")
Back to Journals » Clinical Ophthalmology » Volume 18
Utilizing PROSE as a Drug Delivery Device for Preservative-Free Cyclosporine 0.05% for the Treatment of Dry Eye Disease: A Pilot Study
Authors Nakhla MN , Patel R , Crowley E, Li Y, Peiris TB, Brocks D
Received 20 July 2024
Accepted for publication 30 October 2024
Published 9 November 2024 Volume 2024:18 Pages 3203—3213
DOI https://doi.org/10.2147/OPTH.S487369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Monica Nabil Nakhla,1 Ria Patel,1 Estelle Crowley,2 Yichen Li,3 Thelge Buddika Peiris,3 Daniel Brocks2
1Tufts University School of Medicine, Boston, MA, USA; 2Department of Ophthalmology, BostonSight, Needham, MA, USA; 3Department of Mathematical Sciences, Worcester Polytechnic Institute, Worcester, MA, USA
Correspondence: Daniel Brocks, Department of Ophthalmology, BostonSight, Needham, MA, USA, Tel +1 781 726 7337, Fax +1 781 726 7310, Email [email protected]
Purpose: To evaluate the tolerability of utilizing Prosthetic Replacement of the Ocular Surface Ecosystem (PROSE) as a drug delivery device for preservative-free cyclosporine 0.05% for the treatment of dry eye disease.
Patients and Methods: Fourteen current daily PROSE wearers were enrolled, with four screen failures and one subject that did not complete the study protocol due to burning and stinging. Nine subjects, 18 eyes completed the study protocol. All participants were instructed to instill one drop of preservative-free cyclosporine 0.05% in the PROSE reservoir and then fill the rest of the reservoir with preservative-free normal saline. After applying the PROSE and wearing for 6 hours, the PROSE was removed, and the protocol was repeated for at least another 4 additional hours of wear. Baseline, 1 week and 1 month symptom and sign data were collected.
Results: At one month, OSDI improved by an average of 3.83 ± 6.87 from baseline (p = 0.07) and there was no statistically significant change in best corrected visual acuity. Without comparing with placebo, there was statistically significant (p < 0.05) improvement in mean per subject and mean per eye corneal fluorescein staining, conjunctival lissamine staining, and conjunctival hyperemia by slit lamp examination at one-month follow-up.
Conclusion: Utilizing PROSE as a drug delivery system for non-preserved cyclosporine 0.05% was well tolerated in regard to both ocular symptoms and ocular surface signs. Results from this pilot study are suggestive of efficacy. The results of this study support progressing this protocol to a larger scale randomized controlled double blinded prospective clinical trial.
Keywords: ocular surface disease, scleral lens, keratoconjunctivitis sicca, corneal staining
Introduction
Prosthetic Replacement of the Ocular Surface Ecosystem (PROSE) (BostonSight, Needham, MA) is an FDA approved highly customized scleral lens treatment indicated for the management of conditions affecting the ocular surface such as keratoconjunctivitis sicca (dry eye disease), ocular graft-versus-host disease (oGVHD), neurotrophic keratitis and Stevens-Johnson syndrome (SJS).1–4 Prior to daily application on the eye, the PROSE is filled with non-preserved normal saline. An appropriately fitting PROSE will vault over the cornea and gently land on the conjunctiva posterior to the limbus. The liquid reservoir that is created between the posterior surface of the PROSE and the anterior surface of the cornea serves many functions including refractive neutralization of anterior corneal irregularities, ocular surface support and mitigation of ocular surface pain.
Though the PROSE reservoir is traditionally filled with non-preserved normal saline, an off-label technique of filling the reservoir with non-preserved topical ophthalmic medications has been described in a limited fashion. Small retrospective cohorts and case reports have reported on the use of non-preserved commercial antibiotics, and non-preserved anti-VEGF agents in the PROSE reservoir.5–11 It is hypothesized that utilizing the PROSE reservoir for drug delivery will increase drug corneal contact time, increase bioavailability and potentially increase efficacy compared to standard on-label application of topical ophthalmic drops.
Preservative-free cyclosporine topical ophthalmic emulsion 0.05% (Restasis, AbbVie, Atlanta, GA) is a commonly utilized pharmaceutical indicated for the treatment of keratoconjunctivitis sicca.12 Approved by the FDA in 2003, ophthalmic cyclosporine 0.05% is a nonsteroidal, immunomodulating ophthalmic emulsion that targets ocular surface inflammation by blocking T-cell activation and the subsequent cascade of inflammatory cytokines.13 The non-preserved nature of this formulation is of importance, as preservatives held for prolonged periods within the PROSE reservoir would risk severe epithelial damage, and are therefore contraindicated. An additional appeal of cyclosporine 0.05% as a drug candidate is the lack of significant local or systemic adverse effects while having the potential to reduce disease progression due to its specific and reversible action on T cells.14 This lower risk profile is in contrast to other topical ophthalmic immunomodulating or immunosuppressant agents, such as topical steroids, which are associated with significant side effects including cataracts, increased intraocular pressure, glaucoma, and infection.
The tolerability, efficacy and safety of topical ophthalmic cyclosporine 0.05% has been well documented when used on-label. In this pilot study, we embark on the first step of an off-label investigation to evaluate using the PROSE reservoir as a drug delivery system for topical cyclosporine 0.05%, with a focus on evaluating tolerability, including corneal toxicity and symptomatic intolerance. We report the first data presented in ophthalmic literature on the tolerability of cyclosporine 0.05% when administered via the PROSE reservoir as the initial step in investigating the potential utility of this treatment modality for dry eye disease.
Material and Methods
Study Design
This prospective observational pilot study investigated the tolerability of preservative-free cyclosporine 0.05% when administered via the PROSE reservoir in patients with dry eye syndrome. Fourteen subjects were enrolled over 14 months and evaluated by the same practitioner at one eye care center. All participants were 18 years of age or older and were already using or willing to transition to buffered preservative-free normal saline (PuriLens, The Lifestyle Company, Inc, Freehold, NJ) as the PROSE reservoir solution. Subjects had to be current, bilateral, daily wearers of PROSE for greater than 6 months with a baseline ocular surface disease index (OSDI) of 13 or greater.15 Utilizing the National Eye Institute (NEI) Grading Scale for corneal fluorescein staining, subjects were required to have baseline corneal fluorescein staining (CFS) of 2 or greater when combining the scores of both eyes.16 Pertinent exclusion criteria included pregnancy or nursing, ocular surgery in the past 12 weeks, or any subject currently using topical ophthalmic glaucoma medications. Current or prior use of topical cyclosporine eye drops in the last 3 months or current use of Lifitegrast 5% ophthalmic solution with use initiated within the last 3 months were as well criteria for exclusion. All PROSE had standard plasma treatment without Hydra-PEG coating.17
At visit 1A, following informed consent, participants were enrolled into two groups: those currently using PuriLens (Group A) and those who were not currently using PuriLens but were willing to transition to it (Group B). After medical history intake, each participant’s symptoms were evaluated with a tolerability questionnaire and OSDI. The novel tolerability questionnaire (exploratory endpoint) was designed to specifically query symptomatic daily experience of PROSE wear at baseline and during the cyclosporine treatment period; evaluating comfort, burning or stinging, and vision quality. A grading system of zero to ten was utilized for each question, with a higher score indicating a subjective response of more comfort, less burning and stinging and better quality vision. Visual acuity (logMAR) with PROSE was measured.18 The automated Keratograph 5M R-Scan (K5MRS), (Oculus, Arlington, WA) was utilized off-label to measure bulbar conjunctival injection with PROSE on the eye and was utilized on-label to measure bulbar conjunctival injection without PROSE on the eye.19,20 Slit lamp examination was completed to ensure the current PROSE fit was acceptable, to assess the ocular surface, to measure conjunctival redness (Efron grading scale), and to document corneal fluorescein and conjunctival lissamine staining using the NEI grading system.21,22 The Efron grading scale for conjunctival redness was modified for this study, with the conjunctiva superior, nasal, inferior and temporal sections being graded separately from zero (no injection) to four (severe injection) and added together for the total reported score (maximum score 16 per eye).23
Subjects in Group A, who were already using Purilens as their habitual daily PROSE reservoir filling solution, were then started on the cyclosporine 0.05% study protocol; they were instructed to instill one drop of cyclosporine 0.05% in the PROSE reservoir and then fill up the rest of the reservoir with Purilens. After applying the PROSE and wearing for 6 hours, the PROSE was removed, and the protocol was repeated; subjects were instructed to flush out any residual fluid in the reservoir and refill with one drop of cyclosporine 0.05% and to fill the remainder of the reservoir with Purilens again and wear for at least another 4 hours.
Subjects in Group B were instructed to discontinue their current habitual daily PROSE reservoir filling solution and were provided Purilens to instead use exclusively in the reservoir for the next two weeks, until they returned for visit 1B. At Visit 1B their medical history was updated, and the same assessments conducted at Visit 1A were completed. At this study visit, Group B subjects were started on cyclosporine 0.05% and given identical instructions for use as Group A. Baseline values of data to be used for comparison post-cyclosporine 0.05% intervention was considered to be Visit 1A for Group A and Visit 1B for Group B.
Participants were re-examined at 1 week (Visit 2) and 4 weeks (Visit 3) post-dispensing cyclosporine 0.05%. Past medical history was updated, and symptoms were re-evaluated via the tolerability questionnaire and OSDI. Visual acuity with PROSE was re-assessed, and K5MRS imaging was repeated. A slit lamp examination was performed to re-assess the ocular surface, conjunctival redness, corneal fluorescein staining and conjunctival lissamine staining. Following the final study visit, all subjects were instructed to discontinue use of cyclosporine 0.05% and to return to their usual pre-study solution regimen.
Statistical Analysis
Statistical analysis was performed using Visual Studio Code (Microsoft Corp., Redmond WA) with python version 3.9.12. Subject data post-treatment was compared to their baseline data, collected prior to initiating use of the study drug. For Group A, the data collected at Visit 1A was considered to be their baseline data pre-intervention. For Group B, the data collected at Visit 1B was considered to be their baseline data (post-initiation of Purilens and pre-initiation of cyclosporine). The core algorithm used was based on the statistical functions module scipy.stats. For univariate data analysis (before/after visits), paired t-test was performed since every patient received treatment. Paired t-test was conducted by scipy.stats. t test_rel and https://www.statskingdom.com/paired-t-test-calculator.html. For bi-variate data, two-way ANOVA (Analysis of variance) was performed. Two-way ANOVA was conducted by sm. stats. anova_lm(model) function. The significance level was set to a P-value of ≤0.05 in all instances of analysis.
Ethical Approval
This study protocol was approved by the New England IRB (NEIRB), an Independent Institutional Review Board, on 7/14/2020, NEIRB File #20201868. All procedures and activities were performed in accordance with relevant state and local law and followed strict ethical obligations as set forth by the Declaration of Helsinki and Good Clinical Practice (GCP). All participants provided informed consent via an IRB approved informed consent document. The clinician completed institutionally required CITI Program training courses including “GCP for Clinical Trials with Investigational Drugs and Medical Devices (US FDA Focus)” and “Biomedical PI”. All aspects of the study were conducted in compliance with the Health Insurance Portability and Accountability Act (HIPAA).
Results
Demographics
Fourteen subjects were enrolled, four of which were screen failures and one of which failed to complete the study due to an adverse event (ocular burning and stinging). Data from eighteen eyes (9 subjects) was collected. All subjects were established daily bilateral PROSE wearers for at least 6 months (mean years of wear 7.01 ± 3.71). Of the 9 subjects that completed all study visits, 4 of the subjects were female and 5 were males. Participants’ age ranged from 38 to 73 years (mean 54.33 +/11.54 years). Six participants identified as Caucasian, one as Asian, and two as Hispanic. All subjects had dry eye disease, and seven of the nine subjects also had corneal ectasia.
OSDI
Over the 1-month intervention period, total OSDI scores decreased (improved) by an average of 3.83 ± 6.87 from baseline (p = 0.07). The maximum improvement in OSDI for one subject over the course of the study was a score decrease of 16.67, while the maximum worsening for one subject was a score increase of 6.24. OSDI Question 11 (“Have your eyes felt uncomfortable in places or areas with low humidity”) was the question that showed the most score improvement during the study period, with a mean decrease of 0.55 ± 0.88 (p = 0.05) from baseline to 1 month. Question 12 (“Have your eyes felt uncomfortable in areas that are air conditioned”) was the only question that showed score worsening over the study period, with a mean increase of 0.22 ± 1.39 (p = 0.32) from baseline to 1 month.
Corneal Staining
Table 1 shows mean NEI corneal fluorescein staining scores at baseline, one week and one-month post initiation of 0.05% cyclosporine treatment. There was a statistically significant improvement (p < 0.05) in corneal staining by subject, by eye and by each individual corneal NEI section at both one week and one month except for the NEI nasal corneal section at one week (p = 0.08). By ANOVA testing, there was no statistically significant different response across the five NEI corneal sections [central, superior, nasal, inferior, temporal] at the one-month time point.
 |
Table 1 Mean Corneal Fluorescein Staining Scores (NEI) at Baseline, 1-Week and 1-Month |
Conjunctival Staining
Table 2 shows mean NEI conjunctival staining scores at baseline, one week and one-month post initiation of 0.05% cyclosporine treatment. There was a statistically significant improvement (p < 0.05) in conjunctival staining by subject, by eye and by each individual conjunctival NEI section at both one week and one month except for the NEI temporal conjunctival section at one week (p = 0.06) and one month (p = 0.19). By ANOVA testing, there was no statistically significant different response across the six NEI conjunctival sections [nasal, supero-nasal, infero-nasal, temporal, supero-temporal, infero-temporal] at the one-month time point.
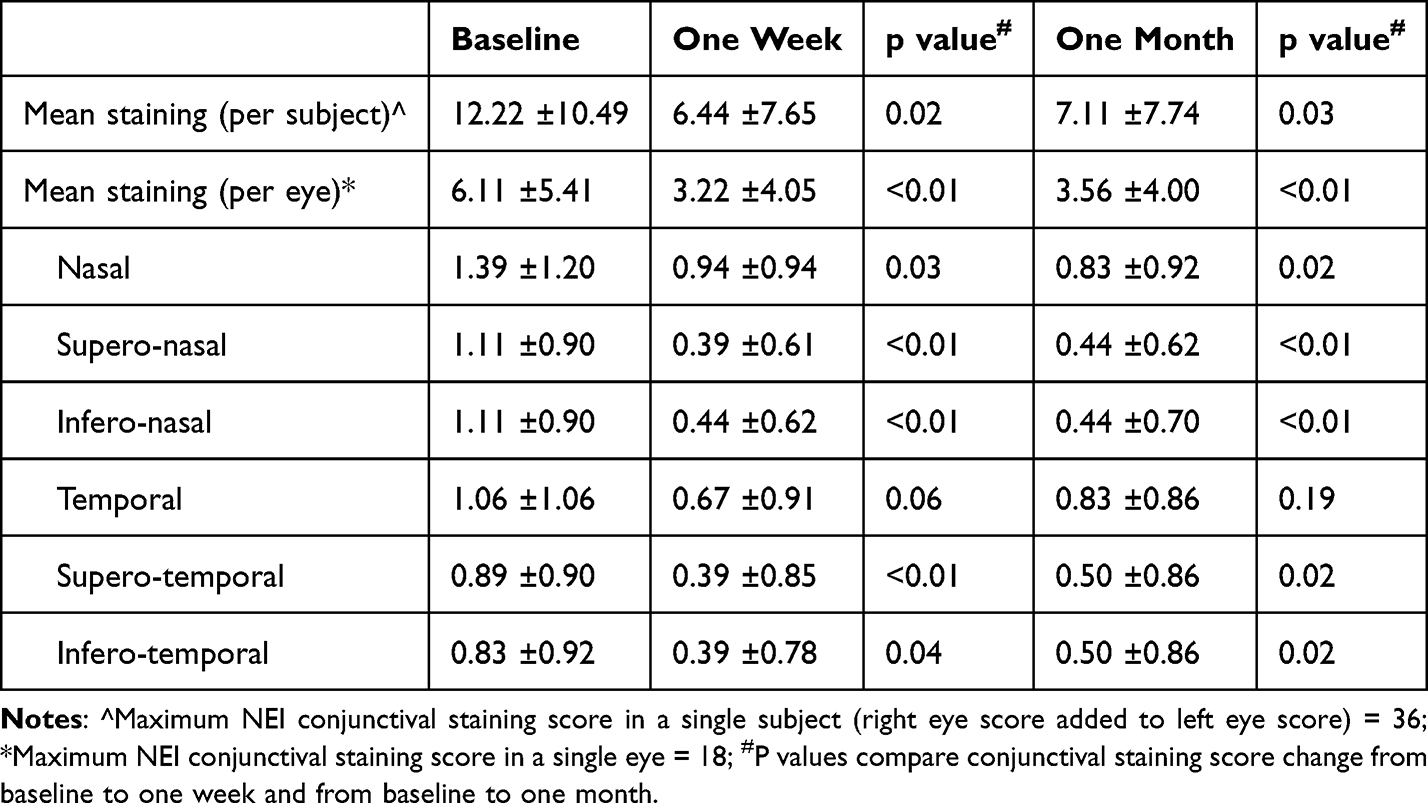 |
Table 2 Mean Conjunctival Staining Scores (NEI) at Baseline, 1-Week and 1-Month |
Vision
There was no statistically significant improvement or worsening in best corrected visual acuity (BCVA) for the eighteen eyes in this study. The mean BCVA (logMAR) at baseline was 0.359 ±0.261. At one week post initiation of 0.05% cyclosporine treatment, the mean logMAR BCVA worsened to 0.393 ±0.320, (p= 0.16). At one month post initiation of 0.05% cyclosporine treatment, the mean logMAR BCVA minimally improved in comparison to baseline, to 0.353 ± 0.320, (p = 0.42).
Conjunctival Redness
Table 3 shows mean conjunctival redness as graded at the slit lamp at baseline (modified Efron grading scale), one week and one-month post initiation of 0.05% cyclosporine treatment. There was a statistically significant improvement (reduction) in average conjunctival redness by subject, by eye and by each individual conjunctival section [superior, nasal, inferior, temporal] at both one week and one month (p < 0.05), except for the superior conjunctival section at one week (p = 0.10).
 |
Table 3 Mean Conjunctival Redness (Modified€ Efron Grading Scale) at Baseline, 1-Week and 1-Month |
Automated Conjunctival Redness
Sixteen of the eighteen study eyes had adequate K5MRS image acquisition for analysis. Image acquisition was not obtained (machine unable to acquire) for several conjunctival sections at several time points for one subject, so this subject was excluded from all K5MRS analysis (both with and without PROSE).
Table 4 shows mean K5MRS grade without PROSE on the eye at baseline, one week and one month post initiation of 0.05% cyclosporine treatment. There was mean improvement in K5MRS grade (conjunctival redness) without PROSE on the eye per subject, per eye and per conjunctival section [bulbar temporal, limbal temporal, limbal nasal, bulbar nasal] at all time points from baseline to one week and from baseline to one month. The mean reduction in redness was only statistically significant (p < 0.05) in the per eye analysis at the one-month time point (p = 0.02).
 |
Table 4 Mean K5MRS Grade at Baseline, 1-Week and 1-Month (Without PROSE on Eye) |
Table 5 shows mean K5MRS grade with PROSE on the eye at baseline, one week and one month post initiation of 0.05% cyclosporine treatment. There was mean improvement in K5MRS grade (conjunctival redness) with PROSE on the eye per subject, per eye and per conjunctival section [bulbar temporal, limbal temporal, limbal nasal, bulbar nasal] at all time points from baseline to one week and from baseline to one month. The mean reduction in redness was only statistically significant (p < 0.05) in the per eye analysis of the limbal nasal conjunctival section at one week (p = 0.03) and at one month (p = 0.03) and the bulbar nasal conjunctival section at one month (p = 0.01).
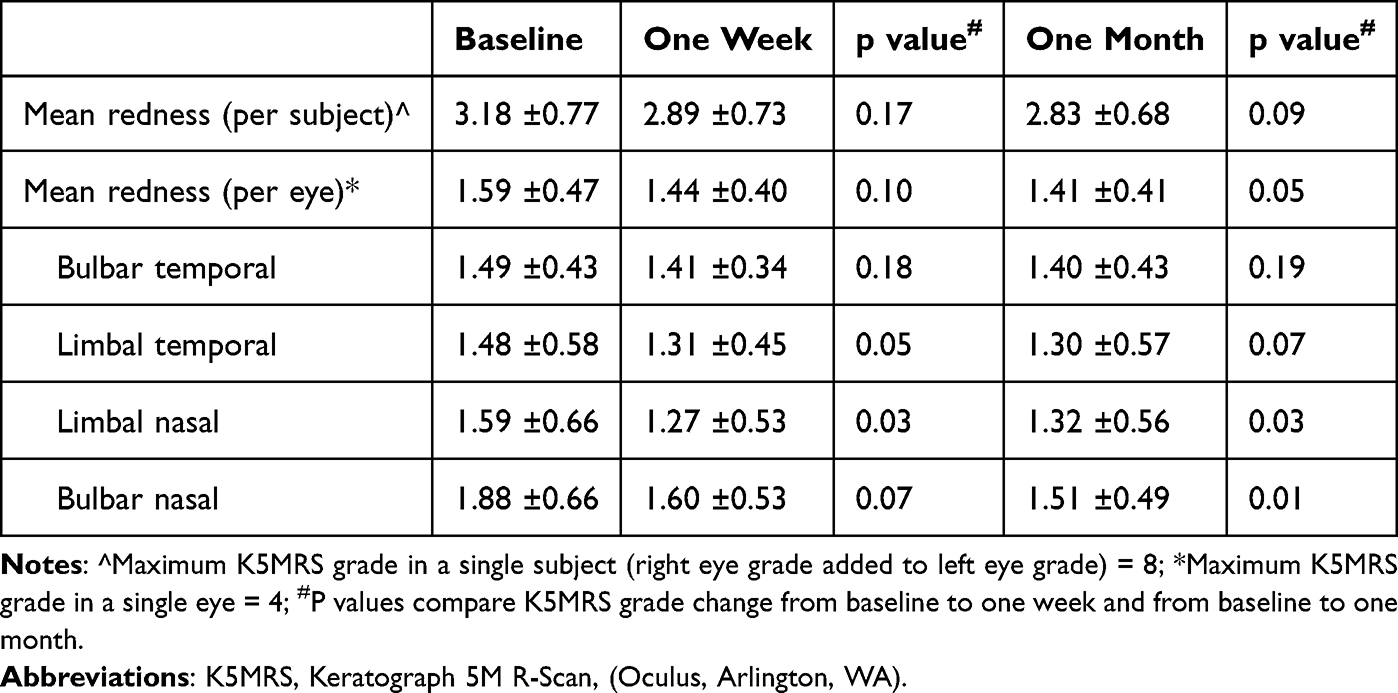 |
Table 5 Mean K5MRS Grade at Baseline, 1-Week and 1-Month (with PROSE on Eye) |
Tolerability Questionnaire
For the nine subjects who completed the study protocol, the mean tolerability scores were statistically equivalent before and after treatment at both the one week and one-month timeline, by mean total score and by individual question scores (Table 6). The “Question 7” mean score result of 9.56 ±0.88 at the 1-month visit indicates the participants on average found the protocol for inserting medication drops into the PROSE reservoir to be easy to perform. Question 7 was not included in the Mean Total Tolerability Score, as it queried ease of use, rather than symptomatic tolerance.
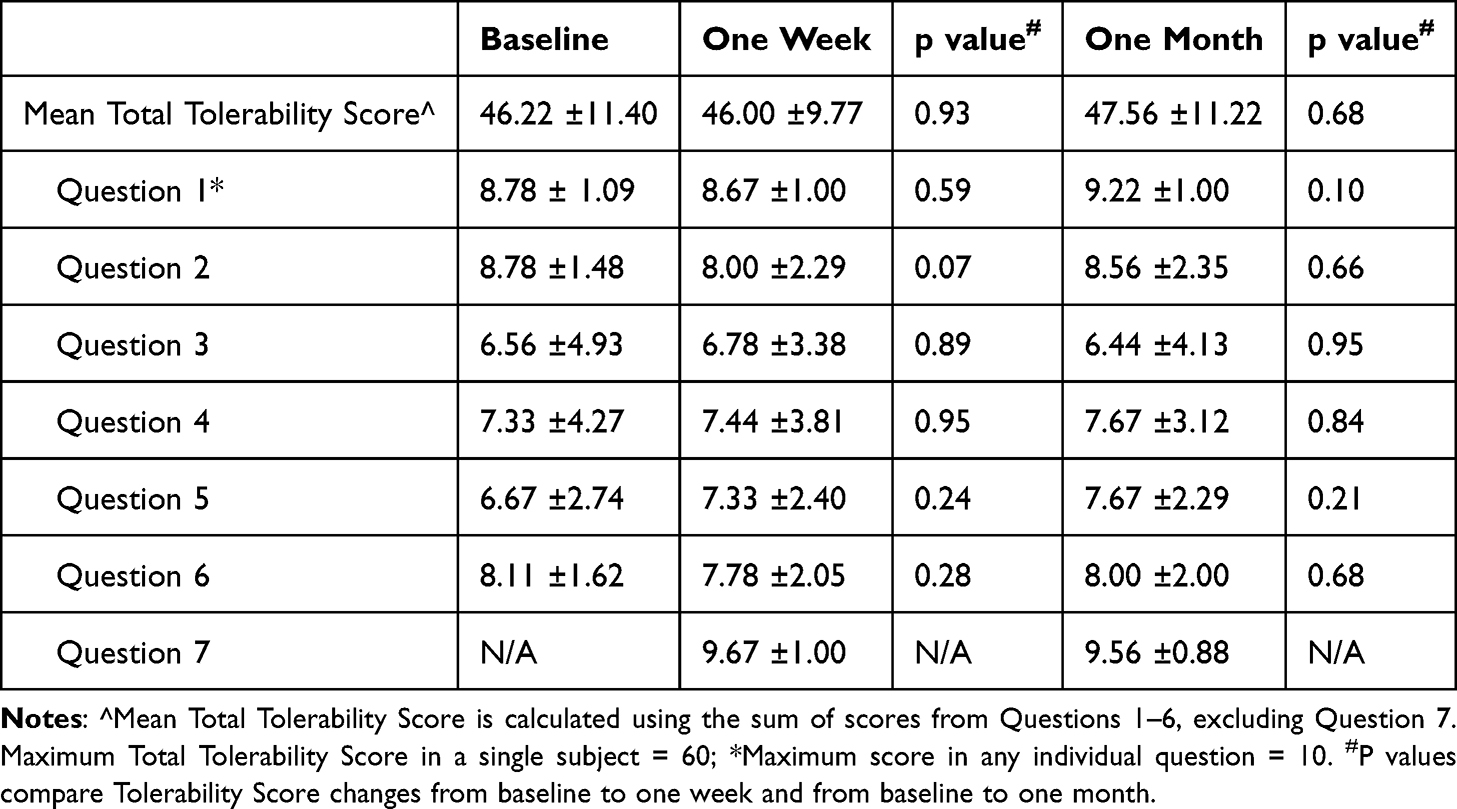 |
Table 6 Mean Tolerability Questionnaire Scores at Baseline, 1-Week and 1-Month |
Adverse Events
One subject (two eyes) reported ocular surface burning and stinging at the one week post-cyclosporine 0.05% initiation visit, and dropped out of the study prior to the final one-month follow-up visit. The entirety of this subject’s data set was removed from the analysis since the participant was unable to complete the study protocol. Ocular surface burning and stinging resolved upon discontinuation of the study drug.
Discussion
On a daily basis, PROSE wearers traditionally fill the fluid reservoir with 0.9% preservative-free saline. Only three options are currently FDA cleared for filling the reservoir: preservative-free normal saline (unbuffered), preservative-free normal saline (pH buffered) and a buffered preservative-free saline solution with added electrolytes, including calcium, magnesium, potassium and phosphate. It is worth noting that any solution instilled in the reservoir must be preservative-free, to avoid ocular surface epithelial damage.
Off-label use of preservative-free ophthalmic pharmaceuticals instilled in a PROSE or scleral lens reservoir has been previously described in literature. Typically, the procedure describes placing one drop of the medication directly in the reservoir, followed by filling the remainder of the reservoir with preservative-free normal saline. Topical non-preserved 0.5% moxifloxacin has been utilized in this manner for bacterial keratitis prophylaxis, specifically in those undergoing PROSE treatment for persistent epithelial defects.5–7 As well, non-preserved 0.5% moxifloxacin has been used in the PROSE reservoir to combat resistant bacterial strains.8 Additionally, topical preservative-free 1% bevacizumab has been utilized in the PROSE reservoir as a treatment for corneal neovascularization and described in two retrospective cohorts.9–11 These prior case reports and retrospective studies have reported this drug delivery model to show efficacy without notable adverse effects or complications.
Overall, minimal experience and literature exists regarding this drug delivery system and to our knowledge, this report is the first to ever describe a prospective clinical trial utilizing a pharmaceutical in this manner. More specifically, no study has previously described results of a prospective clinical trial utilizing preservative-free cyclosporine 0.05% ophthalmic emulsion in a PROSE reservoir for the treatment of dry eye disease. The purpose of this pilot study is to provide an initial evaluation of tolerability of such a potential treatment. Both ocular surface symptoms and ocular surface signs were employed as markers for tracking tolerability during the treatment period. The accrued data is meant to serve as a guide to help evaluate feasibility when considering a future larger randomized placebo controlled double blinded prospective clinical trial.
Tolerability challenges of preservative-free cyclosporine 0.05% ophthalmic emulsion when used on-label and applied directly to the ocular surface have been well documented, including most notably a 17% rate of ocular burning and 1–5% rates of conjunctival hyperemia, eye pain, foreign body sensation, stinging or visual disturbance (such as blurring).12 Cyclosporine 0.05% is a commonly used dry eye pharmaceutical that has been on the market since 2003, with a well-known modest risk profile, and is commercially available with a preservative-free formulation, all of which make it a good candidate for a dry eye study utilizing PROSE as a drug delivery system. Overall, published rates of drug discontinuation related to sides effects of the on-label use of topical cyclosporine 0.05% are quite variable. Sall et al reported 19 of 877 subjects (2.2%) in two multicenter studies of cyclosporine 0.05% used for moderate to severe dry eye discontinued the treatment due to burning and stinging.24 Straub et al reported a retrospective 10-year review of 36 patients, showing a 11.1% rate of drop-out due to local intolerance.13 Anecdotally, in clinical practice, an intolerance drop-out rate is often quoted as being in the range of 10–20%. Published literature underscores that 60% of those that discontinue topical cyclosporine 0.05%, do so due to burning and stinging.14
Using PROSE as a drug delivery device raises notable tolerance questions, namely, whether increased contact time of the drug with the ocular surface, as it remains contained for many hours within the reservoir, will have any ill effects in terms of symptomatology or ocular surface signs. The pilot study results reported here give no suggestion of worsened intolerance or worsened side effect profile when cyclosporine 0.05% is delivered via the PROSE reservoir and worn for at least 10 hours total each day. On the contrary, at one-month post treatment, mean per subject data analysis revealed improvement in OSDI, and mean per subject and mean per eye data analysis revealed improvement in corneal staining, conjunctival staining and conjunctival injection by both slit lamp examination (Efron grading scale) and by automated measurement (K5MRS), though statistical significance of these results varied.
Of note, mean OSDI scores showed improvement with the reduction in overall score approaching statistical significance (p = 0.07). The overall drop-out rate due to burning and stinging was one patient (10%), on par with previously reported cyclosporine drop-out rates due to such intolerance. The Tolerability Questionnaire was created and utilized to have a more focused method of investigating specific questions regarding tolerability of this novel drug delivery therapy in relation to daily PROSE wearing experience. The Tolerability Questionnaire revealed the post-treatment population average to be statistically equal to the pre-treatment population average both by overall questionnaire mean score and by individual question mean score at the one-week and one-month time points. These OSDI and Tolerability Questionnaire results suggest no worsened ocular symptomatology and no appreciable degradation of the subjects’ daily experience with PROSE during the study protocol.
An additional investigative question for this study included determining the difficulty of use of the drug delivery system protocol. Subjects were instructed to apply one drop of cyclosporine 0.05% in the PROSE bowl, followed by filling the rest of the reservoir with preservative-free normal saline. One might imagine the fine motor skills needed to accomplish this task challenging for some subjects. However, the data from Tolerability Questionnaire question 7 (“Please rate on a scale of 0 to 10 the process of application of medication in the device bowl”) revealed an average score of 9.56 ±0.88 out of a possible score of 10 (with 0 indicating “extremely difficult” to do and 10 indicating “extremely easy” to do). This data set supports the practicality of such a drug delivery system for home use.
There are certainly limitations to this pilot study. The small sample size was purposeful, but of course limiting to the overall weight of the study. Additionally, no placebo was utilized in the study design due to lack of access, opting instead to have subjects act as their own controls (using pre-treatment data) in this pilot study. Further understanding of cyclosporine safety and efficacy when delivered within the PROSE reservoir would most certainly necessitate a larger cohort in the form of a randomized placebo controlled double blinded prospective clinical trial. A longer treatment course would as well be beneficial, to more closely approximate typical utilization of cyclosporine 0.05% on-label in clinical practice, where generally at least sixty to ninety days is considered as an adequate timeframe to gauge efficacy. We as well believe conversion of the Tolerability Questionnaire to a validated standardized methodology such as visual analog scale would be appropriate.25
One additional limitation of this drug delivery method includes the fact that tear exchange occurs between the external tear film and reservoir solution throughout the period of PROSE wear time. Though the presence of tear exchange was confirmed on slit lamp examinations at all baseline visits, the rate of such exchange was not measured, as there is no standardized, practical method to do so. Additionally, the composition of the tear film varies not only to some degree physiologically subject to subject, but also according to the varied use of preservative free artificial tears over the PROSE device, which was not restricted or standardized in any way during the study period. Varied tear exchange rates and varied tear composition, which can be affected by artificial tear use, can result in varied solution composition in the PROSE reservoir throughout the PROSE daily wearing periods. Future studies would benefit from quantitatively measuring tear exchange rates and standardization of artificial tear use.26,27
Drug concentration poses a unique challenge and point of discussion in this study and future investigations. Similar to published reports on the use of soft contact lenses for drug delivery, the increased contact time of the drug with the ocular surface is thought to potentially increase bioavailability, to potentially reduce the required frequency of administration, and to potentially decrease the dose concentration required to reach the desired effect.28,29 When choosing to add a pharmaceutical to a PROSE reservoir, there are similar considerations, namely, will the reduced concentration of the created solution (one drop of cyclosporine mixed with normal saline) render the medication less efficacious. Further complicating this question is that the total volume of liquid a PROSE reservoir can hold does vary by customization. Therefore, the final drug concentration of the created mixture is varied. In future investigations, significant attention must be given to calculating drug concentration for each PROSE used by each patient. A large cohort analyzed in this way would likely lead to a determination of optimized concentration to achieve the highest efficacy with the lowest side effect profile. Upon determination of such a concentration, collaborative efforts with the pharmaceutical industry to manufacture standardized concentrations of preservative-free formulations specifically for filling a PROSE or scleral lens reservoir would allow for a more precise, predictable approach for clinical trials and ultimately commercial use.
Conclusion
The ophthalmic and optometric community is in the infancy of investigating the potential use of PROSE or scleral lenses as a drug delivery system for preservative-free ocular topical medications. This pilot study reports encouraging symptom and ocular surface tolerability for cyclosporine 0.05% when delivered via a PROSE reservoir. As well, this early data is suggestive of potential efficacy. Overall, the data analyzed in this report support further investigation into the safety and efficacy of utilizing the PROSE reservoir as a cyclosporine 0.05% drug delivery system for the treatment of dry eye. Additionally, this report underscores the importance of a standardized scientific step-wise approach to the utilization of PROSE or scleral lenses as a drug delivery system.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, DB, upon reasonable request.
Acknowledgments
Authors acknowledge the contributions of Kellen Riccobono, OD, FAAO (Central Texas Eye Center, San Marcos, TX) Bita Asghari, OD, FAAO, FSLS, Chirag Patel, OD, FAAO, Alan Kwok OD, FAAO, FSLS and Karen Carrasquillo, OD, PhD, FAAO, FSLS, FBCLA (BostonSight, Needham, MA) to the creation of the study protocol.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was self-funded by BostonSight. Preservative-free cyclosporine topical ophthalmic emulsion 0.05% (Restasis) was provided at no cost by AbbVie, Atlanta, GA. Preservative-free buffered normal saline (Purilens) was provided at no cost by The Lifestyle Company, Inc, Freehold, NJ.
Disclosure
D. Brocks and E. Crowley are salaried employees of BostonSight, Needham, MA, where BostonSight PROSE treatment was developed and where PROSE devices and BostonSight SCLERAL lenses are manufactured. None of the authors have a proprietary interest in PROSE treatment, the prosthetic devices used in PROSE treatment, or BostonSight SCLERAL lenses. The authors report no other conflicts of interest in this work.
References
1. Asghari B, Brocks D, Carrasquillo KG, Crowley E. OSDI outcomes based on patient demographic and wear patterns in prosthetic replacement of the ocular surface ecosystem. Clin Optom (Auckl). 2022;14:1–12. doi:10.2147/OPTO.S337920
2. Theophanous C, Irvine JA, Parker P, Chiu GB. Use of prosthetic replacement of the ocular surface ecosystem scleral lenses in patients with ocular chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2015;21(12):2180–2184. doi:10.1016/j.bbmt.2015.07.027
3. Wang Y, Rao R, Jacobs DS, Saeed HN. Prosthetic replacement of the ocular surface ecosystem treatment for ocular surface disease in pediatric patients with Stevens-Johnson syndrome. Am J Ophthalmol. 2019;201:1–8. doi:10.1016/j.ajo.2019.01.006
4. Chiu GB, Bach D, Theophanous C, Heur M. Prosthetic replacement of the ocular surface ecosystem (PROSE) scleral lens for Salzmann’s nodular degeneration. Saudi J Ophthalmol. 2014;28(3):203–206. doi:10.1016/j.sjopt.2014.06.001
5. Lim P, Ridges R, Jacobs DS, Rosenthal P. Treatment of persistent corneal epithelial defect with overnight wear of a prosthetic device for the ocular surface. Am J Ophthalmol. 2013;156(6):1095–1101. doi:10.1016/j.ajo.2013.06.006
6. Ciralsky JB, Chapman KO, Rosenblatt MI, et al. Treatment of refractory persistent corneal epithelial defects: a standardized approach using continuous wear PROSE therapy. Ocul Immunol Inflamm. 2015;23(3):219–224. doi:10.3109/09273948.2014.894084
7. Asghari B, Brocks DC. Early postoperative therapeutic scleral lens intervention for penetrating keratoplasty complications in atopic keratoconjunctivitis. Eye Contact Lens. 2023;49(6):254–257. doi:10.1097/ICL.0000000000000997
8. Zhai H, Bispo PJM, Kobashi H, Jacobs DS, Gilmore MS, Ciolino JB. Resolution of fluoroquinolone-resistant Escherichia coli keratitis with a PROSE device for enhanced targeted antibiotic delivery. Am J Ophthalmol Case Rep. 2018;12:73–75. doi:10.1016/j.ajoc.2018.09.006
9. Lim M, Jacobs DS, Rosenthal P, Carrasquillo KG. The Boston ocular surface prosthesis as a novel drug delivery system for bevacizumab. Semin Ophthalmol. 2009;24(3):149–155. doi:10.1080/08820530902802013
10. Keating AM, Jacobs DS. Anti-VEGF treatment of corneal neovascularization. Ocul Surf. 2011;9(4):227–237. doi:10.1016/s1542-0124(11)70035-0
11. Yin J, Jacobs DS. Long-term outcome of using prosthetic replacement of ocular surface ecosystem (PROSE) as a drug delivery system for bevacizumab in the treatment of corneal neovascularization. Ocul Surf. 2019;17(1):134–141. doi:10.1016/j.jtos.2018.11.008
12. Restasis (cyclosporine) ophthalmic label [homepage on the internet]. Irvine: Allergan, Inc; 2012. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/050790s020lbl.pdf.
13. Straub M, Bron AM, Muselier-Mathieu A, Creuzot-Garcher C. Long-term outcome after topical ciclosporin in severe dry eye disease with a 10-year follow-up. Br J Ophthalmol. 2016;100(11):1547–1550. doi:10.1136/bjophthalmol-2015-306930
14. Mah F, Milner M, Yiu S, Donnenfeld E, Conway TM, Hollander DA. PERSIST: physician’s evaluation of Restasis® satisfaction in second trial of topical cyclosporine ophthalmic emulsion 0.05% for dry eye: a retrospective review. Clin Ophthalmol. 2012;6:1971–1976. doi:10.2147/OPTH.S30261
15. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118(5):615–621. doi:10.1001/archopht.118.5.615
16. NEI/Industry grading system [homepage on the internet]. San Francisco: American Academy of Ophthalmology; 2024. Available from: https://www.aao.org/education/image/neiindustry-grading-system.
17. Mickles CV, Harthan JS, Barnett M. Assessment of a novel lens surface treatment for scleral lens wearers with dry eye. Eye Contact Lens. 2021;47(5):308–313. doi:10.1097/ICL.0000000000000754
18. Hazel CA, Elliott DB. The dependency of logMAR visual acuity measurements on chart design and scoring rule. Optom Vis Sci. 2002;79(12):788–792. doi:10.1097/00006324-200212000-00011
19. Wu S, Hong J, Tian L, Cui X, Sun X, Xu J. Assessment of bulbar redness with a newly developed keratograph. Optom Vis Sci. 2015;92(8):892–899. doi:10.1097/OPX.0000000000000643
20. Downie LE, Keller PR, Vingrys AJ. Assessing ocular bulbar redness: a comparison of methods. Ophthalmic Physiol Opt. 2016;36(2):132–139. doi:10.1111/opo.12245
21. Efron N, Morgan PB, Katsara SS. Validation of grading scales for contact lens complications. Ophthalmic Physiol Opt. 2001;21(1):17–29. doi:10.1046/j.1475-1313.1999.00420.x-i1
22. Chun YS, Park IK. Reliability of four clinical grading systems for corneal staining. Am J Ophthalmol. 2014;157(5):1097–1102. doi:10.1016/j.ajo.2014.02.012
23. Efron N. Grading scales for contact lens complications. Ophthalmic Physiol Opt. 1998;18(2):182–186. doi:10.1016/s0275-5408(97)00066-5
24. Sall K, Stevenson OD, Mundorf TK, Reis BL, CsA Phase 3 Study Group. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. Ophthalmology. 2000;107(4):631–639. doi:10.1016/S0161-6420(99)00176-1
25. Amparo F, Schaumberg DA, Dana R. Comparison of two questionnaires for dry eye symptom assessment: the ocular surface disease index and the symptom assessment in dry eye. Ophthalmology. 2015;122(7):1498–1503. doi:10.1016/j.ophtha.2015.02.037
26. Otchere H, Jones LW, Sorbara L. Effect of time on scleral lens settling and change in corneal clearance. Optom Vis Sci. 2017;94(9):908–913. doi:10.1097/OPX.0000000000001111
27. Courey C, Michaud L. Variation of clearance considering viscosity of the solution used in the reservoir and following scleral lens wear over time. Cont Lens Anterior Eye. 2017;40(4):260–266. doi:10.1016/j.clae.2017.03.003
28. Rykowska I, Nowak I, Nowak R. Soft contact lenses as drug delivery systems: a review. Molecules. 2021;26(18):5577. doi:10.3390/molecules26185577
29. Franco P, De Marco I. Contact lenses as ophthalmic drug delivery systems: a review. Polymers. 2021;13(7):11. doi:10.3390/polym13071102
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.