")
Back to Journals » Journal of Inflammation Research » Volume 18
Unilateral Biportal Endoscopic Debridement and Drainage for Lumbar Infectious Spondylodiscitis: A Retrospective Study and Preliminary Results
Authors Chu R, Cui W, Chen W, Zhuang Y, Yin G, Peng W, Zhang S
Received 10 November 2024
Accepted for publication 2 March 2025
Published 13 March 2025 Volume 2025:18 Pages 3695—3704
DOI https://doi.org/10.2147/JIR.S505707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Rupeng Chu,1– 3 Wei Cui,1– 3 Wenjin Chen,1– 3 Yin Zhuang,1– 3 Guoyong Yin,4,5 Wei Peng,1– 3 Shujun Zhang1– 3
1Department of Spine Surgery, Wuxi Ninth People’s Hospital Affiliated to Soochow University, Wuxi, Jiangsu, 214063, People’s Republic of China; 2Wuxi Orthopedic Institute, Wuxi, Jiangsu, 214063, People’s Republic of China; 3Minimally Invasive Orthopedic Institute of Soochow University, Wuxi, Jiangsu, 214063, People’s Republic of China; 4Department of Orthopedics, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, 210029, People’s Republic of China; 5Jiangsu Institute of Functional Reconstruction and Rehabilitation, Jiangsu Provincial Clinical Research Institute, Nanjing, Jiangsu, 210029, People’s Republic of China
Correspondence: Wei Peng, Email [email protected] Shujun Zhang, Email [email protected]
Background: Clinical management of lumbar infectious spondylodiscitis is challenging due to its variable presentation and complex course, and its treatment remains controversial. This study aims to evaluate the clinical efficacy of unilateral biportal endoscopic (UBE) debridement and drainage for treating lumbar infectious spondylodiscitis.
Methods: We retrospectively analysed sixteen patients diagnosed with lumbar infectious spondylodiscitis who underwent UBE debridement and drainage between April 2022 and July 2023. Biopsy specimens were sent to the laboratory to identify pathogens immediately after surgeries. Clinical outcomes were assessed by the visual analog scale (VAS) scores of the back, Oswestry Disability Index (ODI), the modified MacNab criteria (MNC), and regular serological tests at pre- and post-operation.
Results: Fourteen patients (87.5%) experienced a significant improvement in their clinical symptoms. Their VAS and ODI scores significantly improved compared to those before the operation throughout the follow-up (p< 0.05). The modified MNC at the last follow-up indicated that 87.50% of these participants were rated excellent or good. Causative bacteria were identified in 13 (81.25%) of 16 biopsy specimens. At the final follow-up, all patients’ kyphotic angle changes were less than 10° without spinal instability. A 12-month follow-up CT scan revealed bony intervertebral fusion in 10 cases (62.5%). The postoperative regular serological tests were significantly improved than before surgery (p< 0.05). No recurrent infections or significant surgery-related complications were observed during postoperative follow-up.
Conclusion: UBE surgery was successful in debridement, back pain relief, and bacteriologic diagnosis of lumbar infectious spondylodiscitis. This procedure could be an effective alternative for patients when conservative treatments fail.
Keywords: lumbar infectious spondylitis, unilateral biportal endoscopy, UBE, negative pressure drainage, endoscopic debridement, minimally invasive surgery
Introduction
Infectious spondylodiscitis is characterized by infections of the disc, adjacent vertebral bodies, joints, and soft tissues and may even cause epidural abscesses, leading to significant clinical symptoms such as severe back pain, segmental instability, spinal deformity, and paralysis.1 Immunocompromised, diabetes mellitus, oncological diseases, AIDS, etc., are susceptibility factors for infectious spondylodiscitis.2,3 These conditions can lead to the spontaneous development of this disease following the spread of hematogenous infections from other inflammatory sites or following spinal surgery or diagnostic procedures.2 Despite being not uncommon, infectious spondylodiscitis has been a challenging clinical issue due to difficulties in diagnosis, identification, and controversy surrounding treatment guidelines.4,5
The primary therapeutic principles of infectious spondylodiscitis are eradicating infection, protecting neurological function, and restoring spinal stability. Conservative antibiotic treatment involves identifying pathogenic bacteria from a blood culture or CT-guided biopsy.5 However, blood cultures have poor sensitivity, and the drainage tube placed under CT-guided biopsy often fails due to viscosity of pus or necrotic tissues blocking the drainage tubes.3,6 Furthermore, it is also important to note that lumbar infectious spondylodiscitis occurs in deep tissues, and the disc’s natural anatomical structure presents a significant challenge in administering effective antimicrobial therapy; therefore, simple drug therapy does not always result in the desired results. Traditional open surgery, employing an anterior, posterior, or a combined anterior-posterior approach, has been clinically demonstrated effective for debridement and fusion.7 Nevertheless, it has obvious drawbacks, such as a lengthy surgical procedure, significant trauma, and a slow recovery following surgery.8 In addition, some patients’ general condition is suboptimal due to chronic infections, making it difficult to tolerate the incision, debridement, and drainage processes.9–12
Percutaneous endoscopic surgery, including uniaxial endoscopic surgery and unilateral biportal endoscopic (UBE) surgery, is an increasingly popular technique for treating degenerative spinal diseases and replacing more open surgeries.13 It achieves clinical effects comparable to open surgery with a reduced risk of iatrogenic injury. The uniaxial endoscopic technique has been applied to treat infectious spondylodiscitis.1,3–5 However, limited vision and maneuverability challenge thorough debridement, and irrigation cannot be accomplished through a single incision.
Recently, the UBE technique, which employs a flexible percutaneous endoscope, has been extensively utilized to treat degenerative spinal diseases.14 UBE can be manipulated continuously in a more transparent and adjustable surgical vision under high-definition arthroscopes than uniaxial endoscopic techniques.15,16 Moreover, flexible and unrestricted working tubes have also demonstrated enhanced maneuverability and convenience, thereby increased efficiency and reduced iatrogenic injury.16 Consequently, the UBE technique may theoretically provide superior results to uniaxial endoscopy when treating infectious spondylodiscitis.13,17,18
However, few studies have reported the clinical effectiveness of UBE for lumbar infectious spondylodiscitis. This study aims to describe the surgical technique and investigate the clinical and radiological outcomes associated with UBE debridement and physiological saline irrigation as a solution for lumbar infectious spondylodiscitis.
Materials and Methods
This study was approved by the ethics committee of Wuxi Ninth People’s Hospital Affiliated to Soochow University (approval number KS2024040). Written informed consent was obtained from all patients.
Patient Population
This study enrolled sixteen patients diagnosed with lumbar infectious spondylodiscitis who underwent UBE procedures at our institute between April 2022 and July 2023. A total of 10 women and 6 men participated, with an average age of 60.19 years (46~75). The diagnosis of infectious spondylodiscitis was made following a clinical examination, which included elevated values for white blood cells (WBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), X-ray and magnetic resonance imaging (MRI). The microbiology report includes the results of both microscopy and culture, as well as a list of isolated pathogens.
We included patients who fulfilled the following inclusion criteria: (1) Intolerant back and/or radiating pain caused by single lumbar infectious spondylodiscitis; (2) X-ray showed narrowing of the intervertebral disc space and variable degrees of destruction of the adjacent vertebral endplates; and MRI findings showed disc hyperintensity on T2-weighted MRI imaging and/or variable degrees of destruction of the adjacent vertebral endplates; (3) early-stage spondylodiscitis and insufficient response to conservative treatments; (4) complicated spondylodiscitis in older patients and/or with a compromising medical condition; (5) elevated ESR and CRP values. Patients who met the following criteria were excluded from the study: (1) without symptoms; (2) coexisting with large prevertebral abscesses or extensive epidural abscesses; (3) accompanied with spinal disorders of other segments that require surgical treatment together, such as thoracic spinal stenosis, kyphosis deformity etc; (4) complete paralysis of lower limbs; (5) had surgical contraindications or refused surgical treatment; and (6) had lumbar spine instability.
Surgical Technique
The patient was placed in a prone position after general anesthesia. The lesioned intervertebral space was located by fluoroscopy. We selected the side with the most severe compression for the surgical approach. The inner edge of the pedicle was used as a vertical reference line, and the working portal incision was made at the upper edge of the lower lamina. The viewing portal was about 2.5–3 cm above the working portal, with adjustments made based on the thickness of the soft tissue. Furthermore, the position of the viewing and working portals on the right side was slightly lower than on the left side. Then, a sequential dilator was used to expand the portals. Intraoperative fluoroscopy confirmed the sequential dilators converged on the lesioned intervertebral space. The plasma radiofrequency was used for bleeding control and soft tissue separation from the bone surface, and a preliminary workspace was established (Figure 1A).
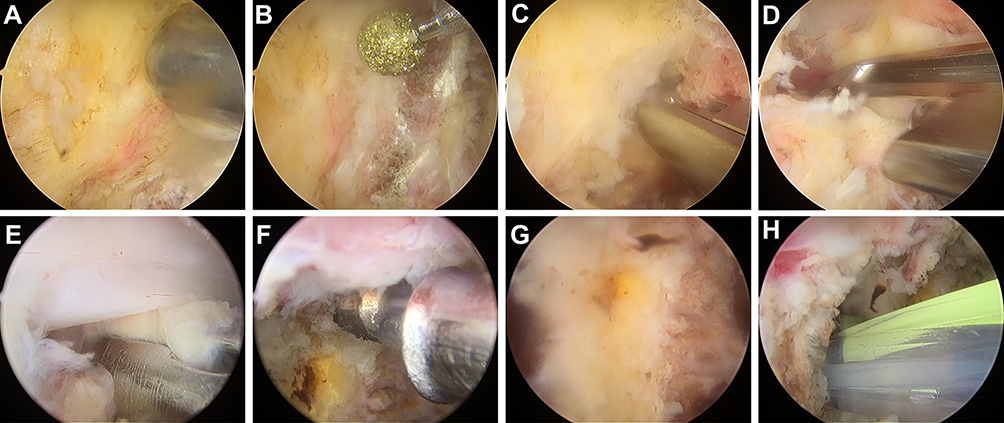 |
Figure 1 Intraoperative endoscopic images of the UBE procedure. (A) Bleeding control and soft tissue detachment were performed with a bipolar radiofrequency instrument. (B and C) A high-speed diamond burr and Kerrison rongeurs were used to remove the lamina to expose the attachment of the LF. (D) Kerrison rongeurs were employed to remove the LF. (E) The infectious disc was removed with a nucleus clamp. (F) Plasma radiofrequency removed the necrotic tissue and abscess wall around the lesion. (G) Thorough debridement was achieved. (H) Negative-pressure drainage was placed in the infectious disc space. |
Hemilaminectomy was performed using a diamond burr and Kerrison rongeurs along the inferomedial edge of the cranial lamina until the attachment of the cephalad of ligamentum flavum (LF) was reached (Figure 1B and C). For more efficient bone removal, the burr should still along the disarticulation of LF. Further drilling along the superior articular processes’ (SAP) medial edge and the caudal lamina’s rostral edge until the inferior LF’s attachment was reached. An intraspinal abscess requires an expanded bone window extending 2–3 mm beyond the abscess border. After bone drilling, the deep LF layer’s superior and inferior attachments were released, and LF was removed en bloc (Figure 1D).
Then, a blunt dissector can be used to carefully detach the infected disc and dural sac, as inflammation can cause adhesions between them. Nucleus pulposus forceps were employed to remove the infected nucleus pulposus, inflammatory granulation tissue, and damaged endplate tissue (Figure 1E). Plasma radiofrequency was applied to remove the necrotic tissue and abscess wall surrounding the lesion. Saline was employed to flush the intervertebral space consistently (Figure 1F). Plasma radiofrequency was used to remove the necrotic tissue and abscess wall around the lesion, and the intervertebral space was continuously flushed with saline. Finally, after checking the nerve roots and dural sacs without obvious compression (Figure 1G), one drainage tube was placed through the intervertebral foraminal channel into the intervertebral disc space and fixed (Figure 1H). The endoscope and the working channel were withdrawn, and the incision was closed. Tissues from the lesions removed intraoperatively were sent for pathological examination and cultured for bacterial growth.
Outcome Assessment
The visual analog scale (VAS) scores of the back, Oswestry Disability Index (ODI), the modified MacNab criteria (MNC), and regular serological tests were used to assess the effectiveness at pre-operation, post-operation (1 day, 1 week, 1 month and 3 months after surgery), and final visit. Following UBE surgery, biopsy specimens were sent to the laboratory to isolate, culture, and identify pathogens. The MNC evaluates clinical efficiency with “Excellent” (patient symptom-free, able to resume everyday life and work), “Good” (slight symptoms remain, activity slightly limited, no effect on life and work), “Fair” (some symptom relief, activity significantly limited, life and work affected) or “Poor” (post-operation symptoms the same or worse as pre-operation symptoms).19
Statistical Analysis
All the statistical analyses were conducted using SPSS version 23.0. Descriptive data are presented as the means and SDs. Student’s t tests were used to compare continuous variables between two groups when the data were continuous, normally distributed, and homoscedastic. Chi-square tests and Fisher’s exact tests were applied to evaluate differences between the two groups in other categorical variables. Differences during the postoperative follow-up period were analyzed by one-way variance analysis. p< 0.05 was considered to indicate statistical significance.
Results
In this study, 16 patients met the inclusion criteria without exclusion criteria, and their medical records were studied. Table 1 summarizes these patients’ demographic information and clinical outcomes following UBE surgery. The infection levels ranged from L2/3 to L5/S1, including 3 with L2/3, 4 with L3/4, 6 with L4/5, 3 with L5/S1, 2 with postoperative infection, and 2 with epidural abscess. The mean operative time was 55.31±16.42 min (range 35~70 min), and hospital stay after surgery was 5.72±2.07 days (range 3~11 days). All patients were followed for at least 12 months; the mean follow-up was 17.64 months (12~27 months).
 |
Table 1 Patients’ Demographic Data and Clinical Outcomes |
Immediately after surgery, fourteen patients (87.5%) experienced significantly alleviated back symptoms (Supplementary Table 1). Based on their ODI scores, these patients’ lumbar function had significant improvement and remained stable throughout follow-up (p>0.05). In addition, the modified MNC at the last follow-up indicated that 87.50% of these participants were rated excellent or good, including three with exceptional outcomes and ten with favorable outcomes. The remaining two patients, who had a persistent infection and severe back pain, underwent posterior debridement with accompanying autograft interbody fusion two weeks after UBE surgery. No recurrent infection and surgery-related significant complications were found among these patients during follow-up after surgery except in 2 patients who complained of transient paresthesia in the infectious lumbar segment, which loosened in one to two weeks. Causative bacteria were isolated in 13 (81.25%) of 16 infected tissue biopsy specimens (Table 1). Nine patients were found to have staphylococcus aureus infections; 5 were oxacillin-sensitive strains, and 4 were oxacillin-resistant strains. The other four patients were infected with streptococci viridans, streptococcus pneumonia, Escherichia coli, and enterococcus faecalis, respectively. Systemic antibiotics were administered according to sensitivity studies for identifying pathogens. No pathogens were isolated from the other three patients (18.75%). Broad-spectrum antibiotics were administered to these patients after UBE surgery. Two of them had positive outcomes following surgery and recovered without significant incidents after at least 12-week broad-spectrum antibiotic treatment. Another patient suffered from persistent back pain and progressive infection after UBE surgery. This patient eventually underwent open posterior debridement and autograft interbody fusion, and the pathogen was finally identified as oxacillin-resistant Staphylococcus aureus (ORSA).
Fourteen (87.50%) patients responded positively to UBE surgery and were successfully treated with injectable antibiotics or full-course antimicrobial chemotherapy (Figure 2). Pre- and post-operative X-rays were taken to evaluate the kyphotic angle and spinal stability. The sagittal alignment was not significantly different (mean kyphotic angle change: −1.57°), and all patients had a kyphotic angle change of less than 10° at the final follow-up (Table 2). Although all cases’ sagittal X-rays showed decreased disc height during follow-up, no patient had spinal instability. A 12-month follow-up CT scan revealed bony intervertebral fusion in 10 cases (62.5%). Table 3 presents the changes in serological values pre- and post-operative surgery in the 14 successfully treated patients. In these patients, elevated CRP values returned to normal ranges within one to six weeks (average 4.2 weeks) (Supplementary Table 2). In contrast, elevated ESR values decreased irregularly to half their pre-treatment levels within 3 to 6 weeks (mean 5.1 weeks) (Supplementary Table 3). In addition, WBC count was elevated in only seven (43.75%) of these patients, which seemed to be a relatively low likelihood of spinal infection (Supplementary Table 4).
 |
Table 2 Kyphotic Angle Change in Infected Level |
 |
Table 3 Pre- and Post-Operative Clinical Outcomes and Serological Detections |
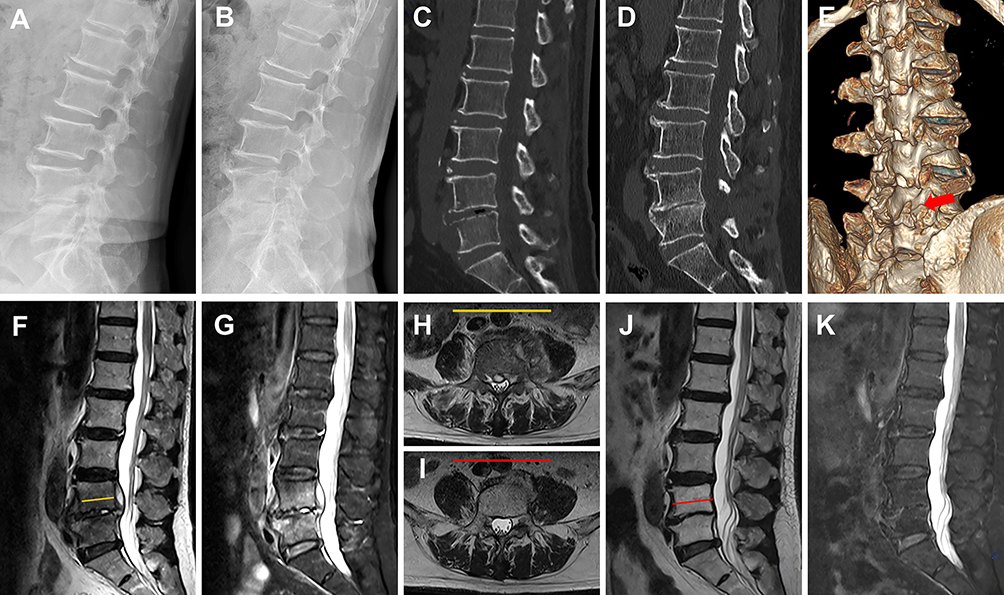 |
Figure 2 Pre-and postoperative X-ray, magnetic resonance imaging (MRI), and computed tomography (CT) scans. (A and B) Preoperative and 12 months follow-up X-rays. At the left L4/5 level, the intervertebral space narrowed. (C and D) Preoperative and 12 months follow-up sagittal CT images of the lumbar spine show that the bony fusion was achieved. (E) Postoperative 3-dimensional CT image. (F–K) Preoperative and 12 months follow-up sagittal and axial MRI scans showed that the infectious lesion had recovered, and the epidural abscess had disappeared. The yellow and red lines represent the axial planes in (H and I, respectively). |
Discussion
Infectious lumbar spondylodiscitis is on the rise, particularly among elderly, immunocompromised, and comorbid patients.5 The disease manifests in various forms and has a complex course, making diagnosis and treatment difficult.4,5 There is substantial evidence that conventional open surgery treats lumbar infectious spondylodiscitis safely and effectively.20 Recently, minimally invasive surgery has gained popularity and gradually replaced traditional surgery to some extent, thereby reducing many adverse outcomes associated with conventional surgery.1,3–5 UBE has advanced significantly as a minimally invasive technique due to its high efficiency, extensive decompression, flexible surgical field, and gentle learning curve.14–16 In this study, we evaluated the clinical efficacy of UBE debridement and drainage for treating lumbar infectious spondylodiscitis.
Conservative therapy with sensitive antibiotics, nutritional support, and bed rest is adequate for patients with minor damage or in the early stages of lumbar infectious spondylodiscitis. However, blood cultures have inferior sensitivity, lumbar infectious spondylodiscitis occurs in a deep location, and the disc’s natural anatomical structure makes it difficult to administer an effective antimicrobial therapy; therefore, simple drug therapy does not always produce the desired result.3,6 CT-guided drainage tube placement and biopsy is another frequently used and effective conservative treatment. However, the drainage tub often fails due to viscosity of pus or necrotic tissues blocking the drainage tubes. Histological examinations and cultures of samples taken from infection sites are the most reliable tests for determining the causative bacteria.
Nevertheless, CT-guided biopsy faces challenges in obtaining enough infected tissue, resulting in a low rate of positive bacterial culture results.6,21 This study identified causative bacteria of infected lesions in 13 of 16 patients. Among these identified cases, Staphylococcus aureus was the most common strain (9/13), and the isolation rate was consistent with previous reports such as Patel et al.22 Additionally, there were three cases with negative biopsy culture results, in which the preoperative use of antibiotics, combined bacterial pollution, and laboratory conditions against insensitive strains may be the causes. Although the postoperative bacterial culture was negative, these patients treated with 12-week broad-spectrum antibiotics following UBE surgery achieved satisfactory clinical results. In addition, WBC, CRP, and ESR significantly decreased one week after surgery compared to before. At the last follow-up, these serological examinations returned to the normal range. It’s worth noting that the elevated ESR and CRP were significantly more reliable than the increased WBC for the early diagnosis of lumbar infectious spondylodiscitis in our study.
When antibiotic treatment fails to provide satisfactory results, the spinal deformity progresses, lumbar instability develops, epidural abscesses form, or neurological damage occurs, surgical intervention may be necessary for patients with lumbar infectious spondylodiscitis.23 The traditional open surgical procedure involves anterior, lateral, and posterior debridement and bone graft fusion with internal fixation.7 These procedures can complete debridement, identify bacteria, and provide an internal solid fixation. Consequently, rapid pain relief, immediate spinal stabilization, and improved neurological functions were achieved.24 However, it comes with significant trauma, prolonged surgery time, more bleeding, slower postoperative recovery, and a high complication rate.8 Elderly patients or patients with comorbid underlying diseases often cannot tolerate it.9–12
With the advancement of spinal surgical techniques and the development of minimally invasive concepts, endoscopic techniques have been widely used to treat lumbar spine diseases.1,3–5,25 Several studies have demonstrated that patients with lumbar infectious spondylodiscitis who were insensitive to antibiotic treatment were treated with uniaxial endoscopic debridement and irrigation and drainage, with routine postoperative anti-infective treatment.1,3–5,25 These patients’ back pain was significantly relieved immediately after endoscopic surgery, and the clinical efficacy was satisfactory, although the causative pathogens could be identified in only 45% of the cases.21 These results indicate that endoscopic techniques are viable strategies.
Compared to uniaxial endoscopic techniques, UBE, a novel minimally invasive spinal technique, has several advantages, including clear and flexible surgical field, extensive decompression, and high efficiency.14 By performing UBE surgery, infected and necrotic tissue can be removed more efficiently and safely from the disc and even the epidural space. These advantages may be because arthroscopy provides a three-dimensional view and flexible surgical vision allowing surgeons to perform debridement more meticulously and prevent unnecessary injuries.15 Furthermore, UBE has a separate working and observing channel, which enables traditional instruments to be operated freely, increasing surgical instruments’ flexibility and mobility and making manipulation more convenient and movement space more extensive.26 These advantages make UBE surgery more effective at removing bony structures and debriding infected lesions. In the present study, despite the bony window being opened more extensively than a discectomy conducted with UBE surgery, the sagittal alignment was not significantly different between that before and after surgery, and all patients had a kyphotic angle change of less than 10° at final follow-up.
Moreover, over half of the cases achieved bony intervertebral fusion at the 12-month follow-up. These above results indicated that the spinal stability was not compromised after the extensive bone window was opened during UBE surgery. Thus, we can remove enough bony structures without disturbing the spine’s stable structures to perform a thorough debridement. This advantage is particularly evident in patients with lumbar infectious spondylodiscitis coexisting with epidural abscesses.
Intraoperative irrigation with large amounts of saline can wash out most pus, pathogenic bacteria, and inflammatory necrotic tissues. Further, large-diameter negative-pressure drainage can continuously suck out pathogens from the infection site following surgery. In the current study, adequate debridement with large amounts of saline irrigation and full-course specific antimicrobial treatment resulted in satisfactory outcomes. The patient was relieved of intractable back pain immediately after the procedure. VAS scores significantly decreased, and ODI scores significantly improved throughout follow-up. ESR, CRP, and WBC values at different time points postoperatively, except 1-day post-surgery, were reduced considerably than before surgery and recovered to the normal range at the final visit. No recurrent infection and surgery-related significant complications were observed among these patients during follow-up after surgery except in 2 patients who complained of transient paresthesia in the infectious lumbar segment, which alleviated in one to two weeks. At the last follow-up, the modified MNC indicated that 87.50% of these participants were rated excellent or good, which illustrated that the therapeutic effect of UBE was satisfactory.
However, for patients in poor general condition who cannot receive general anesthesia, uniaxial endoscopic surgery through the transforaminal approach under local anesthesia is more appropriate. UBE surgery is mainly performed through the interlaminar approach, the nerve roots are inevitably stretched, leading to intraoperative pain. Therefore, relief of this discomfort cannot be achieved solely through local anesthesia. In contrast, transforaminal approaches are less invasive to the nerve roots, making local anesthesia generally sufficient to alleviate intraoperative pain. Recently, interlaminar approaches have also been conducted using local anesthesia combined with intradural anesthesia.27,28 This type of anesthesia effectively and safely manages intraoperative pain during percutaneous endoscopic surgeries via the interlaminar approach. However, this combined anesthesia method may not be suitable for cases involving lumbar infectious spondylodiscitis, as the extent of lesion removal must be assessed intraoperatively, resulting in unpredictable operating time. Hence, performing uniaxial endoscopic surgery via the transforaminal approach under local anesthesia is more appropriate for patients in poor general condition who cannot receive general anesthesia since anesthesia medications can be re-administered if the procedure takes longer than anticipated.
Moreover, via the transforaminal approach, uniaxial endoscopy offers more benefits for patients with lesions limited to the discs. This technique minimizes surgical manipulation, which reduces exposure to nerve tissue and surrounding structures compared to UBE surgery, thus limiting the spread of inflammation. However, for patients presenting with an epidural abscess or extensive bone destruction, UBE surgery is more beneficial. Firstly, UBE can effectively remove a broader range of lesions due to its enhanced maneuverability and convenience. Secondly, UBE allows for simultaneous resection and irrigation, providing further benefits to the patient.
This research has some limitations that need to be considered. First, the small sample size of this study makes it necessary to conduct future research to reach a more definitive conclusion. Secondly, this research was a retrospective, non-controlled trial with no randomly assigned subjects or reasonable controls. Moreover, this was a single-center study, which might not represent the university population. Therefore, it would be necessary to extend the evaluation of this technique to a multicenter study.
Conclusion
UBE surgery was successful in debridement, relief of back pain, and bacteriologic diagnosis of lumbar infectious spondylodiscitis. This procedure could be an effective alternative for patients with an inferior response to conservative treatment.
Abbreviations
UBE, Unilateral biportal endoscopy; LF, Ligamentum flavum; SAP, Superior articular processes; WBC, white blood cell; CRP, C-reactive protein; ESR, Erythrocyte sedimentation rate; VAS, visual analog scale; ODI, Oswestry Disability Index; MNC, MacNab criteria; MRI, Magnetic resonance imaging; OSSA, oxacillin-sensitive Staphylococcus aureus; ORSA, oxacillin-resistant Staphylococcus aureus.
Data Sharing Statement
The dataset generated during this study is available from the corresponding author (SJZ and WP) upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of Wuxi Ninth People’s Hospital Affiliated to Soochow University, Wuxi, China (approval number KS2024040). All procedures were performed in accordance with the ethical standards of the Ethics Committee of the hospital and under the guidelines of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all patients.
Consent for Publication
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient.
Acknowledgments
We are grateful to the patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the General Project of Wuxi Municipal Health Commission in 2020 (grant number M202002) and the Science and Technology Bureau of Wuxi (Nos. K20221063 and Y20222029).
Disclosure
The authors declare that there are no competing interests in this work.
References
1. Choi SH, Koo JW, Hur JM, Kang CN. A new surgical strategy for infective spondylodiscitis: comparison between the combined antero-posterior and posterior-only approaches. Spine. 2020;45(19):E1239–E1248. doi:10.1097/BRS.0000000000003544
2. Chung TC, Yang SC, Chen HS, Kao YH, Tu YK, Chen WJ. Single-stage anterior debridement and fibular allograft implantation followed by posterior instrumentation for complicated infectious spondylitis: report of 20 cases and review of the literature. Medicine. 2014;93(27):e190. doi:10.1097/MD.0000000000000190
3. Wang X, Zhou S, Bian Z, et al. Unilateral percutaneous endoscopic debridement and drainage for lumbar infectious spondylitis. J Orthop Surg Res. 2018;13(1):306. doi:10.1186/s13018-018-1009-5
4. Yang SC, Fu TS, Chen HS, Kao YH, Yu SW, Tu YK. Minimally invasive endoscopic treatment for lumbar infectious spondylitis: a retrospective study in a tertiary referral center. BMC Musculoskelet Disord. 2014;15:105. doi:10.1186/1471-2474-15-105
5. Lin IH, Lin CY, Chang CC, et al. Percutaneous endoscopic surgery alone to treat severe infectious spondylodiscitis in the thoracolumbar spine: a reparative mechanism of spontaneous spinal arthrodesis. Pain Physician. 2022;25(2):E299–E308.
6. Iwata A, Ito M, Abumi K, et al. Fungal spinal infection treated with percutaneous posterolateral endoscopic surgery. J Neurol Surg a Cent Eur Neurosurg. 2014;75(3):170–176. doi:10.1055/s-0032-1329268
7. Connor DE, Chittiboina P, Caldito G, Nanda A. Comparison of operative and nonoperative management of spinal epidural abscess: a retrospective review of clinical and laboratory predictors of neurological outcome. J Neurosurg Spine. 2013;19(1):119–127. doi:10.3171/2013.3.SPINE12762
8. Shousha M, Heyde C, Boehm H. Cervical spondylodiscitis: change in clinical picture and operative management during the last two decades. A series of 50 patients and review of literature. Eur Spine J. 2015;24(3):571–576. doi:10.1007/s00586-014-3672-5
9. DiGiorgio AM, Stein R, Morrow KD, Robichaux JM, Crutcher CL, Tender GC. The increasing frequency of intravenous drug abuse-associated spinal epidural abscesses: a case series. Neurosurg Focus. 2019;46(1):E4. doi:10.3171/2018.10.FOCUS18449
10. Lu YA, Sun WC, Kuo G, et al. Epidemiology and outcomes of infectious spondylodiscitis in hemodialysis patients. Spine. 2018;43(12):869–876. doi:10.1097/BRS.0000000000002443
11. Dubost JJ, Lopez J, Pereira B, et al. Primary infectious spondylodiscitis in 51 patients over 75 years old: a comparative study. Med Clin. 2018;150(10):371–375. doi:10.1016/j.medcli.2017.07.027
12. Waheed G, Soliman MAR, Ali AM, Aly MH. Spontaneous spondylodiscitis: review, incidence, management, and clinical outcome in 44 patients. Neurosurg Focus. 2019;46(1):E10. doi:10.3171/2018.10.FOCUS18463
13. Heo DH, Lee DC, Park CK. Comparative analysis of three types of minimally invasive decompressive surgery for lumbar central stenosis: biportal endoscopy, uniportal endoscopy, and microsurgery. Neurosurg Focus. 2019;46(5):E9. doi:10.3171/2019.2.FOCUS197
14. Hwa Eum J, Hwa Heo D, Son SK, Park CK. Percutaneous biportal endoscopic decompression for lumbar spinal stenosis: a technical note and preliminary clinical results. J Neurosurg Spine. 2016;24(4):602–607. doi:10.3171/2015.7.SPINE15304
15. Park JH, Jun SG, Jung JT, Lee SJ. Posterior percutaneous endoscopic cervical foraminotomy and diskectomy with unilateral biportal endoscopy. Orthopedics. 2017;40(5):e779–e783. doi:10.3928/01477447-20170531-02
16. Jiang HW, Chen CD, Zhan BS, Wang YL, Tang P, Jiang XS. Unilateral biportal endoscopic discectomy versus percutaneous endoscopic lumbar discectomy in the treatment of lumbar disc herniation: a retrospective study. J Orthop Surg Res. 2022;17(1):30. doi:10.1186/s13018-022-02929-5
17. Aygun H, Abdulshafi K. Unilateral biportal endoscopy versus tubular microendoscopy in management of single level degenerative lumbar canal stenosis: a prospective study. Clin Spine Surg. 2021;34(6):E323–E328. doi:10.1097/BSD.0000000000001122
18. Deng Y, Yang M, Xia C, Chen Y, Xie Z. Unilateral biportal endoscopic decompression for symptomatic thoracic ossification of the ligamentum flavum: a case control study. Int Orthop. 2022;46(9):2071–2080. doi:10.1007/s00264-022-05484-0
19. Li M, Meng H, Du J, Tao H, Luo Z, Wang Z. Management of thoracic myelopathy caused by ossification of the posterior longitudinal ligament combined with ossification of the ligamentum flavum-a retrospective study. Spine J. 2012;12(12):1093–1102. doi:10.1016/j.spinee.2012.10.022
20. Gregori F, Grasso G, Iaiani G, Marotta N, Torregrossa F, Landi A. Treatment algorithm for spontaneous spinal infections: a review of the literature. J Craniovertebr Junction Spine. 2019;10(1):3–9. doi:10.4103/jcvjs.JCVJS_115_18
21. Haaker RG, Senkal M, Kielich T, Kramer J. Percutaneous lumbar discectomy in the treatment of lumbar discitis. Eur Spine J. 1997;6(2):98–101. doi:10.1007/BF01358740
22. Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014;14(2):326–330. doi:10.1016/j.spinee.2013.10.046
23. Rohde V, Meyer B, Schaller C, Hassler WE. Spondylodiscitis after lumbar discectomy. Incidence and a proposal for prophylaxis. Spine. 1998;23(5):615–620. doi:10.1097/00007632-199803010-00016
24. Tong YJ, Liu JH, Fan SW, Zhao FD. One-stage debridement via oblique lateral interbody fusion corridor combined with posterior pedicle screw fixation in treating spontaneous lumbar infectious spondylodiscitis: a case series. Orthop Surg. 2019;11(6):1109–1119. doi:10.1111/os.12562
25. Wang SF, Tsai TT, Li YD, et al. Percutaneous Endoscopic Interbody Debridement and Fusion (PEIDF) decreases risk of sepsis and mortality in treating infectious spondylodiscitis for patients with poor physical status, a retrospective cohort study. Biomedicines. 2022;10(7):1659. doi:10.3390/biomedicines10071659
26. Merter A, Karaeminogullari O, Shibayama M. Comparison of radiation exposure among 3 different endoscopic diskectomy techniques for lumbar disk herniation. World Neurosurg. 2020;139:e572–e579. doi:10.1016/j.wneu.2020.04.079
27. Guan Y, Huang T, An G, et al. Percutaneous endoscopic interlaminar lumbar discectomy with local anesthesia for L5-S1 disc herniation: a feasibility study. Pain Physician. 2019;22(6):E649–e654.
28. Feng WL, Yang JS, Wei D, et al. Gradient local anesthesia for percutaneous endoscopic interlaminar discectomy at the L5/S1 level: a feasibility study. J Orthop Surg Res. 2020;15(1):413. doi:10.1186/s13018-020-01939-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.