to prevention and treatment strategies. Circulation. 2021;144(9):728–745. doi:10.1161/CIRCULATIONAHA.120.052163
7. Defronzo RA, Lecture B. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773–795. doi:10.2337/db09-9028
8. Devesa A, Fuster V, Vazirani R, et al. Cardiac insulin resistance in subjects with metabolic syndrome traits and early subclinical atherosclerosis. Diabetes Care. 2023;46(11):2050–2057. doi:10.2337/dc23-0871
9. Iglesies-Grau J, Garcia-Alvarez A, Oliva B, et al. Early insulin resistance in normoglycemic low-risk individuals is associated with subclinical atherosclerosis. Cardiovasc Diabetol. 2023;22(1):350. doi:10.1186/s12933-023-02090-1
10. Laakso M, Kuusisto J. Insulin resistance and hyperglycaemia in cardiovascular disease development. Nat Rev Endocrinol. 2014;10(5):293–302. doi:10.1038/nrendo.2014.29
11. Williams KV, Erbey JR, Becker D, et al. Can clinical factors estimate insulin resistance in type 1 diabetes? Diabetes. 2000;49(4):626–632. doi:10.2337/diabetes.49.4.626
12. Zabala A, Darsalia V, Lind M, et al. Estimated glucose disposal rate and risk of stroke and mortality in type 2 diabetes: a nationwide cohort study. Cardiovasc Diabetol. 2021;20(1):202. doi:10.1186/s12933-021-01394-4
13. Epstein EJ, Osman JL, Cohen HW, et al. Use of the estimated glucose disposal rate as a measure of insulin resistance in an urban multiethnic population with type 1 diabetes. Diabetes Care. 2013;36(8):2280–2285. doi:10.2337/dc12-1693
14. Helliwell R, Warnes H, Kietsiriroje N, et al. Body mass index, estimated glucose disposal rate and vascular complications in type 1 diabetes: beyond glycated haemoglobin. Diabet Med. 2021;38(5):e14529. doi:10.1111/dme.14529
15. Zhang Z, Zhao L, Lu Y, et al. Insulin resistance assessed by estimated glucose disposal rate and risk of incident cardiovascular diseases among individuals without diabetes: findings from a nationwide, population based, prospective cohort study. Cardiovasc Diabetol. 2024;23(1):194. doi:10.1186/s12933-024-02256-5
16. Kim MJ, Cho YK, Kim EH, et al. Association between estimated glucose disposal rate and subclinical coronary atherosclerosis. Nutr Metab Cardiovasc Dis. 2024.
17. Liu C, Liu X, Ma X, et al. Predictive worth of estimated glucose disposal rate: evaluation in patients with non-ST-segment elevation acute coronary syndrome and non-diabetic patients after percutaneous coronary intervention. Diabetol Metab Syndr. 2022;14(1):145. doi:10.1186/s13098-022-00915-9
18. Attiq A, Afzal S, Ahmad W, et al. Hegemony of inflammation in atherosclerosis and coronary artery disease. Eur J Pharmacol. 2024;966:176338. doi:10.1016/j.ejphar.2024.176338
19. Kaptoge S, et al. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet. 2010;375(9709):132–140.
20. Duffy JR, Salerno M. New blood test to measure heart attack risk: c-reactive protein. J Cardiovasc Nurs. 2004;19(6):425–429. doi:10.1097/00005082-200411000-00016
21. Sabatine MS, Morrow DA, Jablonski KA, et al. Prognostic significance of the centers for disease Control/American Heart association high-sensitivity C-reactive protein cut points for cardiovascular and other outcomes in patients with stable coronary artery disease. Circulation. 2007;115(12):1528–1536. doi:10.1161/CIRCULATIONAHA.106.649939
22. Shahid R, Chu LM, Arnason T, et al. Association between insulin resistance and the inflammatory marker c-reactive protein in a representative healthy adult Canadian population: results from the Canadian health measures survey. Can J Diabetes. 2023;47(5):428–434. doi:10.1016/j.jcjd.2023.03.006
23. Meshkani R, Adeli K. Hepatic insulin resistance, metabolic syndrome and cardiovascular disease. Clin Biochem. 2009;42(13–14):1331–1346. doi:10.1016/j.clinbiochem.2009.05.018
24. Tang L, Chen H, Hu X-Q, et al. Intensive lipid-lowering therapy as per the latest dyslipidemia management guideline in predicting favorable long-term clinical outcomes in patients undergoing coronary artery bypass grafting: a retrospective cohort study. J Am Heart Assoc. 2023;12(20):e029397. doi:10.1161/JAHA.123.029397
25. ElSayed NA, Aleppo G, Aroda VR, et al. 2. classification and diagnosis of diabetes: standards of care in Diabetes—2023. Diabetes Care. 2023;46(Suppl. 1):S19–S40. doi:10.2337/dc23-S002
26. Mancia G, Kreutz R, Brunström M, et al. 2023 ESH guidelines for the management of arterial hypertension the task force for the management of arterial hypertension of the European Society Of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. 2023;41(12):1874–2071. doi:10.1097/HJH.0000000000003480
27. Mansournia MA, Altman DG. Inverse probability weighting. BMJ. 2016;352:i189. doi:10.1136/bmj.i189
28. DeFronzo RA, Tobin JD, Andres R. Glucose clamp technique: a method for quantifying insulin secretion and resistance. Am J Physiol. 1979;237(3):E214–23. doi:10.1152/ajpendo.1979.237.3.E214
29. Guerrero-Romero F, Simental-Mendia LE, Gonzalez-Ortiz M, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–3351. doi:10.1210/jc.2010-0288
30. Sun J, Wang N, Li S, et al. Estimated glucose disposal rate and risk of arterial stiffness and long-term all-cause mortality: a 10-year prospective study. J Epidemiol Community Health. 2023;78(3). doi:10.1136/jech-2023-220664.
31. Xuan J, Juan D, Yuyu N, et al. Impact of estimated glucose disposal rate for identifying prevalent ischemic heart disease: findings from a cross-sectional study. BMC Cardiovasc Disord. 2022;22(1):378. doi:10.1186/s12872-022-02817-0
32. Nyström T, Holzmann MJ, Eliasson B, et al. Estimated glucose disposal rate predicts mortality in adults with type 1 diabetes. Diabetes Obes Metab. 2018;20(3):556–563. doi:10.1111/dom.13110
33. Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999;340(2):115–126. doi:10.1056/NEJM199901143400207
34. Mauriello A, Sangiorgi G, Fratoni S, et al. Diffuse and active inflammation occurs in both vulnerable and stable plaques of the entire coronary tree: a histopathologic study of patients dying of acute myocardial infarction. J Am Coll Cardiol. 2005;45(10):1585–1593. doi:10.1016/j.jacc.2005.01.054
35. Stefanadis C, Diamantopoulos L, Dernellis J, et al. Heat production of atherosclerotic plaques and inflammation assessed by the acute phase proteins in acute coronary syndromes. J Mol Cell Cardiol. 2000;32(1):43–52. doi:10.1006/jmcc.1999.1049
36. Wang D, Day EA, Townsend LK, et al. GDF15: emerging biology and therapeutic applications for obesity and cardiometabolic disease. Nat Rev Endocrinol. 2021;17(10):592–607. doi:10.1038/s41574-021-00529-7
37. Pantazi D, Tellis C, Tselepis AD. Oxidized phospholipids and lipoprotein-associated phospholipase A(2) (Lp-PLA(2)) in atherosclerotic cardiovascular disease: an update. Biofactors. 2022;48(6):1257–1270. doi:10.1002/biof.1890
38. Chen W, Wang X, Chen J, et al. Household air pollution, adherence to a healthy lifestyle, and risk of cardiometabolic multimorbidity: results from the China health and retirement longitudinal study. Sci Total Environ. 2023;855:158896. doi:10.1016/j.scitotenv.2022.158896
39. Lachine NA, Elnekiedy AA, Megallaa MH, et al. Serum chemerin and high-sensitivity C reactive protein as markers of subclinical atherosclerosis in Egyptian patients with type 2 diabetes. Ther Adv Endocrinol Metab. 2016;7(2):47–56. doi:10.1177/2042018816637312
40. Li T, Wang P, Wang X, et al. Inflammation and insulin resistance in diabetic chronic coronary syndrome patients. Nutrients. 2023;15(12).
41. Jin A, Wang S, Li J, et al. Mediation of systemic inflammation on insulin resistance and prognosis of nondiabetic patients with ischemic stroke. Stroke. 2023;54(3):759–769. doi:10.1161/STROKEAHA.122.039542
42. Lee DY, Rhee E-J, Chang Y, et al. Impact of systemic inflammation on the relationship between insulin resistance and all-cause and cancer-related mortality. Metabolism. 2018;81:52–62. doi:10.1016/j.metabol.2017.11.014
43. Hartge MM, Unger T, Kintscher U. The endothelium and vascular inflammation in diabetes. Diab Vasc Dis Res. 2007;4(2):84–88. doi:10.3132/dvdr.2007.025
44. Ridker PM. The time to initiate anti-inflammatory therapy for patients with chronic coronary atherosclerosis has arrived. Circulation. 2023;148(14):1071–1073. doi:10.1161/CIRCULATIONAHA.123.066510
45. Zhang FS, He Q-Z, Qin CH, et al. Therapeutic potential of colchicine in cardiovascular medicine: a pharmacological review. Acta Pharmacol Sin. 2022;43(9):2173–2190. doi:10.1038/s41401-021-00835-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.