")
Back to Journals » Research and Reports in Urology » Volume 17
Urological Manifestation of Mpox Virus: A Scoping Review
Authors Mantica G, Drocchi G , Chierigo F , Granelli G, Trani G, Paraboschi I, Alba S, Ambrosini F, De Klerk C , Riccardi N , Nozza S, Van der Merwe A , Terrone C
Received 14 February 2025
Accepted for publication 17 May 2025
Published 24 May 2025 Volume 2025:17 Pages 175—184
DOI https://doi.org/10.2147/RRU.S519803
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Guglielmo Mantica,1 Giovanni Drocchi,1 Francesco Chierigo,2 Giorgia Granelli,1 Giorgia Trani,1 Irene Paraboschi,3 Stefano Alba,4 Francesca Ambrosini,1 Cecelia De Klerk,5 Niccolò Riccardi,6 Silvia Nozza,7 André Van der Merwe,5 Carlo Terrone1
1Department of Surgical and Diagnostic Integrated Sciences (DISC), University of Genoa; IRCCS Ospedale Policlinico San Martino, Genoa, Italy; 2Department of Urology, ASST Santi Paolo e Carlo, Milan, Italy; 3Department of Biomedical and Clinical Sciences, University of Milano, Milan, Italy; 4Romolo Hospital, Rocca di Neto (KR), Rocca di Neto, Italy; 5Division of Urology, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, 7100, South Africa; 6CRR-TB, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy; 7Infectious Diseases Unit, IRCCS San Raffaele Scientific Institute, Milan, Italy
Correspondence: Guglielmo Mantica, Email [email protected]
Background: Mpox primarily presents with systemic and cutaneous symptoms. However, it can also lead to urological complications, necessitating specialized attention. The aim of this scoping review is to summarize the current evidence regarding the urological manifestations of Mpox, possible complications, and available treatments.
Methods: An electronic systematic search of the current literature was conducted through the Medline and NCBI PubMed and Scopus databases on 18th August 2024. Our study search and inclusion criteria were in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9 The search terms and keywords used were: “monkeypox; Mpox” (MeSH Terms), combined with different terms: “urology”, “kidney”, “ureter”, “bladder”, “prostate”, “genitals”, “penis”, “testicles”, “urethra”, in all different possible combinations.
Results: A total of 32 articles included in the scoping review. A total of 116 patients were included, all males. The genitals were the most interested organs, associated with urethritis, while bladder and kidneys seemed to be not impacted by the disease. Patients were usually young, with a mean age of 36 years [31.5– 40 years]. The most prevalent risk factor was sexual intercourse in the days/weeks before the appearance of symptoms. All patients had a molecular confirmatory diagnosis by a polymerase chain reaction (PCR) test. Five articles out of 32 (15.6%) reported the need for surgical debridement of penile and genital lesions due to their clinical worsening. However, in most reports, patients experienced spontaneous resolution of the lesions and symptoms.
Conclusion: Awareness of Mpox and timely diagnosis are crucial for ensuring appropriate treatment and reducing the need for surgical management and the possible risk of long-term sequelae. Collaboration among dermatologists, infectious disease specialists, and urologists is pivotal to effectively managing Mpox patients.
Keywords: mpox, monkeypox, urology, UTIs, infections
Introduction
Mpox virus, formerly known as Monkeypox, is an emerging zoonotic viral disease caused by the Monkeypox virus, a member of the Poxviridae family, which has been traditionally confined to central African countries, with only sporadic cases outside this region.1,2 However, Mpox has recently spread worldwide, making it a global health concern.3,4 Usually, the clinical presentation of Mpox includes fever, headache, lymphadenopathy, and a characteristic rash that progresses through several stages (from macules to papules, vesicles, pustules, and crusts), affecting inoculum areas (eg mucosae and genitalia). Although Mpox primarily presents with systemic and cutaneous symptoms, it can also lead to urological complications, necessitating specialized attention. Furthermore, this symptomatology, which is often initially non-specific, can delay diagnosis and treatment.5–8 Correct knowledge of the possible clinical manifestations of the virus also by urologists is pivotal, not only for Mpox patient care, but also for its prevention, prompt diagnosis and reduction of contagion.
The aim of this scoping review is to summarize the current evidence regarding the urological manifestations of Mpox, possible complications, and available treatments.
Materials and Methods
Literature Search Strategy
An electronic systematic search of the current literature was conducted through the Medline and NCBI PubMed and Scopus databases on 18th August 2024. Our study search and inclusion criteria were in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.9 The search terms and keywords used were: “monkeypox; Mpox” (MeSH Terms), combined with different terms: “urology”, “kidney”, “ureter”, “bladder”, prostate”, “genitals”, “penis”, “testicles”, “urethra”, in all different possible combinations. References from commentaries, editorials, conference publications, review articles, and included studies were hand-searched and cross-referenced to ensure completeness. The research was performed independently by two Authors (GM and GD), and any disagreement was resolved by a third independent researcher (GG). The initial screening was done on the base of titles and abstracts. Any duplicates were screened, identified, and removed by Endnote (Version 9.2; Clarivate Analytics, Philadelphia, PA, USA) automated tools. The research focused on the urological manifestations of Mpox virus. Non-urological manifestations concerning kidney transplant patients were not considered relevant for this review. As regards genital lesions, only those relating to the male genitals were considered in the review.
Inclusion and Exclusion Criteria
Due to the paucity of literature in this field, also case series and case reports about “urological” clinical manifestations of Mpox virus were considered for the review. Other publications such as reviews and editorials were excluded, but screened in order to identify possible articles missed by our search strategy. The most recent publication was considered if the same patient cohort was used in more than one study. Only studies published in English were included.
Data Extraction Design
When available, the following data were extracted from each eligible study: article information (authors, study design, year), objectives, study cohort, sample size, patients’ characteristics, clinical manifestations, involved organs, follow-up, risk factors, and outcomes.
Results
The flow diagram in Figure 1 depicts the number of publications selected or excluded through the different phases of our electronic literature search. After electronic search, we identified 284 studies (118 from PubMed and 166 from Scopus). After duplicates removal we found a total of 193 studies for screening. After careful evaluation we excluded 157 articles for a total of 32 articles included in the systematic review.10–41
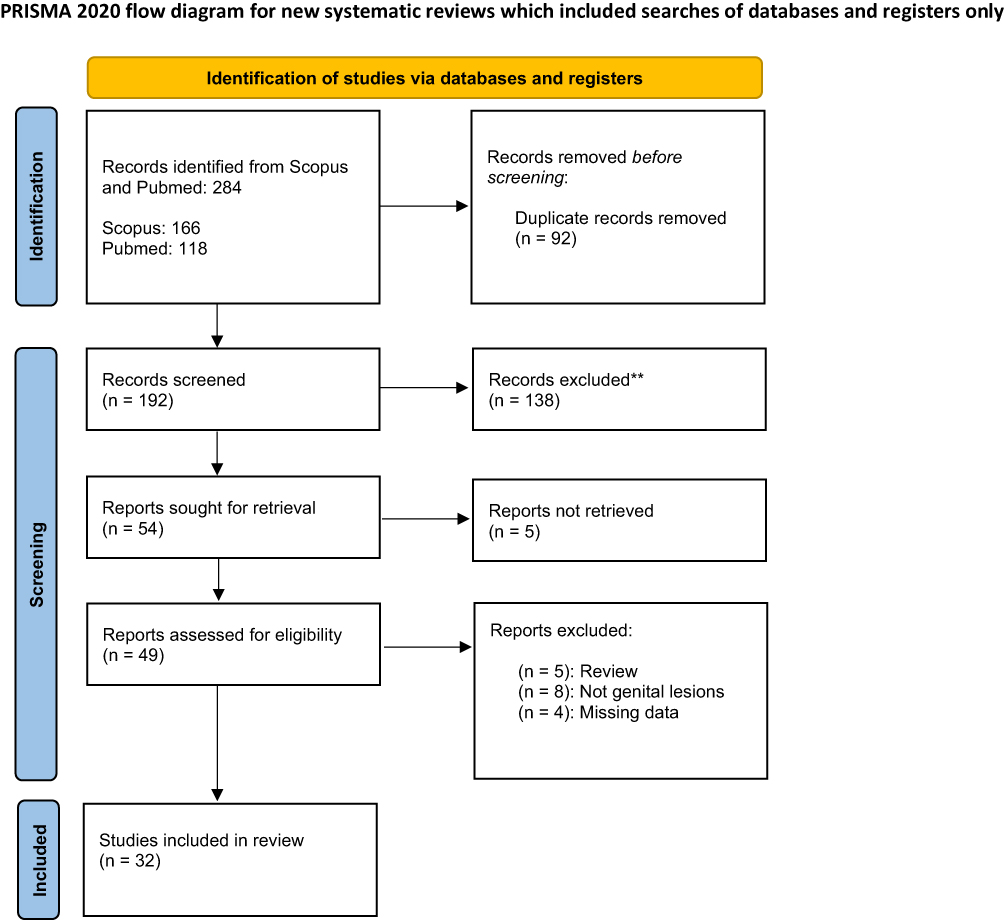 |
Figure 1 Flow diagram of publications explored. |
Type of Articles and Origin
Almost all articles were case reports or small case series, of which only 2 had more than 10 cases described. Most of articles came from US (31.2%) and Italy (18.7%). However, cases were reported from all continents apart from Oceania.
Clinical Data
A total of 116 patients were included, all males. The genitals were the most interested organs, associated with urethritis, while bladder and kidneys seemed to be not impacted by the disease (Table 1). Patients were usually young, with a mean age of 36 years [31.5–40 years]. The most prevalent risk factor was sexual intercourse in the days/weeks before the appearance of symptoms in males who have sex with males (MsM) group. Seventeen studies reported previous sexually transmitted diseases (STDs), while 14 did not report previous comorbidities. Forty patients (34.4%) had HIV co-infection. Fourteen studies reported a genital onset, 17 systemic symptoms before the appearance of genital signs, and two a concomitant onset of both genital and systemic symptoms. In those who reported subsequent genital presentation, this usually occurred after a mean 5 days [4–7 days] after the systemic one. In most cases, the urological presentation was a genital lesion (often penile/foreskin umbilicated pustules or a vesicular/macular lesion) accompanied by swelling. Groin/inguinal mono or bilateral lymphadenopathy could be present. Fever, headache, arthromyalgia, diarrhea and skin lesions were the most commonly associated signs and symptoms. In some patients, urethritis could be concomitant (see Table 1).
 |
Table 1 Overview of Included Studies |
Management and Follow-Up
When reported, all patients had a molecular confirmatory diagnosis by a polymerase chain reaction (PCR) test, obtained on swab or biopsies taken from the lesions/pustules. Five articles out of 32 (15.6%) reported the need for surgical debridement of penile and genital lesions due to their clinical worsening. However, in most reports, patients experienced spontaneous resolution of the lesions and symptoms, generally within a month of the onset of signs of the disease. Isolation and contact-tracing were fundamental to decrease disease spreading. Furthermore, in 9 studies (28.1%) patients were managed with tecovirimat, in all cases with a complete resolution. In 13 studies antibiotic prophylaxis or therapy was administered in order to avoid superinfections or to treat concomitant infections such as bacterial urethritis. All patients recovered but one who died due to multiple organ failure.
Discussion
Most urologic Mpox cases were reported as case reports or small case series, with the majority originating from the United States and Europe, while cases were reported from all continents except Oceania. These results suggest that the disease is not limited to specific geographic regions, but is a current global health issue. Although it is more prevalent in sub-Saharan Africa, reporting may be biased towards more developed countries, where healthcare infrastructures allow for better diagnosis and data reporting. Efforts should prioritize surveillance and widespread reporting systems to better characterize the real burden of the urological manifestation of Mpox.
In terms of patient demographics, it is notable that all cases involved were males, mainly with genital involvement. The disease predominantly affects the genital area, while the bladder, kidneys, and organs of the genito-urinary system are spared, possibly underlines the localized nature of the Mpox and its route of infection, at least in its early stages. MsM with a recent sexual activity were found to be at higher risk of urological Mpox. The observed median age of 36 years reflects a relatively young patient population, which may have implications for public health and sexual health education strategies. Systemic symptoms, including fever, headache, and arthromyalgia, were commonly reported prior to genital involvement, with genital symptoms occurring after a median of approximately five days from the onset of systemic signs. This temporal relationship between the onset of systemic and genital signs highlights the need for early recognition of systemic symptoms, which can aid in the diagnosis and management of the disease before genital symptoms fully manifest. However, in several cases the genital manifestation occurred before the systemic symptoms. A serious problem could also lie in the lack of ability of urologists to recognize this pathology, a problem already encountered with other uncommon infectious pathologies uncommon in developed countries, such as genitourinary tuberculosis (GUTB).42 The genital lesions observed were predominantly penile or foreskin umbilicated pustules, with vesicular or macular lesions and associated swelling being the most common clinical findings. Lymphadenopathy, particularly in the inguinal area, was also frequently noted, adding to the characteristic presentation of the disease.
The management for these patients focused primarily on confirming the diagnosis by PCR testing of lesion smears or biopsies, with treatment strategies varying depending on the severity of symptoms.
A small proportion of patients (15.6%) required surgical intervention, such as debridement of genital lesions, due to clinical worsening. In the majority of patients, however, the symptoms and lesions resolved spontaneously within a month. This underlines that the disease is self-limiting in most cases, although monitoring and early intervention remain crucial in more severe cases and/or in case of multiple comorbidities. In addition to supportive care, tecovirimat was used in a significant number of cases (28.1%), with all patients experiencing complete symptoms resolution. This highlights the potential role of antiviral therapy in managing more severe or prolonged cases. WHO recommends the use of antiviral treatment with tecovirimat in case of extensive genital lesions. However, the availability of the antiviral is limited to some expanded access program; a second choice is cidofovir i.v.43 The early initiation of the treatment is associated to a better outcome, so the early diagnosis is crucial. Antibiotic treatment may be of help in case of bacterial urethritis, with a comprehensive approach to patient management, addressing not only the primary disease but also the risk of superinfections, co-infections with other sexually transmitted diseases and proactive screening for HIV, HPV and viral hepatitis. The co-occurrence of HIV and MPOX presents unique challenges due to the potential for immunosuppression in people living with HIV (PLWH) and the impact this may have on disease severity. PLWH, especially those with a low CD4 count (<350 cells/µL) or uncontrolled HIV, are at a higher risk of developing severe MPOX.
Despite the generally favorable outcomes, there was one reported death due to multiple organ failure, despite surgical debridement and broad-spectrum antibiotic treatment. The World Health Organization (WHO) expressed global concern about the spread of Mpox and based on the recent experience with the COVID-19 pandemic, in order to alert about the potential impact of Mpox outbreaks on healthcare systems, including medical education and surgical training.44
Study Limitations
Most of the data on urologic Mpox cases came from case reports or small case series, leading to potential publication bias. The lack of large, systematic studies limits the ability to generalize findings. Differences in healthcare systems and resources across regions may influence treatment strategies and outcomes, making it difficult to compare clinical treatment methods. In addition, the true burden of the disease in underserved areas may be overlooked. The lack of longitudinal studies limits understanding of the long-term impact of urologic Mpox, including potential sequelae or recurrence. The indirect impact of Mpox outbreaks on healthcare systems, including surgical training, was not consistently addressed in the literature reviewed, leaving a gap in understanding its wider impact.
Conclusions
The current available literature provides few insights into the clinical characteristics, management, and outcomes of patients with urological manifestation of Mpox. Known risk factors such as recent intercourse in the MsM population should drive clinical suspicion. The predominance of genital involvement, the clinical course with systemic symptoms preceding genital lesions, and the need for comprehensive MST screening are key takeaways. Additionally, the role of sexual health education and public health interventions in preventing transmission, particularly in high-risk populations, should be prioritized. Awareness of Mpox and timely diagnosis are crucial for ensuring appropriate treatment and reducing the need for surgical management and the possible risk of long-term sequelae. Finally, collaboration among dermatologists, infectious disease specialists, and urologists is pivotal to effectively managing Mpox patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kaur N, Dabar J, Bassi P. Monkeypox: a re-emerging disease. Indian J Pharmacol. 2024;56(2):129–135. Epub 2024 Apr 30. PMID: 38687317; PMCID: PMC11161004. doi:10.4103/ijp.ijp_156_23
2. Lu J, Xing H, Wang C, et al. Mpox (formerly monkeypox): pathogenesis, prevention, and treatment. Signal Transduct Target Ther. 2023;8(1):458. PMID: 38148355; PMCID: PMC10751291. doi:10.1038/s41392-023-01675-2
3. Kluge H, Ammon A. Monkeypox in Europe and beyond - tackling a neglected disease together. Euro Surveill. 2022;27(24):2200482. PMID: 35713025; PMCID: PMC9205161.doi:10.2807/1560-7917.ES.2022.27.24.2200482
4. Kumar N, Acharya A, Gendelman HE, Byrareddy SN. The 2022 outbreak and the pathobiology of the monkeypox virus. J Autoimmun. 2022;131:102855. Epub 2022 Jun 25. PMID: 35760647; PMCID: PMC9534147. doi:10.1016/j.jaut.2022.102855
5. Bausch K, Mantica G, Smith EJ, et al. Genitourinary tuberculosis: a brief manual for urologists on diagnosis and treatment from the European Association of Urology Urological Infections Panel. Eur Urol Focus. 2024;10(1):77–79. Epub 2023 Aug 2. PMID: 37541917. doi:10.1016/j.euf.2023.07.006
6. Mantica G, Ambrosini F, Riccardi N, et al. Genitourinary tuberculosis: a comprehensive review of a neglected manifestation in low-endemic countries. Antibiotics. 2021;10(11):1399. PMID: 34827337; PMCID: PMC8614939. doi:10.3390/antibiotics10111399
7. Irvine A, watt J, Kurth MJ, Lamont JV, Fitzgerald P, Ruddock MW. The importance of diagnostics in the treatment of urinary tract infections in the United Kingdom. Res Rep Urol. 2024;16:327–335. PMID: 39619890; PMCID: PMC11608548. doi:10.2147/RRU.S483147
8. Raphael E, Argante L, Cinconze E, et al. Incidence and recurrence of urinary tract infections caused by uropathogenic Escherichia coli: a retrospective cohort study. Res Rep Urol. 2024;16:253–264. PMID: 39399308; PMCID: PMC11471108. doi:10.2147/RRU.S470605
9. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
10. Moreno-Matson MC, Ma O, Sáenz RD, Valero HP. Penile necrosis due to monkeypox. Urol Case Rep. 2023;51:102554. PMID: 37965126; PMCID: PMC10641105. doi:10.1016/j.eucr.2023.102554
11. Louisa Suzanna Kerkemeyer K, Bunker CB, Pang KH, Alnajjar HM, Muneer A, Freeman A. Fournier’s gangrene of the penis complicating both COVID-19- and Mpox-related genital ulceration - A case report. Int J STD AIDS. 2024;35(3):228–230. Epub 2023 Nov 6. PMID: 37931275.doi:10.1177/09564624231208728
12. Wegrzyn GH, Kilianek M, Yallapragada S, Vidal P, Dobbs RW. Genitourinary Mpox: a case report & primer for urologists. Urol Case Rep. 2023;51:102559. PMID: 37727280; PMCID: PMC10506087. doi:10.1016/j.eucr.2023.102559
13. Milano E, Belati A, De Santis L. First case of paraphimosis as a severe complication of monkeypox. Vaccines. 2022;11(1):63. PMID: 36679908; PMCID: PMC9865472. doi:10.3390/vaccines11010063
14. Urban N, Valencak J, Bauer WM, Thalhammer F, Handisurya A. Diary of human monkeypox: illustrations of the clinical course. J Eur Acad Dermatol Venereol. 2023;37(5):e672–e674. Epub 2022 Dec 11. PMID: 36461771.doi:10.1111/jdv.18802
15. Mr S, Mossack SM, Feng CL, Roadman DF, Salkowski ME, Olweny EO. Genital monkeypox superimposed on co-incident sexually transmitted infections in AIDS patient; a case report. Urol Case Rep. 2022;45:102238. PMID: 36185757; PMCID: PMC9523066. doi:10.1016/j.eucr.2022.102238
16. Gomez-Garberi M, Sarrio-Sanz P, Martinez-Cayuelas L, et al. Genitourinary lesions due to monkeypox. Eur Urol. 2022;82(6):625–630. Epub 2022 Sep 9. PMID: 36096858; PMCID: PMC9628708.doi:10.1016/j.eururo.2022.08.034
17. Chen TC. Monkeypox presenting with unusual sign of penis ulcer in a newly diagnosed human immunodeficiency virus infected patient. J Formos Med Assoc. 2024;123(2):293–294. Epub 2023 Sep 26. PMID: 37758542.doi:10.1016/j.jfma.2023.09.007
18. Lee J, McLean J, Zucker J, Brandes S, Joice G. Mpox genital lesions: a large single-center experience with intermediate follow-up. J Urol. 2023;210(3):510–516. Epub 2023 Jun 9. PMID: 37294043.doi:10.1097/JU.0000000000003579
19. Fazal H, Gandrakota N, Shackelford J, Kulshreshtha A. Mpox infection in an AIDS patient with syphilis manifesting with scrotal and penile cellulitis. J Med Virol. 2023;95(7):e28906. PMID: 37394787.doi:10.1002/jmv.28906
20. Ciccarese G, Di BA, Drago F, et al. Monkeypox virus infection mimicking primary syphilis. Infez Med. 2022;31(1):113–115. PMID: 36908381; PMCID: PMC9994820. doi:10.53854/liim-3101-16
21. Poole M, Mehrmal S, Kremer M, Guo AM, West DA. An atypical presentation of monkeypox associated with scrotal and penile shaft edema. JAAD Case Rep. 2023;33:36–38. Epub 2023 Jan 20. PMID: 36694844; PMCID: PMC9854266. doi:10.1016/j.jdcr.2022.12.018
22. Manoharan A, Braz BX, McBride A, et al. Severe monkeypox with superimposed bacterial infection in an immunocompetent patient: a case report. IDCases. 2022;30(e01626). PMID: 36345426; PMCID: PMC9622463. doi:10.1016/j.idcr.2022.e01626
23. Pérez-Martín ÓG, Hernández-Aceituno A, Dorta-Espiñeira MM, García-Hernández L, Larumbe-Zabala E. Atypical presentation of sexually-transmitted monkeypox lesions. Infect Dis. 2022;54(12):940–943. Epub 2022 Sep 14. PMID: 36102117; PMCID: PMC9527785.doi:10.1080/23744235.2022.2121420
24. Davido B, D’anglejan E, Jourdan J, Robinault A, Davido G. Monkeypox 2022 outbreak: cases with exclusive genital lesions. J Travel Med. 2022;29(6):taac077. PMID: 35699601. doi:10.1093/jtm/taac077
25. Farley R, Sarver J, Milliner B, Miller BD. Genital infection from Monkeypox virus requiring surgical debridement and scrotoplasty in an immunocompromised patient. Urol Case Rep. 2023;49:102438. Epub 2023 May 14. PMID: 37215942; PMCID: PMC10183090. doi:10.1016/j.eucr.2023.102438
26. Miyazaki Y, Adachi T. Human mpox presenting with penile edema and ulcer: a case report. J Infect Chemother. 2024;30(8):789–792. Epub 2024 Jan 11. PMID: 38218223.doi:10.1016/j.jiac.2024.01.004
27. Oiwoh SO, Tobin EA, Asogun DA, et al. Atypical presentation of mpox in Irrua environs: a case report. J Med Case Rep. 2023;17(1):492. PMID: 38007455; PMCID: PMC10676585. doi:10.1186/s13256-023-04225-0
28. Bociąga-Jasik M, Raczyńska A, Lara M, Kalinowska-Nowak A, Garlicki A. Monkeypox presenting with genital ulcers: a challenging clinical problem. Pol Arch Intern Med. 2022;132(10):16304. Epub 2022 Jul 29. PMID: 35912913. doi:10.20452/pamw.16304
29. Ramoni S, Maronese CA, Morini N, et al. Syphilis and monkeypox co-infection: coincidence, synergy or asymptomatic carriage? Travel Med Infect Dis. 2022;50:102447. Epub 2022 Sep 5. PMID: 36067937; PMCID: PMC9629038. doi:10.1016/j.tmaid.2022.102447
30. Ortiz-Martínez Y, Rodríguez-Morales AJ, Franco-Paredes C, et al. Monkeypox - a description of the clinical progression of skin lesions: a case report from Colorado, USA. Ther Adv Infect Dis. 2022;9:20499361221117726. PMID: 35910397; PMCID: PMC9335484. doi:10.1177/20499361221117726
31. Pipitò L, Caputo V, Cascio A. Verrucous penile lesions and widespread vesicular rash in a 33-year-old bisexual man. Int J Dermatol. 2023;62(5):691–693. Epub 2022 Dec 18. PMID: 36529930.doi:10.1111/ijd.16569
32. Oliveirae Silva F, Cruz AJ, Nuak J. Penile cellulitis related to mpox genital lesions. Acta Med Port. 2023;37(1):51–52. doi:10.20344/amp.19832
33. Mahtani AU, Engome YM, Haider M, et al. Paraphimosis as a complication of monkeypox infection. J Surg Case Rep. 2022;2022(11):rjac533. PMID: 36452291; PMCID: PMC9701556. doi:10.1093/jscr/rjac533
34. Quattri E, Avallone G, Maronese CA, et al. Unilesional monkeypox: a report of two cases from Italy. Travel Med Infect Dis. 2022;49:102424. Epub 2022 Aug 10. PMID: 35961491; PMCID: PMC9533888. doi:10.1016/j.tmaid.2022.102424
35. Qingqing LI, Xingdong YE, Aili GAO, et al. Monkeypox with penile papule and plaque: a case report. China J Leprosy Skin Dis. 2024;40(4):231–233.
36. Miše J. Monkeypox presenting as sudden appearance of a solitary pigmented genital lesion. Int J Dermatol. 2023;62(4):565–566. Epub 2022 Nov 2. PMID: 36323642.doi:10.1111/ijd.16481
37. Potthoff A, Brockmeyer NH, Skaletz-Rorowski A. Monkey pox: images of a clinical course. J Dtsch Dermatol Ges. 2023;21(3):283–284. Epub 2023 Feb 14. PMID: 36786070.doi:10.1111/ddg.14981
38. Contag CA, Karan A, Studemeister L, et al. Case report: mpox - not just a rash. Am J Trop Med Hyg. 2023;108(3):592–594. PMID: 36716741; PMCID: PMC9978541. doi:10.4269/ajtmh.22-0626
39. Lopes PS, Haddad GR, Miot HA. Sexually-transmitted monkeypox: report of two cases. An Bras Dermatol. 2022;97(6):783–785. Epub 2022 Sep 20. PMID: 36137892; PMCID: PMC9560761.doi:10.1016/j.abd.2022.08.002
40. Kreuter A, Grossmann M, Müller VL, et al. Monkeypox infection with concomitant penile lymphoedema. J Eur Acad Dermatol Venereol. 2023;37(3):e431–e432. Epub 2022 Aug 20. PMID: 35974448.doi:10.1111/jdv.18502
41. Turco M, Mancuso FR, Pisano L. A monkeypox virus infection mimicking primary syphilis. Br J Dermatol. 2022;187(6):e194–e195. Epub 2022 Sep 25. PMID: 36005947.doi:10.1111/bjd.21847
42. Mantica G, Van der Merwe A, Terrone C, et al. Awareness of European practitioners toward uncommon tropical diseases: are we prepared to deal with mass migration? Results of an international survey. World J Urol. 2020;38(7):1773–1786. Epub 2019 Sep 20. PMID: 31538244. doi:10.1007/s00345-019-02957-7
43. World Health Organization. Available from: https://www.who.int/news-room/fact-sheets/detail/mpox. Accessed May 20, 2025.
44. World Health Organization. Multi-country outbreak of mpox, External situation report #45.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.