")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 17
Two-Stage Crestal Sinus Elevation Using Osseodensification Technique for Single Molar Restoration: A Case Report
Authors AlRowis R
Received 1 January 2025
Accepted for publication 12 March 2025
Published 27 March 2025 Volume 2025:17 Pages 201—207
DOI https://doi.org/10.2147/CCIDE.S515234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Raed AlRowis
Department of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh 11545, Saudi Arabia
Correspondence: Raed AlRowis, Department of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh 11545, Saudi Arabia, Email [email protected]
Abstract: This report presents a two-stage approach for crestal sinus elevation using the osseodensification technique in a case of severe vertical bone deficiency (< 3 mm). Traditional approaches to maxillary sinus elevation with less than 3 mm of residual bone height typically require a lateral window technique. A 55-year-old male patient presented with a missing maxillary right first molar with residual bone height of 2 mm. The treatment involved: Stage 1: Crestal sinus elevation using osseodensification with Versah burs and allograft placement. Stage 2: After 6 months of healing, placement of a Straumann Bone Level Tapered implant (4.1 × 10mm) with 35 Ncm insertion torque and final prosthetic restoration was started 4 months after implant placement. Then, follow-up at 12 months demonstrated stable peri-implant tissues, maintained bone levels, and excellent patient satisfaction. Radiographic evaluation showed uniform bone formation around the implant and maintained sinus floor elevation. The case demonstrates that osseodensification can provide a predictable alternative to lateral window approaches even in cases with severe vertical bone deficiency (< 3 mm), offering reduced invasiveness with enhanced bone density and favorable clinical outcomes.
Keywords: dental implant, osseodensification, minimally invasive surgery, bone grafting, single tooth replacement
Introduction
Dental implants are regarded as the gold standard for replacing missing teeth due to their predictable long-term outcomes and excellent functional restoration. However, implant placement in the posterior maxilla presents unique challenges arising from vertical and horizontal bone loss patterns commonly associated with this region.1 Vertical bone loss is often attributed to sinus pneumatization, a natural process that accelerates after tooth loss and aging, and addressing these anatomical limitations often necessitates pre-implant surgical preparation, such as external or internal sinus elevation procedures, sometimes supplemented with bone grafting.2 The development of the sinus elevation techniques covers more than five decades, during which two main approaches were developed: external (lateral window) and internal (crestal) sinus elevation techniques.
Whyte and Boeddinghaus3 stated that the maxillary sinus houses critical anatomical structures, such as the septum, antral artery, and ostium. Vogiatzi et al4 identified that numerous pathological and anatomical variations like rhinosinusitis, septae, and variable degrees of pneumatization that significantly influence surgical outcomes. Preoperative computed tomography has thus become indispensable for accurate diagnosis and surgical planning.
The elevation of the maxillary sinus floor was first envisioned by Boyne and James5 in 1980, leading to the development of two surgical approaches: the lateral window technique and the crestal osteotome approach.6 Even though the osteotome technique is less invasive but presents drawbacks, such as patient discomfort and challenges in assessing membrane integrity.7
Thus, a major breakthrough came through recent developments in sinus elevation techniques which have included magnetic mallets, piezoelectric surgery, and most notably, osseodensification. Introducing magnetic mallets has provided an alternative to traditional osteotome techniques, offering more precise control and reduced patient discomfort.8 However, the osseodensification technique, introduced in 2013 using Versah burs, has particularly revolutionized crestal sinus elevation procedures.9–11 This technique enhances bone preservation, improves implant primary stability, and reduces patient discomfort compared to conventional methods. Osseodensification achieves these outcomes by densifying bone along osteotomy walls while preserving bulk bone through compaction autografting. Thus, Versah burs, operating at 800–1500 rpm, works on compact bone particles by creating a densified layer that enhances implant stability.11
The efficacy of osseodensification was further validated by several recent clinical studies that the technique increased bone density by 30% over conventional drilling protocols, enhanced implant stability,12 and reduced sinus membrane perforation rates.13 So, this innovation represents a paradigm shift in crestal sinus elevation, significantly improving outcomes in implant dentistry.
This case report describes a novel, minimally invasive approach for maxillary sinus elevation using the osseodensification technique in a case with severe vertical bone deficiency (<3mm residual bone height). This paper presented the improved accuracy, reduced invasiveness, and promising outcomes compared to traditional lateral window approaches for posterior maxillary rehabilitation.
Case Report
A 55-year-old male patient who reported smoking 10 cigarettes per day for the past 20 years presented at the Dental Implant Clinic in September 2022 seeking a replacement for his maxillary right molar, which he lost ten years prior due to extensive dental caries. The correlation between smoking and implant success was thoroughly discussed with the patient, and a strict smoking cessation protocol was implemented. Written informed consent was obtained for the surgical procedures. The patient’s medical history was unremarkable, with no contraindications for dental implant treatment. His dental history indicated routine dental care and good oral hygiene. Ethical approval to report the case was not required. Written informed consent was obtained from the patient for publishing the case details and images.
Smoking Management
A formal smoking management protocol was established prior to and during surgery to avoid the well-documented detrimental effects of smoking on implant success. Complete cessation from smoking for a minimum of two weeks prior to surgery was enforced and sustained throughout the healing phase. Monitoring for compliance was routine at follow-up visits. Additionally, the patient was educated about the negative impact of smoking on healing and long-term implant success and that cessation should be maintained.
Radiographic Assessment
Initial CBCT imaging revealed severe maxillary sinus pneumatization with significant vertical bone loss at the implant site. The residual bone height was 2 mm from the alveolar crest to the sinus floor. However, the buccolingual bone width was adequate reaching 10 mm at crestal bone level (Figure 1). Pre-operative CBCT imaging revealed notable radiopacity in the maxillary sinus, suggesting potential sinus mucosal membrane thickening. Also, an ENT consult was obtained, where the patient was on nasal corticosteroids for one month prior to the sinus elevation.
 |
Figure 1 Pre-operative CBCT of area #16. |
Treatment Planning and Timeline
Given the severe vertical bone deficiency, a two-stage treatment approach was planned, beginning with crestal sinus elevation using osseodensification technique, followed by implant placement after healing. This approach was selected over traditional lateral window techniques for its minimally invasive nature and reduced post-operative complications.
The treatment process was initiated with the first surgery in December 2022, which was followed by a healing time of six months, and this was extended considering the history of smoking in the patient as well as the bone density. The implants were inserted in July 2023, following adequate healing. Osseointegration lasted four months, considering the posterior maxillary position and the bone density aspect. The restoration was completed in November 2023, and this was the end of the treatment process.
Surgical Procedure
The surgical procedure started with extensive pre-operative preparation of the surgical field. The patient was asked to rinse with 0.12% chlorhexidine gluconate solution for two minutes. Local anesthesia was obtained by cautious infiltration of 2% Lidocaine with 1:100,000 epinephrine in the buccal and palatal aspects of the surgical site.
A horizontal mid-crestal incision was made, and a full-thickness flap was elevated. Using Versah burs in densifying mode at 1200 rpm, the initial osteotomy was created, maintaining a 1 mm safety margin from the sinus membrane. The drill was used in a bouncing motion with copious sterile saline irrigation. The osteotomy was sequentially enlarged up to 3.3 mm while preserving bone density. The sinus floor was carefully fractured with controlled pressure, and membrane integrity was verified via the Valsalva maneuver. Grafting material (Puros® Cancellous Particulate Allograft, ZimVie Dental, Florida, USA) was incrementally introduced using a Versah bur at reduced speed 150 rpm in densifying mode with no irrigation. This created a 13 mm elevated space to accommodate a 10 mm implant. A resorbable collagen membrane was placed over the osteotomy site, and the site was closed with 4/0 ePTFE sutures.
Post-Operative Care and Instructions
Post-Operative Care Included
- Antibiotics (Augmentin 875/125 mg BID for 7 days).
- Analgesics (Ibuprofen 600mg PRN).
- Chlorhexidine mouthwash (0.12% twice daily).
- Strict smoking cessation instructions:
- Complete abstinence from smoking for at least 4 weeks post-surgery.
- Education about the risks of smoking on implant success and healing.
- Regular follow-up to monitor compliance.
- Oral hygiene instructions.
- Avoidance of actions that could displace the elevated membrane.
Radiographic Evaluation
Six months post-surgery, CBCT revealed uniform graft integration and 11 mm vertical augmentation, aligning with pre-surgical objectives. The sinus membrane remained elevated without collapse, though slight shrinkage was noted, as is expected in sinus elevation procedures Figure 2.
 |
Figure 2 Post-Operative CBCT shows sinus augmentation of area #16 at 6 months. |
Implant Placement
The second stage was performed six months post-elevation. Under local anaesthesia, a mid-crestal incision was made, and a (⌀ 4.1 × 10 mm, SLActive bone level tapered, Straumann, Switzerland) was placed with a torque of 35 Ncm. Postoperative radiographs confirmed optimal implant positioning Figure 3. The implant was submerged for four months to ensure osseointegration. After osseointegration, a healing abutment was placed, and the soft tissue was allowed to mature for two weeks. At the same time, the upper right second premolar was extracted due to restorability reason. The final restoration was a screw-retained zirconia crown, ensuring functional and aesthetic success Figure 4.
 |
Figure 3 Post-Operative PA radiograph shows implant placement of area #16. |
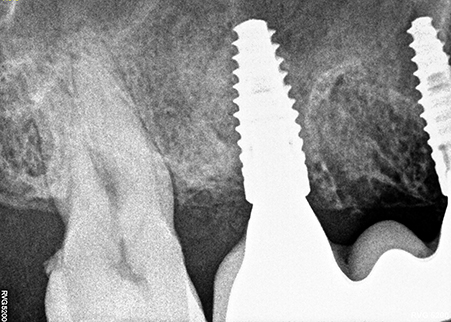 |
Figure 4 Post-Operative PA radiograph shows implant crown placement of area #16. |
Treatment Outcomes
At the 12-month follow-up, clinical examination showed no inflammation, stable keratinized tissue, and excellent pink aesthetics. Radiographs confirmed stable crestal bone levels and well-maintained sinus augmentation with complete graft integration. Minimal shrinkage of the sinus elevation was observed but did not affect the implant’s stability or the treatment outcome Figure 5.
 |
Figure 5 Post-Operative CBCT shows sinus augmentation and dental implant of area #16 at 12 months. |
Discussion
The successful rehabilitation of the posterior maxilla with dental implants poses unique challenges due to anatomical limitations and physiological bone resorption patterns. The present case report describes the effective use of the osseodensification technique for crestal sinus elevation in a case with severe vertical bone deficiency (<3 mm residual bone height), which was traditionally considered a contraindication for the crestal approach procedures.14
The management of a smoking patient presented additional challenges in this case. Recent literature has demonstrated significantly higher implant failure rates in smokers, with studies reporting up to 2.1 times increased risk.15 The patient was thoroughly informed about these risks and their impact on treatment success rates. A comprehensive smoking cessation protocol was implemented, beginning two weeks before surgery and maintained throughout the healing period. This approach aligns with current evidence suggesting that even temporary smoking cessation can improve wound healing and implant success rates.16
Maxillary atrophy and low bone density presented significant challenges for achieving optimal implant stability. The osseodensification technique proved particularly valuable in this context, allowing for improved bone density and stability in the compromised bone site. The achievement of 35 Ncm insertion torque in the grafted site is in line with Vaddamanu et al17 work which suggested that osseodensification considerably enhances implant stability in low-density bone and grafted sites. In a systematic review by Gaspar et al,18 it was found that implants placed with osseodensification have consistently shown higher insertion torque values and improved ISQ measurements than those of conventional drilling protocols.
The reason an osseodensification technique was performed instead of the classic lateral window approach is for some important considerations.18,19 Although the traditional lateral window techniques are effective, this type of surgery presents higher morbidity and longer healing time, with more complications occurring over 20–60% with an average of 30% membrane perforation cases.20 This osseodensification approach in the presented case showed strong benefits as being minimally invasive with preserved bone volume and control in membrane elevation.
Bone densification, as performed by the Versah bur system, represents a paradigm shift in osteotomy preparation. In contrast to subtractive drilling in the traditional sense, this method preserves bone by means of controlled plastic deformation and autografting of bone particles along the osteotomy walls.21 Recent studies have shown that this technique can enhance bone mineral density by up to 30% compared to conventional drilling protocols, which might also lead to improved primary stability and, presumably, shorter healing times.11
The success of this membrane elevation without perforation, in this case, with such minimal residual bone height, gives credence to the previous findings, which concluded that the hydraulic pressure generated during osseodensification results in more controlled and predictable membrane elevation when compared to traditional osteotome techniques.22,23 The gradual elevation achieved through this approach, combined with the preservation of bone architecture, likely contributed to the very stable long-term outcomes observed.
The radiographic evidence of uniform bone formation and integration of the graft at three months post-surgery is in accordance with recent histomorphometric studies that osseodensification creates an optimized regenerative environment through preserved bone volume and enhanced blood supply, which might also accelerate the healing process.24 The maintained bone levels and lack of major resorption at 12 months follow-up further support the biological benefits of this technique.
However, a few considerations deserve to be discussed, considering the applicability of this technique in a broader sense. Success, in this case, is promising but likely better understood within the realm of proper case selection and operator experience. Parameters like sinus anatomy, membrane thickness, and presence of septae could strongly influence the predictability of a crestal approach procedure.25 In this case, the radiographic finding significantly influenced our surgical approach. Special consideration was given to mucosal membrane thickness and elasticity during the elevation procedure, requiring more meticulous surgical management. This condition is not a contraindication for sinus elevation, but it only needs careful membrane elevation and an adapted healing protocol to ensure optimal sinus health. Mucosal membrane thickening had no effect on the implant success; this goes along with a recent systematic review on this matter.26 Additionally, the technique’s learning curve and need for specialized instrumentation must be considered when implementing this approach in clinical practice.
Our case demonstrates successful results at 12 months. Still, longer follow-up periods and a larger sample size would be of interest in creating definitive clinical guidelines pertaining to case selection and possible technique modifications based on site-specific conditions. Like that, combining digital planning and guided surgical approaches with osseodensification techniques is an exciting direction for future research. Advanced imaging and surgical guide fabrication will further improve the predictability of this technique in cases of minimal residual bone height.
Conclusion
This case report describes the successful application of the osseodensification technique for crestal sinus elevation in a severe vertical bone deficiency situation. The procedure’s minimally invasive nature preserved bone and reduced patient morbidity, allowing enhanced primary stability with predictable bone formation.
Disclosure
The author discloses no conflicts of interest for this work.
References
1. Andre A, Ogle OE. Vertical and horizontal augmentation of deficient maxilla and mandible for implant placement. Dent Clin. 2021;65(1):103–123. doi:10.1016/j.cden.2020.09.009
2. Tatakis DN, Chien -H-H, Parashis AO. Guided implant surgery risks and their prevention. Periodontology 2000. 2019;81(1):194–208. doi:10.1111/prd.12292
3. Whyte A, Boeddinghaus R. The maxillary sinus: physiology, development and imaging anatomy. Dentomaxillofacial Radiol. 2019;48(8):20190205. doi:10.1259/dmfr.20190205
4. Vogiatzi T, Kloukos D, Scarfe WC, Bornstein MM. Incidence of anatomical variations and disease of the maxillary sinuses as identified by cone beam computed tomography: a systematic review. Int J Oral Maxillofac Surg. 2014;29(6):1301–1314. doi:10.11607/jomi.3644
5. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613–616.
6. Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compendium. 1994;15(2):154–156. passim; quiz 162.
7. de Souza Pinto V, Couy KC, de Souza Pinto MN, Paulon P. Treatment of the mucoalveolar complex immediately after tooth extraction. 50 years of Osseointegration: Reflections and Perspectives. 2015.
8. Bennardo F, Barone S, Vocaturo C, Nucci L, Antonelli A, Giudice A. Usefulness of Magnetic Mallet in Oral Surgery and Implantology: a Systematic Review. J Pers Med. 2022;12(1):108. doi:10.3390/jpm12010108
9. Huwais S. Fluted Osteotome and Surgical Method for Use US2013/0004918. 2013.
10. Huwais S. Autografting Osteotome. Geneva, Switzerland ; 2014:WO2014/077920.
11. Huwais S, Meyer EG. A novel osseous densification approach in implant osteotomy preparation to increase biomechanical primary stability, bone mineral density, and bone-to-implant contact. Int J Oral Maxillofac Implants. 2017;32(1):27–36. doi:10.11607/jomi.4817
12. Trisi P, Berardini M, Falco A, Podaliri Vulpiani M. New osseodensification implant site preparation method to increase bone density in low-density bone: in vivo: evaluation in sheep. Implant Dent. 2016;25(1):24–31. doi:10.1097/ID.0000000000000358
13. Othman R, AbdElsamad T, Tewfik BE-DA-R. Evaluation the primary stability of dental implant placed in closed sinus-lifting using osseodensification technique. Al-Azhar J Dental Sci. 2024;27(3):397–405. doi:10.21608/ajdsm.2023.180762.1391
14. Alhayati JZ, Al-Anee AM. Evaluation of crestal sinus floor elevations using versah burs with simultaneous implant placement, at residual bone height ≥ 2.0 _ < 6.0 mm. A prospective clinical study. Oral Maxillofac Surg. 2023;27(2):325–332. doi:10.1007/s10006-022-01071-0
15. Banerjee U, Dhawan P, Rani S, Jain N. Evidence-based critical assessment of the success rate of dental implants in smokers: an umbrella systematic review. Cureus. 2024;16(9):e70067. doi:10.7759/cureus.70067
16. Bain CA. Smoking and implant failure--benefits of a smoking cessation protocol. Int J Oral Maxillofac Implants. 1996;11(6):756–759.
17. Vaddamanu SK, Saini RS, Vyas R, et al. A comparative study on bone density before and after implant placement using osseodensification technique: a clinical evaluation. Int J Implant Dent. 2024;10(1):56. doi:10.1186/s40729-024-00565-8
18. Gaspar J, Proença L, Botelho J, et al. Implant stability of osseodensification drilling versus conventional surgical technique: a systematic review. Int J Oral Maxillofac Implants. 2021;36(6):1104–1110. doi:10.11607/jomi.9132
19. Gaspar J, Mazor Z, Bonfante EA. Osseodensification technique in crestal maxillary sinus elevation—A narrative review. Clin Implant Dent Relat Res. 2025;27(1):e13399. doi:10.1111/cid.13399
20. Valentini P, Artzi Z. Sinus augmentation procedure via the lateral window technique—Reducing invasiveness and preventing complications: a narrative review. Periodontology 2000. 2023;91(1):167–181. doi:10.1111/prd.12443
21. Bleyan S, Huwais S, Neiva R. Osseodensification effective for immediate molar replacement. Compend Continuing Educ Dent. 2022;43(7):444–452.
22. Huwais S, Mazor Z, Ioannou AL, Gluckman H, Neiva R. A multicenter retrospective clinical study with up-to-5-year follow-up utilizing a method that enhances bone density and allows for transcrestal sinus augmentation through compaction grafting. Int J Oral Maxillofac Surg. 2018;33(6):1305–1311. doi:10.11607/jomi.6770
23. Samir M, Bissar MW, Abuel-Ela HA. Osseodensification versus piezoelectric internal sinus elevation (PISE) technique in delayed implant placement (a randomized controlled clinical trial). BMC Oral Health. 2024;24(1):1306. doi:10.1186/s12903-024-04964-6
24. Kotsakis GA, Romanos GE. Biological mechanisms underlying complications related to implant site preparation. Periodontology 2000. 2022;88(1):52–63. doi:10.1111/prd.12410
25. Akbari S, Taheri M, Aslroosta H, et al. Relationship of maxillary sinus mucosal thickening and residual alveolar ridge height: a CBCT analysis. Front Dent. 2022;19:19. doi:10.18502/fid.v19i19.9965
26. Amid R, Kadkhodazadeh M, Moscowchi A, Nami M. Effect of schneiderian membrane thickening on the maxillary sinus augmentation and implantation outcomes: a systematic review. J Maxillofac Oral Surg. 2021;20(4):534–544. doi:10.1007/s12663-021-01551-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.