")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Using QIP-MS to Guide the Timing of MRD Testing in Patients With Multiple Myeloma: A Budget Impact Analysis From the French Payer Perspective
Authors Siegfried C , Amarapala M, Leleu X, Fusfeld L
Received 1 October 2024
Accepted for publication 7 January 2025
Published 20 February 2025 Volume 2025:17 Pages 107—114
DOI https://doi.org/10.2147/CEOR.S498848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xing Lin Feng
Christian Siegfried,1 Miyuru Amarapala,1 Xavier Leleu,2 Lauren Fusfeld1
1Veranex, Boston, MA, USA; 2Department of Hematology, CHU, Poitiers, Poitiers, France
Correspondence: Christian Siegfried, CRO and Consulting Services, Veranex, 100 Federal St Suite 3302A, Boston, MA, 02110, USA, Email [email protected]
Purpose: Serum or urine protein electrophoresis (SPEP or UPEP) and immunofixation electrophoresis (SIFE or UIFE) are routinely used to detect M-proteins in MM patients. However, SPEP and SIFE are not sensitive enough to measure M-protein levels that are low but still clinically significant. This study aimed to evaluate the potential cost savings associated with using the EXENT GAM Assay, a serum-based quantitative-immunoprecipitation mass spectrometry (QIP-MS) diagnostic test instead of SIFE to guide the timing of minimal residual disease (MRD) testing for patients with multiple myeloma (MM).
Patients and Methods: A simple 2-year budget impact model was created in Excel using data from MM clinical trials and fee schedules. Patients are tested with either QIP-MS or SIFE at predetermined timepoints. If patients test negative, they will receive MRD testing. The result of the MRD test will determine if the preceding serum-based test was a true negative result (MRD test is negative) or a false negative result (MRD test is positive). Patients receiving autologous stem cell transplant (henceforth referred to as transplant) and those not receiving transplant are both eligible for one MRD test per year. MRD testing for transplant-eligible patients occurs prior to transplant and one year following transplant.
Results: Across a hypothetical population of 5154 mm patients receiving 1st-line treatment in France, using QIP-MS instead of SIFE prior to MRD testing leads to 1973 fewer false negative results and 744 more false positive results (due, in part, to the detection of residual IgG). Net savings per QIP-MS test would be € 260 or total savings of € 2,481,832.
Conclusion: This study suggests that the use of QIP-MS prior to MRD testing may be cost-saving for testing French patients with MM.
Keywords: mass spectrometry, minimal residual disease, immunofixation electrophoresis, plasma cell disorder
Introduction
Multiple myeloma (MM) is a malignancy of the blood caused by the proliferation of abnormal clonal plasma cells within the bone marrow. Monoclonal proteins (M-proteins), which are immunoglobulins produced by the abnormal plasma cells, are a marker of disease activity and can be used to diagnose MM; in France, 5425 new cases are diagnosed each year.1 M-proteins can also be used for disease monitoring following treatment of MM patients.
In current practice in France, several tests are routinely used to detect M-proteins in MM patients: serum or urine protein electrophoresis (SPEP or UPEP) and immunofixation electrophoresis (SIFE or UIFE).2 However, these tests are not sensitive enough to measure M-protein levels that are low but still clinically significant.3 Patients receiving new therapies, such as the combination of daratumumab, bortezomib, thalidomide, and dexamethasone (D-VTd) or daratumumab, bortezomib, lenalidomide, and dexamethasone (D-VRd), can generate responses deeper than SIFE can detect.4–6 Without the use of supplementary assays, therapeutic antibodies can also interfere with the results of SIFE testing, leading to false positive results.7 Consequently, patients testing negative with SIFE may be required to undergo more sensitive tests such as minimal residual disease (MRD) testing with next-generation flow cytometry (NGF) or next-generation sequencing (NGS) at sensitivities of 10−5 or 10−6 to determine the presence or absence of malignant cells.8 In newly diagnosed multiple myeloma (NDMM) patients who have achieved CR, up to 31% can still be positive via MRD testing.9
Studies demonstrate an association between improved progression-free survival (PFS) or overall survival (OS) and MRD negativity where CR is less prognostic.6,9 The use of MRD in MM recently gained unanimous support from the FDA’s Oncologic Drugs Advisory Committee (ODAC) as a surrogate primary endpoint in MM clinical trials to enable accelerated approvals of new therapies.10 The FDA’s position on MRD has sparked discussions with the European Medicines Agency (EMA), which announced it would use both cost and clinical data to make a determination on the use of MRD as a surrogate endpoint by July 1, 2024. As MRD testing transitions from clinical trials to routine clinical practice in France, more sensitive tests will be needed to detect M-proteins in the blood and reduce the additional costs and invasive bone marrow (BM) aspiration procedures associated with NGF/NGS.11–13
Noting the improved accuracy of mass spectrometry (MS) over conventional serum- or urine-based methods and MS’ ability to distinguish endogenous M-proteins from therapeutic antibodies, the International Myeloma Working Group (IMWG) has endorsed the use of MS-based tests for the monitoring of patients with MM and other plasma cell disorders.3,14 The EXENT GAM Assay (Thermo Fisher, Waltham, Massachusetts, United States), a quantitative immunoprecipitation mass spectrometry (QIP-MS) system, is a serum-based test that can detect and quantify M-proteins at much lower levels than serum immunofixation electrophoresis (SIFE) and SPEP.3,15,16 QIP-MS measures immunoglobulins G, A, and M, as well as total kappa and lambda. The lower limit of measuring interval (LLMI) for QIP-MS is 0.015 g/L, roughly ten times as sensitive as SIFE.17 By identifying proteins based on their unique isotype and mass-to-charge ratio of their light chains, QIP-MS can also distinguish between endogenous M-proteins and therapeutic antibodies.16,18
In anticipation of the potential increase in MRD testing in MM in clinical practice, this study uses a simple budget impact model to compare QIP-MS versus SIFE as a precursor to testing MRD with NGF or NGS in France.
Materials and Methods
Study Design
A two-year budget impact analysis was developed in Excel to compare the hypothetical use of SIFE or QIP-MS as a precursor to MRD testing from the French payer perspective. The French healthcare system, l’Assurance Maladie, is a mandatory-enrollment, single-payer national healthcare system which covers nearly all residents of France.19
Patients receive MRD testing only after a negative M-protein test via SIFE or QIP-MS. MRD testing is considered definitive in this model; a positive MRD assessment means the preceding M-protein test with either SIFE or QIP-MS was a false negative.
The frequency of MRD testing in the model is based on a practicing French hematologist’s clinical trial experience regarding the times MRD has been most informative in the management of patients (XL). Patients receiving autologous stem cell transplant (henceforth referred to as transplant) and those not receiving transplant are both eligible for one MRD test per year. Transplant patients are eligible for MRD testing prior to transplant and one year following transplant. Figure 1 provides an overview of the diagnostic pathway that occurs at each testing time point.
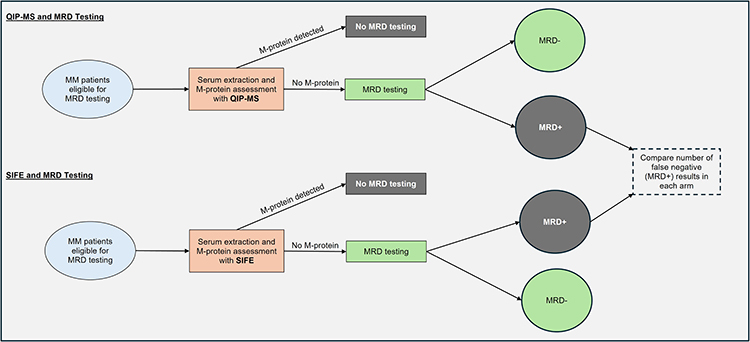 |
Figure 1 Budget Impact Model Framework. Abbreviations: QIP-MS, quantitative immunoprecipitation mass spectrometry; SIFE, serum immunofixation electrophoresis; MRD, minimal residual disease. |
Model Development
The model framework and input values were selected via a focused review of literature on PubMed, published fee schedules, and primary research with a practicing French hematologist (XL). The model includes direct costs associated with M-protein and MRD tests, extraction of blood and bone marrow aspirate, and associated physician visits. In accordance with budget impact modeling best practices, the model does not include cost discounting.20
Clinical Inputs
The number of patients entering the model is determined by the total insured population, the number of insured patients who are newly diagnosed with MM, and, finally, the percentage of those insured NDMM patients who would benefit from treatment. The true presence of disease in the model is determined by the positivity of MRD tests. These values are provided by the GEM2012MENOS65 trial, which tested NDMM patients with NGF.21 Given the short timeframe of the model and the population (newly diagnosed patients), the one-year survival rate is assumed to be the same for patients receiving transplant and those not receiving transplant. This assumption is supported by the DETERMINATION trial, which did not show a significant difference in survival between these two groups over a one-year period.22 The number of patients entering the second year of the model is multiplied by this survival rate. The clinical values are provided in Table 1.
 |
Table 1 Clinical Inputs |
Table 2 provides the sensitivity and specificity of the M-protein testing methods. These values were calculated using each test’s concordance with NGS MRD results in NDMM patients.
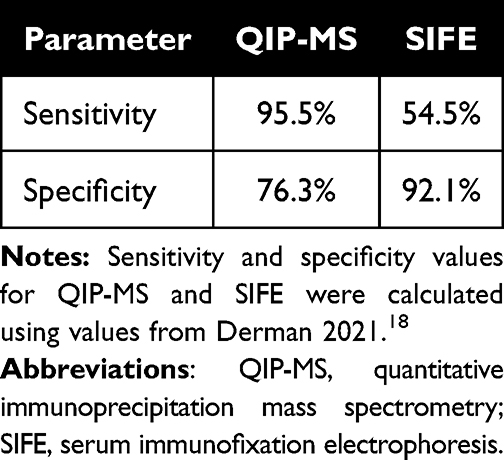 |
Table 2 Test Specifications |
Cost Inputs
Costs are from published literature as well as the Common Classification of Medical Procedures (CCAM) and National Biology Coding Table (NABM) when possible and were reviewed by a hematologist (XL). The cost of QIP-MS, provided by the manufacturer, is €90. All costs are in 2023 Euros. Additional costs can be found in Table 3
 |
Table 3 Costs |
The cost of MRD testing per patient is a weighted average of the costs of testing with NGS and NGF, based on the hematologist’s experience with the proportion of testing performed with either method and his expectations for future MRD testing in clinical practice (XL). The average cost of MRD testing includes the cost of the bone marrow aspiration and specialist visit. The proportions of testing with NGS/ NGF and the average cost of MRD testing are provided in Table 4.
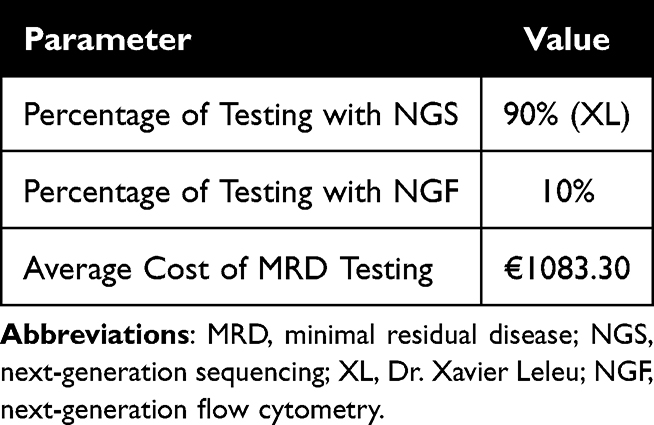 |
Table 4 Average Cost of MRD Testing |
Sensitivity Analysis
A one-way sensitivity analysis examined the effect of varying each input by ±10% of its base case value.
Results
Across a hypothetical population of 5154 mm patients receiving 1st-line treatment in France, using QIP-MS instead of SIFE prior to MRD testing leads to a reduction in premature MRD tests of 1973 and total savings of €2,481,832. Compared with SIFE, QIP-MS would produce 744 additional false positive results and 1973 fewer false negative results. Net savings per QIP-MS test would be €260. For the 2062 transplant and 3029 non-transplant patients, QIP-MS would save €993,478 and €1,488,354, respectively. Table 5 provides a breakdown of the distribution of test results, with associated costs in Table 6. Total costs by year are provided in Figure 2, with higher costs in year two when rates of underlying disease are lower.
The most influential input parameters in the one-way sensitivity analysis are the sensitivity of QIP-MS, the specificity of SIFE, the cost of MRD testing, and the specificity of QIP-MS, presented in Figure 3.
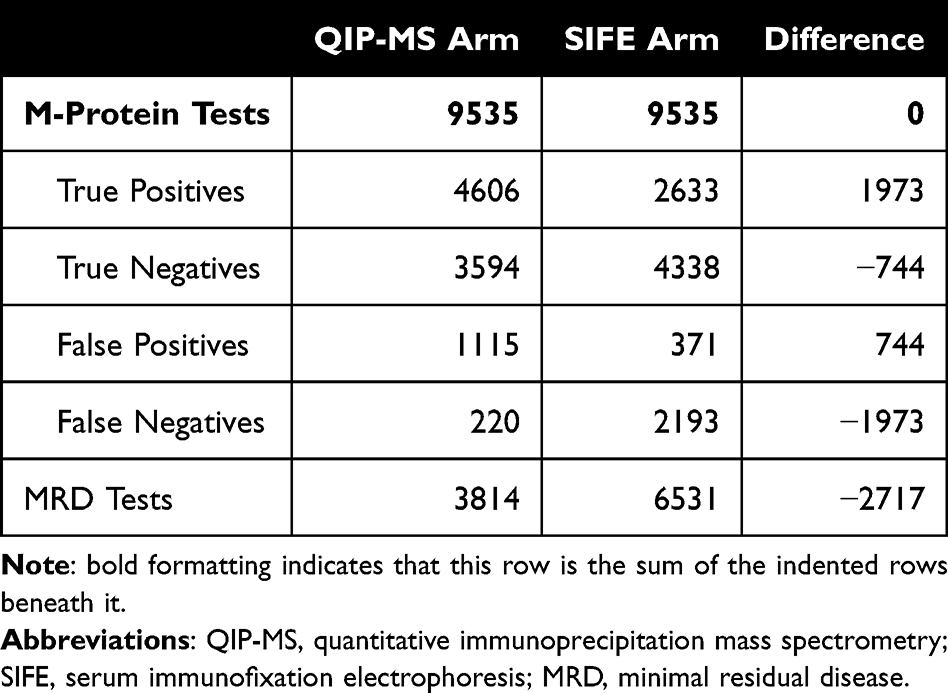 |
Table 5 Test Volume |
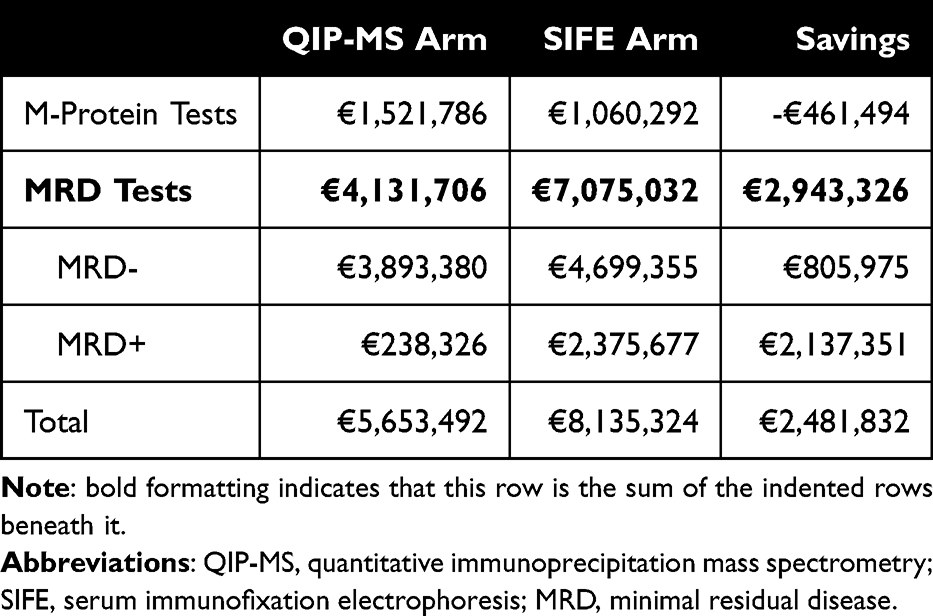 |
Table 6 Total Costs |
 |
Figure 2 Total Yearly Costs for the QIP-MS and SIFE Arms. Abbreviations: QIP-MS, quantitative immunoprecipitation mass spectrometry; SIFE, serum immunofixation electrophoresis. |
 |
Figure 3 One-Way Sensitivity Analysis (Total Savings in 000s). Abbreviations: QIP-MS, quantitative immunoprecipitation mass spectrometry; SIFE, serum immunofixation electrophoresis; MRD, minimal residual disease. Note: All input percentages must be within 0% and 100% in the model. Consequently, the one-way sensitivity analysis uses 100% as the upper limit for the sensitivity of QIP-MS and the specificity of SIFE rather than 110% times the base case value. |
Discussion
Using MRD tests to inform clinical decision-making has been established in many hematological malignancies, and clinicians are already beginning to incorporate MRD testing in MM clinical practice in several countries. For example, some clinicians in Spain review MRD results at specific times in the MM patient journey, such as prior to and following transplant, following consolidation therapy in those patients that receive it, and a year following transplant.21,29 While MRD testing is not currently a part of routine clinical practice in France, its use in MM clinical trials has been growing, and MRD testing could become part of the standard of care in the future.4
For countries using MRD testing, clinicians may be able to optimize patient assessment by first employing a blood-based test that is more sensitive than SIFE to accurately identify patients who would be eligible for MRD testing with NGS/NGF. Utilizing a sensitive test as a precursor to MRD could improve the number of accurately diagnosed MRD-negative patients and postpone invasive bone aspirations in patients who would otherwise have been subjected to premature MRD testing.
This study is the first to demonstrate the economic feasibility of using QIP-MS rather than SIFE as a precursor to MRD testing in France.
Limitations
Intended as a preliminary evaluation, this model has several limitations, including a short two-year time horizon. Clinicians confirmed, however, that this timeframe would capture most MRD testing in a patient’s journey. Any additional uses of QIP-MS for monitoring MM patients, aside from serving as a precursor to MRD testing, have been excluded from the model but could be added once data on these applications have been published. Without regular monitoring, MM patients, such as those with IgG myeloma, may have false positive test results with QIP-MS due to residual M-proteins continuing to circulate in their blood for as long as six months.15,30,31 When used regularly, QIP-MS can quantify low concentrations of M-proteins and could allow physicians to determine when IgG levels are decreasing even while the MS test result remains positive.15,30,31 Studies suggest MS can also detect disease in patients who test MRD-negative with NGF, which is likely to occur for two reasons: patients have MM proliferating outside of the bone marrow, (known as extramedullary disease) or, due to limitations on where the bone marrow aspiration can be extracted, the sample is not extracted from a region with cancerous cells.32–35 Conversely, in the roughly 1% to 3% of myeloma patients with non-secretory myeloma, QIP-MS will be unable to monitor the disease due to the absence of M-proteins in the blood. While conventional blood-based methods are also unable to detect M-proteins in patients with oligosecretory MM, which comprises roughly 2% to 3% of all MM patients, QIP-MS has demonstrated the ability to detect and monitor disease in small studies of these patients.36,37 QIP-MS’s ability to detect M-proteins in these patients is due to its LLMI of 0.0015 g/dl, which is well below the 1 g/dl threshold of serum M-protein that defines patients as oligosecretory.17,38 The model also does not incorporate treatment and patient outcomes. When patient outcomes following MS testing become available, an expanded economic model including treatments and patient outcomes would be useful to consider. Lastly, hematologists, acknowledging the potential complications and patient discomfort associated with the extraction of bone marrow, indicate that minimizing premature bone marrow aspirations would be of value to patients, but data limitations prevent the model from accounting for these improvements in quality of life.39 Patient-related outcome measures, such as quality of life, should be evaluated in future studies.
Conclusions
As evidence supporting the use of MRD in MM grows, it will be important to understand how best to incorporate MRD testing in clinical practice. This study suggests that the use of QIP-MS prior to MRD testing may be cost-saving for testing French patients with MM.
Acknowledgments
We thank Sabrina Iadicicco (Veranex) and Sabina Schadyew (Veranex) for providing several model parameters.
Disclosure
The analysis was funded by Thermo Fisher Scientific. Veranex, Inc. received consulting fees from Thermo Fisher Scientific for developing the model on which this manuscript is based. Co-authors Christian Siegfried, Miyuru Amarapala, and Lauren Fusfeld were employed by Veranex, Inc. at the time of this research.
References
1. Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.who.int/today.
2. Multiple Myeloma Research Foundation [Internet]. Diagnostic testing for multiple myeloma. Available from: https://themmrf.org/diagnosis-and-treatment/diagnostic-testing/.
3. Murray DL, Puig N, Kristinsson S, et al. Mass spectrometry for the evaluation of monoclonal proteins in multiple myeloma and related disorders: an International Myeloma Working Group Mass Spectrometry Committee report. Blood Cancer J. 2021;11(2):24. doi:10.1038/s41408-021-00408-4
4. Moreau P, Hulin C, Perrot A, et al.; Intergroupe Francophone du Myélome, the Dutch-Belgian Cooperative Trial Group for Hematology Oncology and the CASSIOPEIA Investigators. Bortezomib, thalidomide, and dexamethasone with or without daratumumab and followed by daratumumab maintenance or observation in transplant-eligible newly diagnosed multiple myeloma: long-term follow-up of the CASSIOPEIA randomised controlled Phase 3 trial. Lancet Oncol. 2024;25(8):1003–1014. Epub 2024 Jun 15. PMID: 38889735. doi:10.1016/S1470-2045(24)00282-1
5. Sonneveld P, Dimopoulos MA, Boccadoro M, et al. PERSEUS Trial Investigators. Daratumumab, bortezomib, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med. 2024;390(4):301–313. doi:10.1056/NEJMoa2312054 Epub 2023 Dec 12. PMID: 38084760.
6. Paiva B, San-Miguel J, Avet-Loiseau H. MRD in multiple myeloma: does CR really matter? Blood. 2022;140(23):2423–2428. doi:10.1182/blood.2022016170 PMID: 35560160.
7. Kirchhoff DC, Murata K, Thoren KL. Use of a daratumumab-specific immunofixation assay to assess possible immunotherapy interference at a major cancer center: our experience and recommendations. J Appl Lab Med. 2021;6(6):1476–1483. doi:10.1093/jalm/jfab055 PMID: 34293131; PMCID: PMC9487159.
8. Ferla V, Antonini E, Perini T, et al. Minimal residual disease detection by next-generation sequencing in multiple myeloma: promise and challenges for response-adapted therapy. Front Oncol. 2022;12:932852. PMID: 36052251; PMCID: PMC9426755. doi:10.3389/fonc.2022.932852
9. Munshi NC, Avet-Loiseau H, Rawstron AC, et al. Association of minimal residual disease with superior survival outcomes in patients with multiple myeloma: a meta-analysis. JAMA Oncol. 2017;3(1):28–35. doi:10.1001/jamaoncol.2016.3160 PMID: 27632282; PMCID: PMC5943640.
10. US Food & Drug Administration [Internet]. April 12, 2024 meeting of the oncologic drugs advisory committee meeting announcement. Available from: https://tinyurl.com/2rexatkp.
11. Hibbs S. This is going to hurt: revisiting the patient experience of bone marrow biopsies. Hemasphere. 2022;6(4):e710. doi:10.1097/HS9.0000000000000710
12. Gendron N, Zia Chahabi S, Poenou G, et al. Pain assessment and factors influencing pain during bone marrow aspiration: a prospective study. PLoS One. 2019;14(8):e0221534. doi:10.1371/journal.pone.0221534
13. Liptrott SJ, Botti S, Bonifazi F, et al. Management of pain and anxiety during bone marrow aspiration: an Italian national survey. Pain Manag Nurs. 2021;22(3):349–355. doi:10.1016/j.pmn.2020.09.005
14. Murray DL. Bringing mass spectrometry into the care of patients with multiple myeloma. Int J Hematol. 2022;115(6):790–798. doi:10.1007/s12185-022-03364-2
15. Eveillard M, Korde N, Ciardiello A, et al. Using MALDI-TOF mass spectrometry in peripheral blood for the follow up of newly diagnosed multiple myeloma patients treated with daratumumab-based combination therapy. Clin Chim Acta. 2021;516:136–141. doi:10.1016/j.cca.2021.01.021
16. Berlanga O, North S, Barnidge D, et al. QIP-MS: an alternative to electrophoresis to distinguish endogenous M-proteins from therapeutic monoclonal antibodies in multiple myeloma. Clin Lymphoma Myeloma Leuk. 2019;19(10):143–144. doi:10.1016/j.clml.2019.09.239
17. Li K, Barnidge D, Krevvata M, et al. Comparison of the analytical performance of EXENT®, a mass spectrometry-based assessment of M-protein, to SPEP and NGS-based MRD in multiple myeloma patient samples. Blood. 2022;140(Supplement 1):12446–12447. doi:10.1182/blood-2022-160249
18. Derman BA, Stefka AT, Jiang K, et al. Measurable residual disease assessed by mass spectrometry in peripheral blood in multiple myeloma in a Phase II trial of carfilzomib, lenalidomide, dexamethasone and autologous stem cell transplantation. Blood Cancer J. 2021;11(2):19. doi:10.1038/s41408-021-00418-2
19. Or Z, Gandré C, Seppänen AV, et al. France: Health System Summary, 2024. In: WHO Regional Office for Europe on Behalf of the European Observatory on Health Systems and Policies. Copenhagen; 2023.
20. Sullivan SD, Mauskopf JA, Augustovski F, et al. Principles of good practice for budget impact analysis II: report of the ISPOR Task Force on good research practices – budget impact analysis. Value Health. 2014;17(1):5–14. doi:10.1016/j.jval.2013.08.2291
21. Puig N, Contreras Sanfeliciano T, Paiva B, et al. Assessment of treatment response by IFE, next generation flow cytometry and mass spectrometry coupled with liquid chromatography in the GEM2012MENOS65 clinical trial. Blood. 2021;138(Suppl 1):544. doi:10.1182/blood-2021-151557
22. Richardson PG, Jacobus SJ, Weller E, et al. DETERMINATION Investigators. Triplet therapy, transplantation, and maintenance until progression in myeloma. N Engl J Med. 2022;387(2):132–147. doi:10.1056/NEJMoa2204925
23. CIA. The World Factbook. Population of France. Available from: https://www.cia.gov/the-world-factbook/countries/france/.
24. Cancer research UK [Internet]. Survival statistics for myeloma. Available from: https://www.cancerresearchuk.org/about-cancer/myeloma/survival.
25. Hulin C, Orazio S, Monnereau A, et al. P938: survival of patients with multiple myeloma in the general population based on data from two French cancer registries. Hemasphere. 2023;7(Suppl):e306494f. doi:10.1097/01.HS9.0000970656.30649.4f PMCID: PMC10431277.
26. Sécurité sociale, l’Assurance maladie [Internet]. National biology coding table. Available from: http://www.codage.ext.cnamts.fr/cgi/nabm/cgi-fiche?p_code_nabm=1571&p_date_jo_arrete=%25&p_menu=FICHE&p_site=AMELI.
27. Ministère du Travail, de la Santé et des Solidarités. [Internet]. The repository of innovative procedures outside the biology and anatomopathology nomenclature (RIHN). Available from: https://sante.gouv.fr/systeme-de-sante/innovation-et-recherche/rihn.
28. Sécurité sociale, l’Assurance Maladie [Internet]. Common classification of medical procedures (CCAM). Available from: https://www.ameli.fr/accueil-de-la-ccam/trouver-un-acte/fiche-abregee.php?code=FEHB001.
29. Veranex primary research with 3 practicing Spanish hematologists in 2024.
30. Mai EK, Huhn S, Miah K, et al. Implications and prognostic impact of mass spectrometry in patients with newly-diagnosed multiple myeloma. Blood Cancer J. 2023;13:1. doi:10.1038/s41408-022-00772-9
31. Abeykoon JP, Murray DL, Murray I, et al. Implications of detecting serum monoclonal protein by MASS-fix following stem cell transplantation in multiple myeloma. Br J Haematol. 2021;193:380–385. doi:10.1111/bjh.17195
32. Szalat R, Anderson K, Munshi N. Role of minimal residual disease assessment in multiple myeloma. Haematologica. 2024;109(7):2049–2059. doi:10.3324/haematol.2023.284662 PMID: 38328864; PMCID: PMC11215375.
33. International Myeloma Foundation. [Internet]. Bone marrow tests for multiple myeloma. Available from: www.myeloma.org.
34. Puig N, Agulló C, Contreras T, et al. Combined mass spectrometry and next generation flow as early predictors of long-term response in relapsed/refractory myeloma patients treated with CAR-T cells and T-cell engagers. EHA2024. Abstract#EHA–7107.
35. Bladé J, Beksac M, Caers J, et al. Extramedullary disease in multiple myeloma: a systematic literature review. Blood Cancer J. 2022;12(3):45. doi:10.1038/s41408-022-00643-3 PMID: 35314675; PMCID: PMC8938478.
36. Giles HV, Cook MA, Drayson MT, et al. Redefining nonmeasurable multiple myeloma using mass spectrometry. Blood. 2022;139(6):946–950. doi:10.1182/blood.2021013794 PMID: 34871382.
37. Berlanga O, Simion C, Njere F, et al. PB2139: Monitoring oligosecretory multiple myeloma using MALDI-TOF mass spectrometry. Hemasphere. 2023;7(Suppl):e46491ff. doi:10.1097/01.HS9.0000975320.46491.ff PMCID: PMC10429298.
38. Migkou M, Avivi I, Gavriatopoulou M, et al. Clinical characteristics and outcomes of oligosecretory and non-secretory multiple myeloma. Ann Hematol. 2020;99(6):1251–1255. doi:10.1007/s00277-020-03984-w
39. Veranex primary research with 5 practicing European hematologists in 2024.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.