")
Back to Journals » Journal of Inflammation Research » Volume 18
Tryptase as a Biomarker for Adverse Prognosis in ST-Segment Elevation Myocardial Infarction Patients: A Prospective Cohort Study
Authors Xie P , Xu S, Chen X, Xu H, Zhang R, Li D, Sun L, Zhu D, Cui M
Received 3 November 2024
Accepted for publication 2 March 2025
Published 14 March 2025 Volume 2025:18 Pages 3817—3828
DOI https://doi.org/10.2147/JIR.S502496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Adam Bachstetter
Pengxin Xie,1,2 Shuwan Xu,1,2 Xi Chen,1,2 Hong Xu,3 Ruitao Zhang,1,2 Dan Li,1,2 Lijie Sun,1,2 Dan Zhu,1,2 Ming Cui1,2
1Department of Cardiology and Institute of Vascular Medicine, Peking University Third Hospital, Beijing, People’s Republic of China; 2State Key Laboratory of Vascular Homeostasis and Remodeling, Peking University Third Hospital, Beijing, People’s Republic of China; 3College of Science, Minzu University of China, Beijing, People’s Republic of China
Correspondence: Ming Cui; Dan Zhu, Department of Cardiology and Institute of Vascular Medicine, Peking University Third Hospital, 49 North Garden Road, Beijing, 100191, People’s Republic of China, Email [email protected]; [email protected]
Background: Acute ST-segment elevation myocardial infarction (STEMI) is characterized by a rapid inflammatory response, with mast cells (MCs) playing a significant role. However, the relationship between MC activation and the adverse outcomes remains unclear. This study investigated the association between the MC activation biomarker, tryptase, and major adverse cardiovascular events (MACE).
Methods: This prospective study included patients with STEMI who underwent primary percutaneous coronary intervention (PPCI) at Peking University Third Hospital between July 2020 and July 2023. Tryptase levels were detected from plasma samples collected 6 hours post-PPCI and using ELISA method. All patients were followed up every 6 months, with MACE as the primary endpoint.
Results: The study enrolled 514 patients with STEMI who underwent PPCI (mean age: 59.27 ± 13.26 years, 16.93% female). The median follow-up time was 13.28 (10.47– 37.61) months, during which 85 patients (16.54%) experienced MACE. Patients in the higher tryptase group had a higher risk of MACE (HR 2.60 [1.68– 4.01], P < 0.001). Tryptase was an independent risk factor of MACE (HR 1.56 [1.29– 1.88] per 1-unit increase, P < 0.001). Subgroup analysis revealed the prognostic value of tryptase among different age groups, left ventricular ejection levels, and patients with hypertension, hyperlipidemia, smoking and diabetes. The addition of tryptase to the basic model had an incremental effect on the predictive value for MACE (AUC: 0.763 vs 0.702, P = 0.002).
Conclusion: In this study, elevated tryptase levels, a biomarker of MC activation, were identified as a significant predictor of MACE in STEMI patients undergoing PPCI.
Trial Registration: (ClinicalTrials.gov NCT05802667).
Keywords: acute ST-segment elevation myocardial infarction, mast cells, tryptase, major adverse cardiovascular events, prognosis
Introduction
Acute ST-segment elevation myocardial infarction (STEMI) is the most severe type in coronary heart disease. Primary percutaneous coronary intervention (PPCI) is a critical treatment for STEMI.1,2 Plaque rupture, thrombosis and reperfusion after PPCI in these patients are associated with a severe inflammatory response.3
Various inflammatory cells contribute to the inflammatory responses, such as macrophages, lymphocytes, dendritic cells, and mast cells (MCs). Cardiac MCs are mainly distributed in the coronary adventitia and cardiac interstitium.4,5 After myocardial infarction, MCs are rapidly activated by immunoglobulin E, complement components, neuropeptides or cytokines, leading to the release of over 50 active substances.6 MCs are associated with STEMI at various stages, participating in the rupture plaques and ischemia-reperfusion injury by producing various inflammatory cytokines (eg, tumor necrosis factor-α [TNF-α], interferon-γ, interleukin-6 [IL-6], histamine, leukotriene C4, chymase and tryptase).7 A few days after myocardial infarction, MCs release chymase and tryptase, promoting the production of transforming growth factor-β (TGF-β) and angiotensin II, which are key initiators of fibroblast activation.8 Additionally, MCs play roles in other cardiac conditions such as diabetic cardiomyopathy,9 valvular heart disease10 and myocarditis.11 In diabetic mouse, MCs alleviate myocardial fibrosis by inhibiting macrophage aggregation and the release of pro-inflammatory factors while modulating the TGF-β signaling pathway in fibroblasts.9
Tryptase, which is stored in vesicles within MCs and released upon activation, is the gold standard for evaluating the extent of MC activation.12 In patients with acute coronary syndrome, tryptase is a predictor of adverse outcomes within 2 years.13 In STEMI patients, the MC activator, immunoglobulin E, was found to be significantly increased during the acute phase.14 Serum tryptase was significantly elevated in STEMI and negatively correlated with the 2 hours ST-segment resolution rate and left ventricular ejection fraction (LVEF).15,16 However, current research on the relationship between acute-phase tryptase levels and adverse outcomes in STEMI patients is still limited. Based on this, the study was designed with the aim of: (1) identifying the potential association between tryptase levels and clinical prognosis; (2) determining whether tryptase has an incremental effect on risk stratification based on traditional risk factors in STEMI patients who have undergone PPCI.
Materials and Methods
Study Design and Population
This was a prospective cohort study that included patients with STEMI who underwent PPCI at Peking University Third Hospital between July 2020 and July 2023. The inclusion criteria were: 1) age 18 or older, regardless of sex; 2) meeting the STEMI diagnostic criteria (ie, ischemic chest pain lasting ≥30 minutes; ST-segment elevation in two or more contiguous leads or new-onset left bundle branch block on electrocardiograph with or without elevated cardiac biomarkers); 3) complete PPCI and revascularization of the culprit vessel; and 4) agreement to participate in the study.
Exclusion criteria were: 1) chronic renal dysfunction with glomerular filtration rate <30 mL/min/1.73 m²; 2) currently suffering from infectious and neoplastic diseases; 3) allergic or autoimmune diseases; and 4) current or planned long-term use of oral or intravenous glucocorticoids. This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Peking University Third Hospital. All patients signed informed consent forms prior to study commencement.
Between July 2020 and July 2023, a total of 587 patients with STEMI were screened. Of these, 42 patients were excluded due to comorbidities, and 31 were excluded due to a follow-up period of less than 8 months, resulting in 514 patients for the final analysis (Figure 1).
 |
Figure 1 Patient inclusion and exclusion flowchart. Abbreviation: STEMI, ST-elevation myocardial infarction. |
Data Collection
The general demographic characteristics, medical history, laboratory and echocardiography findings were collected by the electronic medical record system. All the patients underwent selective coronary angiography. Two experienced interventional cardiologists identified the culprit vessel based on electrocardiograph and coronary angiography, then performed PPCI. The patients underwent secondary prevention for coronary artery disease based on their condition.
Tryptase Assay
After 6 hours of post PPCI, blood samples were collected in ethylenediamine tetraacetic acid-containing anticoagulant tubes and immediately stored at 4°C. Within 30 minutes of collection, samples were centrifuged at 3000 rpm for 10 minutes at 4°C to obtain plasma, which was then frozen at −80°C until detected. Repeated freeze-thaw cycles of the samples were avoided. Tryptase levels in the plasma were detected using ELISA method according to the manufacturer’s instructions (ml060170B; Mibio, Shanghai, China). Samples from 50 randomly selected patients were retested to assess the stability of tryptase detection across batches. The results indicated excellent consistency, with an inter-observer reliability of 0.999 (95% CI: 0.999–1.000).
Follow-up Strategy
All patients were routinely followed up by trained professionals who were blinded to the tryptase every 6 months by medical systems and telephone. The primary endpoint of this study was major adverse cardiovascular events (MACE), including cardiac death, all-cause death, readmission for heart failure (HF, ICD-10 I50), and recurrent coronary events [recurrent myocardial infarction (ICD-10 I21), unplanned percutaneous coronary intervention, and coronary artery bypass grafting].
The secondary endpoint was major adverse cerebrovascular and cardiovascular events (MACCE), which included MACE and stroke (ICD-10 I63 and I61). The first endpoint event that occurred during follow-up was used for analysis. All events were independently adjudicated by two experienced cardiologists who were blinded to the tryptase levels. In cases of disagreement, a third senior cardiologist made the final decision.
Statistical Methods
Based on the preliminary trial results, 51 STEMI patients were enrolled and divided into the higher and lower groups. The follow-up period lasted 12 months. In the lower group (35 patients), 11.43% of patients experienced MACE, whereas in the higher group (16 patients), 25.00% patients experienced MACE. Sample size calculations were performed using PASS (version 21.0.3, NCSS LLC., Kaysville, U.T., USA), with β = 0.10 and α = 0.05, which indicated that sample size is 426 patients. Considering a 20% dropout rate, a total of 511 patients were required.
For continuous variables following a normal distribution, the mean ± standard deviation was used, and comparisons between the two groups were made using an independent sample t-test. For continuous variables that did not follow a normal distribution, the median (Q1 and Q3) was reported, and the Wilcoxon rank-sum test was used for group comparisons. Categorical variables were expressed as counts and percentages, and comparisons were made using the chi-squared test. Restricted cubic spline (RCS) was used to assess the relationship between tryptase and traditional cardiovascular risk factors. Patients were divided into higher and lower tryptase groups based on the optimal cutoff value of tryptase. Kaplan-Meier survival analysis was used to plot survival curves for the two groups, with comparisons between groups using the Log rank test. Least absolute shrinkage and selection operator (LASSO) regression was used to select the variables for the multivariate Cox regression model.
To determine the incremental prognostic value of tryptase adding to the traditional risk prediction models, three Cox regression models were established: Model 1 included the thrombolysis in myocardial infarction (TIMI) risk score, Model 2 included Model 1 + LVEF + high-sensitivity C-reactive protein (hsCRP), and Model 3 included Model 2 + tryptase. The Delong test was used to compare the areas under the curve (AUC) between the different models. Bootstrapping with 1000 resamples was conducted to calculate integrated discrimination improvement (IDI) and net reclassification improvement (NRI) across the models. In the sensitivity analysis, MACCE confirmed the robustness of the tryptase value in risk stratification. Statistical significance was set at P < 0.05. All analyses were performed using SPSS (version 25; IBM, Armonk, NY, USA) and R (version 4.2.0; R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
A total of 514 patients (mean age: 59.27 ± 13.26 years) were enrolled in this study, including 87 female patients (16.93%) and 199 patients (38.72%) presenting with anterior myocardial infarction (Table 1). During a median follow-up period of 13.28 (10.47, 37.61) months, there were 85 cases (16.54%) of MACE and 89 cases (17.32%) of MACCE. Among these, there were 12 cases (2.33%) of cardiac death, 22 (4.28%) of all-cause death, 17 (3.31%) of readmission for HF, 51 (9.92%) of recurrent coronary events, and 6 (1.17%) of stroke.
 |
Table 1 The Clinical Characteristics of STEMI Patients After PPCI |
The receiver operator characteristic curve of tryptase was generated based on MACE during the follow-up period, with an optimal cutoff value identified as 2.20 ng/mL. The AUC of tryptase for MACE is greater than that of the classic inflammatory marker hsCRP (P = 0.046) (Supplementary Figure S1). The patients were divided into the higher (n=132) and lower (n=382) tryptase groups based on the cutoff value. The higher group had higher rates of assistant instruments, anterior myocardial infarction, Killip grade II or higher. TIMI risk score, hsCRP and peak CKMB were higher in the higher group compared to the lower group. Hemoglobin, LVEF, and global longitudinal strain (GLS) were lower in the higher tryptase group (Table 1). There was no difference between the two groups in terms of the use of secondary prevention medications for coronary artery disease. Additionally, the incidence of MACE, MACCE, cardiac death and readmission for HF and recurrence coronary event was significantly higher in the higher tryptase group (Supplement Figure S2).
Relationship Between Tryptase and Adverse Outcomes
Kaplan-Meier survival analysis showed the patients in higher group had higher risk of MACE (HR 2.60 [1.68–4.01, P < 0.001), cardiac death and readmission for HF (HR 3.02 [1.44–6.33], P = 0.002) and recurrent coronary events (HR 2.31 [1.31–4.10], P = 0.003) compared to the lower group (Figure 2).
 |
Figure 2 Kaplan–Meier curves for endpoint events in higher and lower tryptase group. Kaplan–Meier curves for (A) MACE, (B) cardiac death and readmission for heart failure, (C) recurrent coronary events and (D) MACCE. Abbreviations: MACE, major adverse cardiac events; MACCE, major adverse cerebrovascular and cardiovascular events; HR, hazard ratio; CI, confidence interval. |
RCS were used to assess the relationship between tryptase and common risk factors. Tryptase positively correlated with MACE, anterior myocardial infarction, SYNTAX score, and peak CKMB. It showed a negative correlation with LVEF, and a U-shaped curve with hsCRP (Supplement Figure S3).
Cox Proportional Hazard Analyses to Evaluate the Prognostic Implication of Tryptase
In univariate Cox regression analysis, Killip grade (HR 2.65 [1.70–4.14], P<0.001), multivessel disease (HR 2.02 [1.21–3.37], P=0.007), complete revascularization (HR 0.29 [0.18–0.46], P<0.001), hemoglobin (HR 0.98 [0.97–0.99], P<0.001), tryptase (HR 1.98 [1.70–2.34], P<0.001), peak CKMB >300 U/L (HR 2.33 [1.47–3.70], P<0.001), LVEF (HR 0.94 [0.92–0.95], P<0.001), segmental motion (HR 2.42 [1.04–5.63], P=0.039), and absolute value of GLS (HR 0.79 [0.74–0.85], P=0.002) were the predictors of MACE.
Variables from Table 1 were included in the LASSO regression to select variables for Cox multivariate regression in order to reduce the risk of overfitting. Multivessel disease, complete revascularization, LVEF, segmental motion, hemoglobin, absolute value of GLS and tryptase were included in the Cox multivariate analysis (Supplement Figure S4). The analysis indicated that tryptase (HR 1.56 [1.29–1.88], P<0.001) was an independent predictor of MACE (Table 2).
 |
Table 2 Multivariate COX Regression of MACE and MACCE |
To further control for the influence of confounding variables, three models were constructed in this study. Model 1 only included tryptase levels, while model 2 included demographic characteristics, comorbidities and tryptase. Model 3 further incorporated additional variables such as multivessel disease, complete revascularization, door-to-balloon time, hemoglobin, LVEF, segmental motion, GLS and medication regimen into Model 2. Despite adjusting for these factors, tryptase remained a significant predictor of prognosis (HR 1.96 [1.57–2.45], P < 0.001). When the tryptase level was categorized into two groups, it still showed significant prognostic value (Table 3).
 |
Table 3 Predictive Value of Tryptase for MACE in Different Cox Proportional Hazards Models |
Tryptase revealed the risk stratification value for MACE in different subgroup including age (≤60 years or >60 years), smoking, presence of hypertension, hyperlipidemia, diabetes, anterior myocardial infarction, LVEF (≥50% or <50%), and male patients. However, the prognostic significance of tryptase was not statistically significant in female patients. These findings remained consistent after adjusting for variables factors such as thrombus aspiration, GP IIb/IIIa inhibitors, multivessel disease, left main coronary artery lesions, and assistant instruments (Figure 3).
 |
Figure 3 Cox proportional hazards analysis evaluating prognostic implication of tryptase in different subgroup. HR was evaluated by 1-unit increase of tryptase. Abbreviation: LVEF, left ventricular ejection fraction. |
Incremental Effect of Tryptase on Predictive Value for MACE
To investigate the incremental predictive value of tryptase for MACE, the traditional TIMI risk score was used as Model 1. Model 2 was constructed by adding LVEF and hsCRP to Model 1, and Model 3 was further developed by including tryptase into Model 2. Model 2 revealed improved discrimination for MACE (AUC: 0.702 vs 0.628, P=0.013) compared to Model 1, and Model 3 with the addition of tryptase further improved event discrimination (AUC: 0.763 vs 0.702, P=0.002) compared to Model 2. Bootstrap resampling was performed 1000 times. The inclusion of tryptase significantly enhanced the reclassification and discrimination capabilities of baseline risk models. Model 3 showed improved IDI and NRI values compared to both Model 1 (IDI 0.135 [0.133–0.137], NRI 0.331 [0.331–0.331], all P < 0.001) and Model 2 (IDI 0.049 [0.048–0.050], NRI 0.168 [0.163–0.174], all P < 0.001). Based on the shorter interquartile range in the box plot, it can be observed that Model 3 demonstrates superior stability (Figure 4).
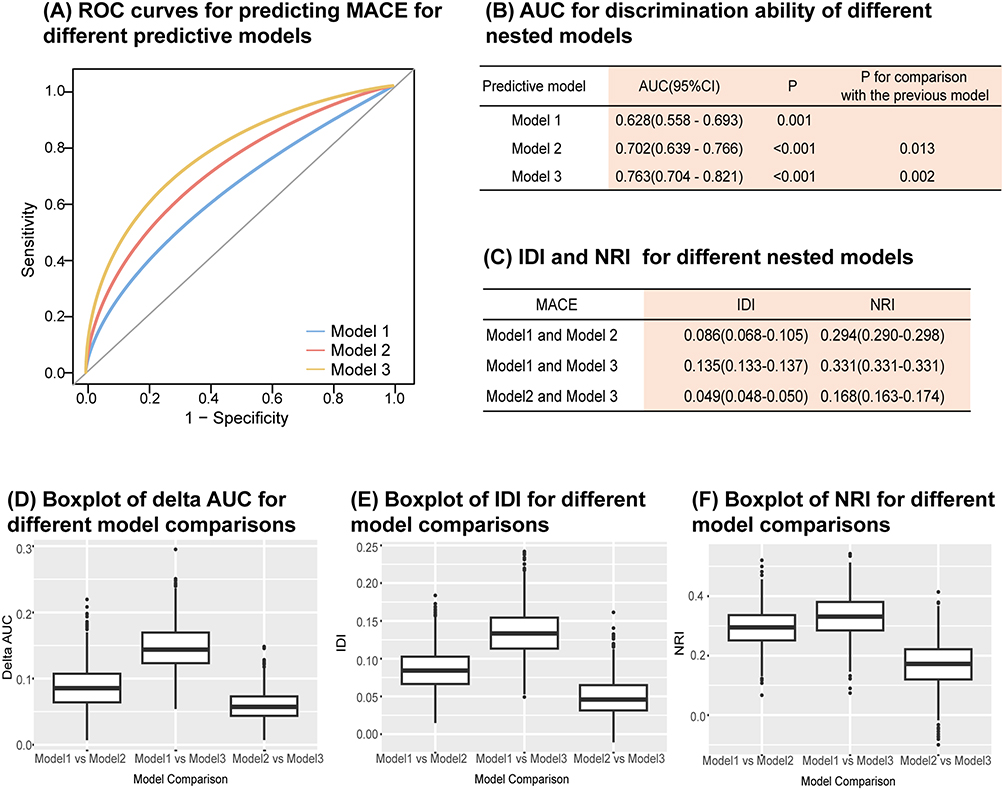 |
Figure 4 Comparison of the discriminative ability of different predictive models to determine the incremental prognostic value of tryptase. Three models were constructed: Model 1: TIMI risk score; Model 2: Model 1 + left ventricular ejection fraction + high-sensitivity C-reactive protein; Model 3: Model 2 + tryptase. (A) ROC curves for predicting MACE for different predictive models; (B) C-statistics for discrimination ability of different nested models; (C) IDI and NRI for different nested model in 1000 times bootstrap; Boxplots of difference in AUC (D), IDI (E) and NRI (F) between different nested models. Abbreviations: MACE, major adverse cardiac events; AUC, area under curve; IDI, integrated discrimination improvement; NRI, net reclassification improvement. |
Sensitivity Analysis
The incidence of MACCE remained significantly higher in the higher tryptase group (Supplement Figure S2). Kaplan-Meier survival curve analysis showed the difference in the prognosis of MACCE between the two groups (HR 2.77 [1.81–4.23], P < 0.001) (Figure 2D). In the multivariate regression model, tryptase remained a significant predictor of MACCE (HR 2.07 [1.52–2.83], P<0.001) (Table 2).
Discussion
This study prospectively included STEMI patients undergoing PPCI. The results indicated that elevated tryptase levels during the acute phase were associated with a higher risk of adverse outcomes. After adjusting for confounding variables, tryptase remained an independent risk factor for MACE. Incorporating tryptase into the traditional STEMI risk stratification model improved predictive ability. This study evaluated the prognostic value of MC activation during the acute phase in myocardial infarction, laying the foundation for further investigation into the underlying mechanisms of MCs.
Growing evidence suggests that MCs promote inflammatory responses after myocardial infarction by releasing various cytokines.17 Among inflammatory cells, only MCs contain pre-stored TNF-α, which is rapidly released under the stimulation of nitric oxide.18 TNF-α is a critical inflammatory factor in myocardial ischemia-reperfusion injury.19 MCs release tryptase and chymase, which exacerbate myocardial injury by directly degrading collagen, elastin, fibronectin, and laminin.20 MCs are involved not only in the acute phase of STEMI, but also in the process of ventricular remodeling over weeks and months. MCs release renin and chymase, promoting the conversion of angiotensin I to angiotensin II, thus activating the local renin-angiotensin-aldosterone system. This pathway is the primary source of angiotensin II in the cardiovascular system, independent of angiotensin converting enzyme.21 MCs are significant sources of fibroblast growth factor and TGF-β, promoting fibrosis after myocardial infarction.22 However, some studies have shown that MCs can alleviate the inflammatory response, accelerate repair in the infarcted area, and reduce myocardial fibrosis in myocardial infarction.23,24
In 2006, Kounis reported that the association between hypersensitivity reactions and angina, highlighting the link between MCs and acute coronary syndrome.25 Multiple clinical studies have demonstrated that MCs play an important role in the development of STEMI. The number of MCs in the myocardial tissue is higher than that in normal tissue, and this phenomenon has also been observed in the atherosclerotic plaques of autopsied patients.26,27 Yang et al found that among 278 patients with STEMI, leukotriene C4 (MCs products) level was an independent predictor of adverse ventricular remodeling at 6 months.28 In this study, with a median follow-up time of 13 months, tryptase remained an indicator for MACE and MACCE after multivariant adjustment. Although this study did not include information for coronary artery disease secondary prevention medication during follow-up, which may affect the conclusions, the results remained unchanged after adjusting for the use of these medications during hospitalization. Future studies should further collect information on these during the follow-up to avoid potential effect. Subgroup analysis revealed that tryptase was significant across different age groups, medical history, and LVEF classifications, suggesting that MC activation has prognostic value across various populations. However, the predictive ability of tryptase level in female patients did not reach statistical significance, possibly due to the limited number of female participants in this study.
MCs are closely associated with allergic disease, infectious diseases, autoimmune diseases, and tumors.29,30 Medications such as ketotifen, cromolyn sodium, omalizumab, and corticosteroids, which are used to treat allergic diseases and asthma, may also influence MC activation. Therefore, to minimize the impact of medications and comorbidities on tryptase, this study excluded patients with allergic diseases, infectious diseases, autoimmune disorders, and tumors. Tryptase peaks 30 minutes to 6 hours after MC activation, and it is recommended that its detection time not exceed 6 hours post-reaction.31–33 Previous studies have shown that the tryptase level at 6 hours post-PCI was negatively correlated with LVEF and the ST-segment resolution rate at 2 hours, which were significantly associated with long-term adverse prognosis.15 Though coronary blood may have higher tryptase concentrations, the choice of peripheral blood at 6 hours post-PCI was made to facilitate the future expansion of the study and increase its applicability to a broader population. While common biomarkers like troponin and CKMB require multiple blood draws to measure peak levels, this study suggests that measuring tryptase 6 hours after PPCI may serve as a prognostic indicator, potentially reducing the need for multiple blood draws.34,35
The TIMI risk score is widely used to assess the risk in STEMI patients; however, its predictive ability still requires further improvement.36,37 In this study, the AUC of TIMI risk score was relatively low. The incorporating of tryptase, hsCRP and LVEF into the traditional TIMI risk score improved the model’s accuracy. The results indicated that tryptase, in conjunction with the traditional inflammatory marker hsCRP, further improved the prognostic predictive ability for patients. However, it must be noted that the increase in AUC was relatively modest. This could be attributed to the fact that the baseline model already incorporates established high-efficiency prognostic markers such as the TIMI risk score, hsCRP, and LVEF. Furthermore, the predictive value of tryptase may be more prominent in specific subgroups. Therefore, further large-scale studies with longer follow-up periods will be crucial to explore the clinical application.
A series of animal experiments confirmed that using MCs stabilizers or histamine receptor antagonists can reduce myocardial infarction size.17,38 In a clinical study involving over 30 patients with acute inferior myocardial infarction, a randomized crossover trial revealed that the use of loratadine (a histamine receptor antagonist) could improve ischemic parameters during cardiopulmonary exercise in STEMI patients.39 There is a clinical study evaluating the impact of acute-phase interventions targeting MCs on prognosis of STEMI (NCT05511831).
Limitations
Meanwhile, several limitations should be recognized. 1) This was a single-center, prospective study, which may inevitably cause selection bias. Multicenter studies with larger sample sizes are required to confirm these findings. 2) In this study, tryptase levels were not measured multiple times during the acute phase or follow-up. Future studies could measure tryptase concentrations at multiple time points and follow-up to assess the relationship between the magnitude of tryptase elevation and prognosis. 3) It was difficult to exclude undiagnosed systemic diseases such as asymptomatic autoimmune diseases and tumors, as well as delayed allergic reactions to contrast agents or abnormal local reactions after PPCI. 4) The medication adjustments including coronary artery disease secondary prevention treatment during the follow-up were not included in the analysis, which may have impacted the patient’s prognosis.
Conclusion
From the prospective cohort study, it is shown that the MC activation biomarker tryptase is a significant risk predictor of MACE in patients with STEMI undergoing PPCI. The addition of tryptase to a baseline risk model has an incremental effect on the predictive potential for adverse prognosis. Further prospective, multi-center clinical studies and basic experiments need to be performed to validate the conclusions and explore the potential mechanisms of MCs in STEMI patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank all patients who participated in the study.
Funding
This study was funded by the National Natural Science Foundation of China (grant number 82070272), Beijing Research Ward Excellence Clinical Study Program (BRWEP2024W014090201), and Key Clinical Projects of Peking University Third Hospital (No. 2024003).
Disclosure
The authors declare that they have no competing interests.
References
1. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
2. Wong GC, Welsford M, Ainsworth C, et al. 2019 Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology Guidelines on the Acute Management of ST-elevation myocardial infarction: focused update on regionalization and reperfusion. Can J Cardiol. 2019;35(2):107–132. doi:10.1016/j.cjca.2018.11.031
3. Kologrivova I, Kercheva M, Panteleev O, Ryabov V. The role of inflammation in the pathogenesis of cardiogenic shock secondary to acute myocardial infarction: a narrative review. Biomedicines. 2024;12(9):2073. doi:10.3390/biomedicines12092073
4. Hermans M, Lennep JRV, van Daele P, Bot I. Mast cells in cardiovascular disease: from bench to bedside. Int J Mol Sci. 2019;20(14):3395. doi:10.3390/ijms20143395
5. Andreadou I, Cabrera-Fuentes HA, Devaux Y, et al. Immune cells as targets for cardioprotection: new players and novel therapeutic opportunities. Cardiovasc Res. 2019;115(7):1117–1130. doi:10.1093/cvr/cvz050
6. Kologrivova I, Shtatolkina M, Suslova T, Ryabov V. Cells of the immune system in cardiac remodeling: main players in resolution of inflammation and repair after myocardial infarction. Front Immunol. 2021;12:664457. doi:10.3389/fimmu.2021.664457
7. Kupreishvili K, Fuijkschot WW, Vonk AB, et al. Mast cells are increased in the media of coronary lesions in patients with myocardial infarction and may favor atherosclerotic plaque instability. J Cardiol. 2017;69(3):548–554. doi:10.1016/j.jjcc.2016.04.018
8. Lagraauw HM, Wezel A, van der Velden D, Kuiper J, Bot I. Stress-induced mast cell activation contributes to atherosclerotic plaque destabilization. Sci Rep. 2019;9(1):2134. doi:10.1038/s41598-019-38679-4
9. He A, Fang W, Zhao K, et al. Mast cell-deficiency protects mice from streptozotocin-induced diabetic cardiomyopathy. Transl Res. 2019;208:1–14. doi:10.1016/j.trsl.2019.01.005
10. Lee SH, Choi JH. Involvement of immune cell network in aortic valve stenosis: communication between valvular interstitial cells and immune cells. Immune Netw. 2016;16(1):26–32. doi:10.4110/in.2016.16.1.26
11. Luo Y, Zhang H, Yu J, Wei L, Li M, Xu W. Stem cell factor/mast cell/CCL2/monocyte/macrophage axis promotes Coxsackievirus B3 myocarditis and cardiac fibrosis by increasing Ly6Chigh monocyte influx and fibrogenic mediators production. Immunology. 2022;167(4):590–605. doi:10.1111/imm.13556
12. Akin C, Siebenhaar F, Wechsler JB, Youngblood BA, Maurer M. Detecting changes in mast cell numbers versus activation in human disease: a roadblock for current biomarkers? J Allergy Clin Immunol Pract. 2024;12(7):1727–1737. doi:10.1016/j.jaip.2024.03.010
13. Pastorello EA, Farioli L, Losappio LM, et al. Serum tryptase detected during acute coronary syndrome is significantly related to the development of major adverse cardiovascular events after 2 years. Clin Mol Allergy. 2015;13(1):14. doi:10.1186/s12948-015-0013-0
14. Erdogan O, Gul C, Altun A, Ozbay G. Increased immunoglobulin E response in acute coronary syndromes. Angiology. 2003;54(1):73–79. doi:10.1177/000331970305400109
15. Chen S, Mu D, Cui M, et al. Dynamic changes and clinical significance of serum tryptase levels in STEMI patients treated with primary PCI. Biomarkers. 2014;19(7):620–624. doi:10.3109/1354750X.2014.960452
16. Chen SM, Mu D, Cui M, Ren C, Zhang S, Guo LJ. [Relationship between serum histamine levels and ST-segment resolution in patients with acute myocardial infarction treated with primary percutaneous coronary intervention]. Beijing da Xue Xue Bao Yi Xue Ban. 2014;46(6):875–878.
17. Poto R, Marone G, Galli SJ, Varricchi G. Mast cells: a novel therapeutic avenue for cardiovascular diseases? Cardiovasc Res. 2024;120(7):681–698. doi:10.1093/cvr/cvae066
18. Keller AM, Clancy RM, Barr ML, Marboe CC, Cannon PJ. Acute reoxygenation injury in the isolated rat heart: role of resident cardiac mast cells. Circ Res. 1988;63(6):1044–1052. doi:10.1161/01.res.63.6.1044
19. Frangogiannis NG, Lindsey ML, Michael LH, et al. Resident cardiac mast cells degranulate and release preformed TNF-alpha, initiating the cytokine cascade in experimental canine myocardial ischemia/reperfusion. Circulation. 1998;98(7):699–710. doi:10.1161/01.cir.98.7.699
20. Tchougounova E, Pejler G, Abrink M. The chymase, mouse mast cell protease 4, constitutes the major chymotrypsin-like activity in peritoneum and ear tissue. A role for mouse mast cell protease 4 in thrombin regulation and fibronectin turnover. J Exp Med. 2003;198(3):423–431. doi:10.1084/jem.20030671
21. Aldi S, Robador PA, Tomita K, Di Lorenzo A, Levi R. IgE receptor-mediated mast-cell renin release. Am J Pathol. 2014;184(2):376–381. doi:10.1016/j.ajpath.2013.10.016
22. Frangogiannis N. Transforming growth factor-beta in tissue fibrosis. J Exp Med. 2020;217(3):e20190103. doi:10.1084/jem.20190103
23. Nazari M, Ni NC, Ludke A, et al. Mast cells promote proliferation and migration and inhibit differentiation of mesenchymal stem cells through PDGF. J Mol Cell Cardiol. 2016;94:32–42. doi:10.1016/j.yjmcc.2016.03.007
24. Ngkelo A, Richart A, Kirk JA, et al. Mast cells regulate myofilament calcium sensitization and heart function after myocardial infarction. J Exp Med. 2016;213(7):1353–1374. doi:10.1084/jem.20160081
25. Kounis NG. Kounis syndrome (allergic angina and allergic myocardial infarction): a natural paradigm? Int J Cardiol. 2006;110(1):7–14. doi:10.1016/j.ijcard.2005.08.007
26. Kaartinen M, Penttila A, Kovanen PT. Accumulation of activated mast cells in the shoulder region of human coronary atheroma, the predilection site of atheromatous rupture. Circulation. 1994;90(4):1669–1678. doi:10.1161/01.cir.90.4.1669
27. Dilsizian V, Eckelman WC, Loredo ML, Jagoda EM, Shirani J. Evidence for tissue angiotensin-converting enzyme in explanted hearts of ischemic cardiomyopathy using targeted radiotracer technique. J Nucl Med. 2007;48(2):182–187.
28. Yang K, Gao R, Chen H, et al. Myocardial reperfusion injury exacerbation due to ALDH2 deficiency is mediated by neutrophil extracellular traps and prevented by leukotriene C4 inhibition. Eur Heart J. 2024;45(18):1662–1680. doi:10.1093/eurheartj/ehae205
29. Varricchi G, Raap U, Rivellese F, Marone G, Gibbs BF. Human mast cells and basophils-How are they similar how are they different? Immunol Rev. 2018;282(1):8–34. doi:10.1111/imr.12627
30. Beyens M, Toscano A, Ebo D, Gülen T, Sabato V. Diagnostic significance of tryptase for suspected mast cell disorders. Diagnostics. 2023;13(24):3662. doi:10.3390/diagnostics13243662
31. Ordoqui E, Zubeldia JM, Aranzabal A, et al. Serum tryptase levels in adverse drug reactions. Allergy. 1997;52(11):1102–1105. doi:10.1111/j.1398-9995.1997.tb00182.x
32. Laroche D, Vergnaud MC, Sillard B, Soufarapis H, Bricard H. Biochemical markers of anaphylactoid reactions to drugs. Comparison of plasma histamine and tryptase. Anesthesiology. 1991;75(6):945–949. doi:10.1097/00000542-199112000-00004
33. CADTH Health Technology Review. Retesting Intervals for Tryptase: Rapid Review. Canadian Agency for Drugs and Technologies in Health; 2024.
34. Gao N, Qi X, Dang Y, et al. Establishment and validation of a risk model for prediction of in-hospital mortality in patients with acute ST-elevation myocardial infarction after primary PCI. BMC Cardiovasc Disord. 2020;20(1):513. doi:10.1186/s12872-020-01804-7
35. Nienhuis MB, Ottervanger JP, de Boer MJ, et al. Prognostic importance of creatine kinase and creatine kinase-MB after primary percutaneous coronary intervention for ST-elevation myocardial infarction. Am Heart J. 2008;155(4):673–679. doi:10.1016/j.ahj.2007.11.004
36. Morrow DA, Antman EM, Charlesworth A, et al. TIMI risk score for ST-elevation myocardial infarction: a convenient, bedside, clinical score for risk assessment at presentation: an intravenous nPA for treatment of infarcting myocardium early II trial substudy. Circulation. 2000;102(17):2031–2037. doi:10.1161/01.cir.102.17.2031
37. Aldujeli A, Haq A, Hamadeh A, et al. A comparison of risk scores’ long-term predictive abilities for patients diagnosed with ST elevation myocardial infarction who underwent early percutaneous coronary intervention. Scand Cardiovasc J. 2022;56(1):56–64. doi:10.1080/14017431.2022.2066718
38. Meng S, Sun X, Juan Z, et al. Clemastine fumarate attenuates myocardial ischemia reperfusion injury through inhibition of mast cell degranulation. Front Pharmacol. 2021;12:704852. doi:10.3389/fphar.2021.704852
39. Erdogan O, Altun A, Gazi S, Ozbay G. Loratidine improves ischemic parameters of exercise stress test in patients with acute myocardial infarction. Am Heart J. 2004;148(6):e24. doi:10.1016/j.ahj.2004.04.048
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Systemic Inflammatory Response Index and Pan-Immune-Inflammation-Value with Long-Term Adverse Cardiovascular Events in ST-Segment Elevation Myocardial Infarction Patients After Primary Percutaneous Coronary Intervention
Liu Y, Liu J, Liu L, Cao S, Jin T, Chen L, Wu G, Zong G
Journal of Inflammation Research 2023, 16:3437-3454
Published Date: 14 August 2023