")
Back to Journals » Clinical Ophthalmology » Volume 18
Translation, Evaluation and Validation of the Adult Strabismus −20 (AS-20) Questionnaire in Swedish
Authors Havstam Johansson L, Levinsson A, Flodin SM
Received 11 July 2024
Accepted for publication 23 October 2024
Published 7 December 2024 Volume 2024:18 Pages 3615—3625
DOI https://doi.org/10.2147/OPTH.S477032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lena Havstam Johansson,1,2 Anna Levinsson,3,4 Sara M Flodin1,2
1Department of Clinical Neuroscience, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 2Department of Ophthalmology, Sahlgrenska University Hospital, Region Västra Götaland, Mölndal, Sweden; 3Department of Epidemiology, Biostatistics, and Occupational Health, Faculty of Medicine, McGill University, Montreal, QC, Canada; 4Department of Social Medicine and Public Health, Sahlgrenska Academy, GothenburgUniversity, Gothenburg, Sweden
Correspondence: Sara M Flodin, Department of Clinical Neuroscience Institute of Neuroscience and Physiology The Sahlgrenska Academy, University of Gothenburg, Gothenburg, SE-431 80, Sweden, Tel +46 721-470080, Email [email protected]
Purpose: To translate and validate the Adult Strabismus 20 (AS-20) questionnaire, a health-related quality of life questionnaire specifically devised for patients with strabismus.
Methods: The AS-20 was translated in accordance with the principles of good practice for the translation and cultural adaptation process for patient-related outcomes (PRO) according to the methodology recommended by the International Society for Pharmacoeconomics and Outcome Research (ISPOR). The translation, evaluation, and validation were performed in several steps. The study used both qualitative and quantitative methods and engaged 31 final-year orthoptic students in workshops, as well as 19 experts (experienced clinical orthoptists), 17 laymen (members of the public), and 17 patients from national eye clinics. The final translated questionnaire was tested for reliability and validity in 68 adults with strabismus by internal consistency using Cronbach´s alpha and content and construct validity using the Rasch analysis.
Results: The Swedish AS-20 showed a high level of internal consistency. Cronbach´s alpha was 0.95 for the psychosocial subscale and 0.92 for the functional subscale. However, the Rasch analysis indicated that both items and responses should be condensed to achieve content and construct validity.
Conclusion: The thorough translation and evaluation process resulted in a validated AS-20 questionnaire for use in the Swedish language, and shows reliability as an instrument to measure health-related quality of life (HRQoL) in adults with strabismus in a clinical setting.
Keywords: health related quality of life, patient reported outcome measures, AS-20, strabismus
Introduction
Questionnaires on health-related quality of life (HRQoL) play an important role in healthcare and may aid clinical decision making through evidence-based practice. A person-reported outcome provides a statistical assessment of Quality of Life (QoL). The assessment of health outcomes emphasizes understanding an individual’s QoL in relation to health issues. QoL instruments can be applied in various settings including healthcare services in hospitals and research environments. In healthcare environments, these instruments aid in symptom relief, care, rehabilitation, and communication with patients and their families. In research, they facilitate comparisons between study treatments.1
Strabismus is a condition with significant impact on QoL.2 Individuals with strabismus may experience both functional and psychosocial difficulties depending on the symptoms experienced. Common issues include inability to perform everyday activities, diplopia (double vision), and self-consciousness regarding appearance.3–5 Application of HRQoL instruments in the evaluation, diagnosis, and treatment of patients with strabismus is important.6
The Adult Strabismus Quality of Life Questionnaire (AS-20) is a patient-derived instrument designed for individuals with strabismus. It was developed through individual patient interviews and generated 181 questionnaire items that were reduced through factor analysis.7 This procedure identified two prominent factors, and the 10 items with the highest correlation with each factor were selected, resulting in a final 20-item questionnaire with two subscales (psychosocial and functional) containing 10 statements each (see Appendix 1). The self-administered questionnaire asks patients to rate their agreement with the proposed statements on a 5-point Likert-type scale (“never”=100, “rarely”=75, ‘sometimes’=50, “often”=25, and ‘always’=0). The overall score is then calculated as the mean of the completed items, and a low overall score indicates a low HRQoL. The threshold for a normal non-strabismic score is 84.8 Traditionally, scores for two distinct domains (psychosocial Q1-10 and functional Q11-20) are calculated as the mean of the completed items within each subscale. Further division of the questionnaire into four distinct domains (self-perception, interactions, reading function, and general function) has been suggested.9 The instrument is reliable in terms of internal consistency and validity,7 and validation against the National Eye Institute Visual Function Questionnaire (NEI VFQ-25) found the AS-20 to be the more sensitive instrument in adult strabismus patients.8 Additionally, it has been translated and validated from the original English version into several other languages10–16 and is freely available on the public website of the Pediatric Eye Disease Investigator Group (PEDIG) https://public.jaeb.org/pedig/view/Forms_AS20 in English, Spanish, and Dutch.
The purpose of this study was to translate the AS-20 into Swedish in accordance with the appropriate translation guidelines and standards and to test and evaluate its reliability and validity.
Materials and Methods
The study was approved by the Regional Ethical Review Board in Gothenburg, Sweden (Dnr: 765–13 and Dnr:2021–01611) and followed the Tenets of the Declaration of Helsinki. As the research was based on translation and validation of questionnaires, it was considered not to have an impact on the care of the patients or on the individual. The translation process contained no background characteristic information about ethnicity and religion, which are sensitive information under Swedish law. Subjects gave their verbal consent in place of written consent to participate, which was approved by the ethics committee. Partakers were provided with a copy of the information sheet and given the opportunity to ask questions. The verbal consent process was documented by the researcher at the time of the dialogue as well as the participants ticking a consent box on the questionnaire.
The validation process followed the recommendations of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) recommended methodology.
Translation Process and Qualitative Validation
Preparation
The project managers and expert committee consisted of two experienced individuals in the ophthalmic field: an orthoptist (SF) and an ophthalmic nurse (LHJ). The study was conducted in two phases: first, the translation and evaluation of the original questionnaire and second, the validation and evaluation of the final version of the translated questionnaire. The translation process aimed for translators to capture the conceptual meaning of the questions rather than exact literal translation.
Forward Translation
The forward translation into Swedish was performed by 17 final-year orthoptist students at the University of Gothenburg, class of 2022, during an on-campus HRQoL workshop session led by the project managers. The students were native Swedish speakers and residents of Sweden. The class worked on the translation from English into Swedish in groups of four. Each group translated five questions and then repeatedly reconciled their peers’ translations. Once the documents had been passed through all the rounds, the project managers merged the translations into a single forward translation.
Reconciliation
A pilot study was conducted to explore people’s perceptions, thoughts, and opinions on the first draft of the Swedish AS-20 following the forward translation process. Through strategic sampling, the questionnaire was distributed to individuals who were not previously involved in the process. The students were instructed to give the questionnaire to three participants from different groups, whilst attending their final clinical placement. The groups were defined as patients with strabismus (experience of the condition investigated), experts (experienced clinical orthoptists) and laymen (members of the public). The participants were invited to comment freely on the questions, content, and experience of filling in the questionnaire to allow further refinement of the instrument. A total of 51 responses from residents in different parts of Sweden, rural and urban areas, and socioeconomic conditions were collected. Furthermore, individual reflections and comments on the translation were summarised and the text was reconciled by the project managers. The risk of biased translation was mitigated by the rigorous process as it included several different individuals and stages.
Back Translation and Review
The Swedish version of the AS-20 was sent to a professional translator for back-translation into English. The independent translator was a native Englishman, now a Swedish resident with a good knowledge of the Swedish language. The back-translation provided further quality control, in that the translation should have the same content and language after being converted back into English from Swedish as the original English version of the AS-20. In response to the translator’s comments, the project managers revised the Swedish AS-20 version, and a further review of the reconciled version was conducted to eliminate discrepancies.
Harmonization
Harmonization was achieved through thoroughness during the translation process. In addition, a harmonization meeting between the key in-country consultant (SF, bilingual Swedish-English), the expert committee and the back translators was held. All back translations were compared taking cultural adaptation into consideration.
Cognitive Debriefing
To ensure that the translation was comprehensible to the public and patients specifically, the instrument was tested by the key in-country person (SF) on a group of five respondents. This process tested the wording and understanding of the Swedish version as well as the interpretation and cultural relevance of the translation.
Review of Cognitive Debriefing Results and Finalization
The project managers reviewed the results from the cognitive debriefings. A comparison of the patient’s interpretation of the translation with the original version was performed by the native and resident project managers to identify and amend any final translation modifications necessary for improvement. Following agreement on finishing changes, the translation underwent ultimate proofreading, and the final version of the questionnaire was presented to the fourteen 2023 final year orthoptic students. They were instructed to distribute the questionnaire to four or five adult patients (aged 17 years or older) at their clinical placements, which were different from those in the first phase workshop. Subsequently, the first evaluation, analysis, and discussion of the results were conducted at a campus workshop session led by the project managers.
Quantitative Validation
All statistical analyses were conducted using the R software (version 4.2.1 (R Core Team, 2022). The translated instrument was quantitatively validated using two psychometric properties: internal consistency and construct validity. Internal consistency was calculated as Cronbach’s alpha for each of the two subscales (psychosocial and functional) using R package.17
Construct validity was evaluated using Rasch analysis to check the following properties: i) ordered item response categories, ii) item scores that fit the Rasch model, and iii) unidimensionality of each subscale. Since the AS-20 has five response categories per item, a polytomous generalization of the Rasch model must be applied, such as the partial credit model included in the R package eRM.18 The ordered response category property was checked using plots of item characteristic curves (ICC),9 the model fit was checked by calculating infit and outfit mean square (MNSQ) fit statistics. Unidimensionality was checked using the unidimensionality coefficient u calculated using the R package. The infit and outfit MNSQ have expectations of 1.0, ranging from zero to infinity. Mean-squares >1.0 indicate underfit to the Rasch model, while mean-squares <1.0 indicate an overfit to the Rasch model, with values within the interval 0.6–1.4 indicate an acceptable fit.
Results
Translation Process and Qualitative Validation
Forward Translation and Reconciliation Process
The first phase generated responses from the 51 participants in the initial version of the translation. Most respondents thought that the questions were well worded, grammatically correct, and easy to understand. One patient with strabismus caused by abducens palsy, who had undergone strabismus surgery, questioned why there was so much focus on the aesthetic aspect. Another comment from a layman was that several of the questions were about reading–would not there be an unnecessarily large weight on that particular aspect?” Feeling that there may be other issues as to why reading could be a problem, such as dyslexia, asthenopia, or even wearing the wrong corrective glasses. An expert with 30 years of clinical experience thought that the questionnaire was highly relevant for patients with strabismus, specifically for those with manifest strabismus without diplopia. Their primary concern is often the social aspect; however, they may be too anxious to mention this. The questionnaire made it easier for this group of patients to complete a score rather than talk about something that may have been a sensitive issue for many years.
In the expert group (ie, experienced clinical orthoptists), 53% did not believe that the questionnaire would be useful. Some of the comments were: “Why should it be used?” (two responses out of seventeen), “remove nine of the questions”, “change the order of the questions” and “patients who really want to be prioritised for strabismus surgery will fill in always” on every question to score higher. Of the 47% who thought the questionnaire was a valuable compliment to an orthoptic examination, comments were: “the questionnaire highlights that the patients really suffer” and that “the instrument is important for accessing psychosocial issues better than from a case history”.
In the laymen and patient groups, 71% thought that the questionnaire was useful and suitable, but two non-experts commented that “a few of the questions may be upsetting, as they have a negative tone as if strabismus is something to be embarrassed about”.
There were several comments from all the respondents, unrelated to the group category, that certain questions were “perceived as the same”. Suggestions for improvement included rephrasing and combining question number five, six, seven and nine into one and questions 12, 16, and 20 into one.
Following reconciliation and back-translation, the items and response options were reworded following cognitive debriefing, where respondents’ comments justified such changes. For specific comments from each respondent, see Table 1.
 |
Table 1 Comments Received from the First Phase of the Questionnaire Which Was Distributed to Patients, Experts and Laymen at Orthoptic Clinics in Sweden, Totaling 51 Responses |
Back Translation
The translator, from Swedish back to English, had comments and suggestions for minor grammatical rephrasing of four of the questions (Items 6, 9, 16, and 17). For a specific back translation, see Table 2.
 |
Table 2 Items from the Original Questionnaire That Were Slightly Changed for Clarity of Text in Swedish Following Back Translation |
Review of Cognitive Debriefing Results and Finalization
This stage resulted in validation of the Swedish AS-20 by 68 patients from Sweden.
Table 3 shows the baseline characteristics, and Figure 1 shows the individual scores.
 |
Table 3 Demographic and Clinical Data of All Subjects from Phase Two (N= 68) |
 |
Figure 1 The individual scores from 68 strabismic patients who participated in validating the final version of the translated AS-20. |
Quantitative Validation
The Cronbach’s alpha was 0.95 for the psychosocial subscale and 0.92 for the functional subscale, indicating good internal consistency.
ICC plots to evaluate the first construct validity criterion (ordered response categories) indicated that all psychosocial subscale items except Q2 had disordered categories. For the functional subscale, categories were disordered for items Q12, Q14, Q19, and Q20, while the remaining items fulfilled the criteria (Figure 2a and b).
Figure 2 Continued. Figure 2 (a) Item characteristic curves for the AS-20 psychosocial subscale. (b) Item characteristic curves for the AS-20 functional subscale.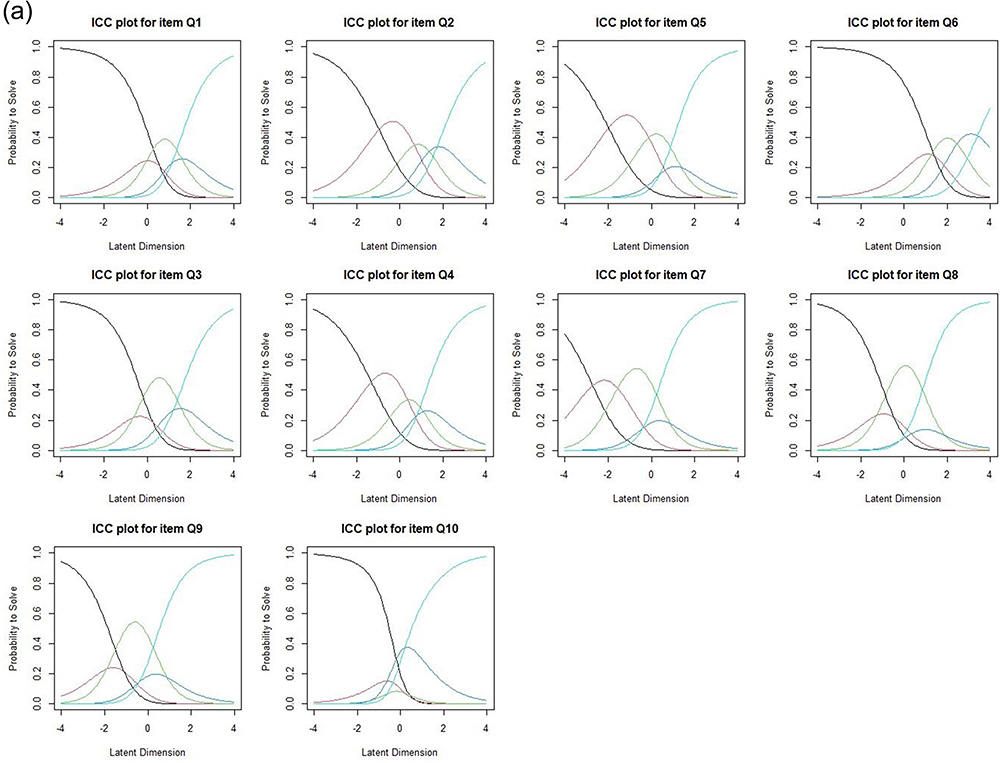

MNSQ infit and outfit values were calculated for both subscales, showing that most items on the psychosocial subscale, except Q2 and Q8, did not fit the Rasch model (Table 4). The items on the functional subscale showed acceptable fit statistics. The unidimensionality index, u, was acceptable for both subscales.
 |
Table 4 Unidimensionality Index, Outfit (Unweighted) Mean Square Statistic and Infit (Weighted) Mean Square Statistic for Items on Each Subscale |
Discussion
In summary, qualitative evaluation of the AS-20 questionnaire translated into Swedish showed the translated instrument to be valid, while quantitative evaluation using Rasch analysis indicated that the translated instrument required further adjustments to achieve consistent validity. The results from the Rasch analysis suggest that both subscales should be reduced in items and response categories.
Until now, the AS-20 has not been available in Swedish, and therefore English or Danish versions have been substituted in Swedish clinical practice. However, using an instrument not in the patients first language may compromise the validity of the results; thus, the AS-20 was translated into Swedish and tested for validity. A correct translation and validation process is important, as a poorly translated instrument tethers the validity of research data.19 This study conformed to the principles of good practice for the translation and cultural adaptation process for patient-related outcomes (PRO), and the validation process followed the recommendations of ISPOR.
The relationship between language, translation and culture is a key aspect of communication.
Therefore, cultural adaptation is highly relevant in the validation process when adapting an existing instrument (AS-20) to measure a phenomenon in people who speak another language and have a different culture. The text needs to be not only “linguistically correct”, but also culturally sensitive. In every translation, the questions undergo a set of changes, whereby information is lost, added, and deformed. Certain phrases may fall out of context unless culturally adapted, as direct translations of idiomatic expressions may not be appropriate in the target language culture. The various stages performed during the translation and validation processes in this study and the diversity of responders fulfilled these criteria.
Unlike some previous translations of AS-20, we did not add specifications or additional questions to the questionnaire regarding certain tasks such as driving or computer usage. We believe that the neutral nature of the AS-20 is important. It was originally designed to not discriminate between socioeconomic, cultural, and educational statuses.
Translation Process and Qualitative Evaluation
Some of the comments received from the experts reflected an unawareness of the instrument’s purpose and showed that it is important that the orthoptist is not involved when the patient fills the questionnaire, as they can influence and control the answers. For example, we believe that the orthoptist may downplay the patients’ actual problems, which demonstrates the importance of investigating the patients’ subjective experiences and problems and taking them into consideration during clinical decision-making to avoid bias. We also believe that another reason why some experts had a negative approach to the questionnaire was their lack of knowledge. Most of the experts were clinical tutors and supervisors and were close to or over the age of 60. This generation did not use PROMs or HRQoL questionnaires during their work experience. It is easy to have preconceptions about something you do not fully understand. Therefore, it is important to cover the aspects of HRQoL in orthoptic education to implement this aspect in future care. There was a vast difference in the susceptibility and acceptance of using the questionnaire from orthoptic students attending the workshop, as they did not have any preconceptions.
Throughout the development and validation process of the AS-20, there have been reports of more women in the study groups than men. There were 68% female respondents in the first round of interviews and 66% during the final version.7 In the Scandinavian validations 70% and 59% were female.12,14 Our translation and validation processes showed a similar trend, with 63% of the participants being women. This may be an example of gender bias in health care, as mentioned in a recent study by Laughton et al, who reported that males and females have the same prevalence of strabismus, but there is a different societal attitude towards women.20
In previous translations and validations of AS-20, there have been suggestions to remove question 14 “I have problems with depth perception”. 12,15 In the Finnish refined version of the AS-20, items 14 and 19, I can´t enjoy hobbies because of my eyes”, were not scored. The two items considered for removal when performing Rasch analysis were items 14 and 19.9 The reason these items are highlighted during other validation processes may be that the wording causes confusion for some subjects. Not all subjects are aware of the meaning of “depth perception”, and they may not have hobbies or have multiple hobbies and may have difficulty with some but not all. Our results from the responses from phase one indicated that some questions could be rephrased and combined as they were perceived as asking about the same thing. Thus, indicating that the questionnaire could be condensed into fewer items. For future studies, our aim will be to analyse a shortened version of the validated Swedish AS-20. A condensed AS-20 may be considered more “user-friendly” and could encourage more clinics to implement it in their routine.
Strengths/Weaknesses
The strength of adding a qualitative part to the present study is that the questionnaire was analysed in further detail by engaging individuals from various groups with different backgrounds and experiences. The validation process follows ISPOR, the recommended methodology, which was a guarantee for quality insurance.
Conclusion
This study confirms that the AS-20 is a qualitatively valid instrument to use in the Swedish language, yet the quantitative validity criteria defined in the Rasch analysis are not fulfilled. Future studies need to evaluate whether a shorter version would be just as appropriate and reliable and perhaps even more applicable for use in a clinical setting. This may enhance the use of HRQoL instruments in clinical decision making and improve the quality of care for patients with strabismus.
Acknowledgments
The authors express their gratitude to the orthoptic students, patients, experts, and laymen, who assisted in validating the AS-20 questionnaire.
Funding
This work was supported by “Greta Andersson foundation G2017-4”.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Fayers PM. Quality of Life: The Assessment, Analysis, and Reporting of Patient-Reported Outcomes.
2. Buffenn AN. The impact of strabismus on psychosocial heath and quality of life: a systematic review. Surv Ophthalmol. 2021;66(6):1051–1064. doi:10.1016/j.survophthal.2021.03.005
3. Durnian JM, Noonan CP, Marsh IB. The psychosocial effects of adult strabismus: a review. Br J Ophthalmol. 2011;95(4):450–453. doi:10.1136/bjo.2010.188425
4. Chang MY, Velez FG, Demer JL, Isenberg SJ, Coleman AL, Pineles SL. Quality of life in adults with strabismus. Am J Ophthalmol. 2015;159(3):539–544.e2. doi:10.1016/j.ajo.2014.12.003
5. McBain HB, MacKenzie KA, Au C, et al. Factors associated with quality of life and mood in adults with strabismus. Br J Ophthalmol. 2014;98(4):550–555. doi:10.1136/bjophthalmol-2013-304220
6. Carlton J, Kaltenthaler E. Health-related quality of life measures (HRQoL) in patients with amblyopia and strabismus: a systematic review. Br J Ophthalmol. 2011;95(3):325–330. doi:10.1136/bjo.2009.178889
7. Hatt SR, Leske DA, Bradley EA, Cole SR, Holmes JM. Development of a quality-of-life questionnaire for adults with strabismus. Ophthalmology. 2009;116(1):139–144.e5. doi:10.1016/j.ophtha.2008.08.043
8. Hatt SR, Leske DA, Bradley EA, Cole SR, Holmes JM. Comparison of quality-of-life instruments in adults with strabismus. Am J Ophthalmol. 2009;148(4):558–562. doi:10.1016/j.ajo.2009.05.009
9. Leske DA, Hatt SR, Liebermann L, Holmes JM. Evaluation of the adult strabismus-20 (AS-20) questionnaire using rasch analysis. Invest Ophthalmol Visual Sci. 2012;53(6):2630–2639. doi:10.1167/iovs.11-8308
10. Akbari MR, Masoomian B, Ameri A, Keshtkar Jaafari A, Mirmohammadsadeghi A. Development of a Persian version of the adult strabismus questionnaire and evaluating the effect of strabismus surgery on health-related quality of life. Strabismus. 2015;23(2):66–72. doi:10.3109/09273972.2015.1025986
11. Alamri R, Alyousef M, Bamardouf N, Alharbi B, Raffa L. Validation of the health-related quality of life questionnaire for adult strabismus AS-20 in the Arabic language. Saudi J Health Sci. 2022;11(3):197–202. doi:10.4103/sjhs.sjhs_113_22
12. Ali N, Sørensen MS, Sørensen TL, Mortzos P. Evaluation and validity of the Danish version of the adult strabismus questionnaire AS-20. Clin Ophthalmol. 2016;10(Issue 1):65–69. doi:10.2147/OPTH.S90844
13. Burggraaf F, Elsman EBM, Nispen RMA, Tjon‐Fo‐Sang MJ, Spek B, Jellema HM. Psychometric properties of the Dutch version adult strabismus-20 questionnaire (AS-20). Ophthalmic Physiol Opt. 2021;41(5):1007–1020. doi:10.1111/opo.12865
14. Mason A, Joronen K, Lindberg L, Koivisto A-M, Fagerholm N, Rantanen A. Health-related quality of life in adult patients with strabismus—translation and psychometric testing of the adult strabismus questionnaire (AS-20) into Finnish. Int J Environ Res Public Health. 2023;20(4):2830. doi:10.3390/ijerph20042830
15. Ortiz Montero T, Lugo Boton IK, Montenegro MB, Mejía JC, Baquero L, Mejia-Vergara AJ. Translation and transcultural adaptation of the AS-20 scale to measure quality of life in adults with strabismus in Colombia, a pilot study. Archivos de la Sociedad Española de Oftalmología. 2023;98(3):142–149. doi:10.1016/j.oftale.2022.11.005
16. Yu H, Yang X, Ye T, Chen J, Zhang F, Yu X. Development and evaluation of a Chinese version of the adult strabismus questionnaire (AS-20). Ophthalmic Epidemiol. 2013;20(4):239–247. doi:10.3109/09286586.2013.809771
17. Revelle WR. Psych: procedures for personality and psychological research. Software. 2024. Available from: https://personality-project.org/r/psych-manual.pdf.
18. Mair P, Hatzinger R. Extended rasch modeling: the eRm package for the application of IRT models in R. J Stat Softw. 2007;20(9):1–20. doi:10.18637/jss.v020.i09
19. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. doi:10.1111/j.1524-4733.2005.04054.x
20. Laughton SC, Hagen MM, Yang W, von Bartheld CS. Gender differences in horizontal strabismus: systematic review and meta-analysis shows no difference in prevalence, but gender bias towards females in the clinic. J Glob Health. 2023;13:04085. doi:10.7189/JOGH.13.04085
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.