")
Back to Journals » Clinical Ophthalmology » Volume 19
Validation of a Novel Low-Cost Glaucoma Risk Calculator for Community-Based Screening in High-Risk Populations
Authors Grimes K , Madu CT , Carrington C, Laroche D
Received 19 November 2024
Accepted for publication 24 January 2025
Published 3 February 2025 Volume 2025:19 Pages 357—369
DOI https://doi.org/10.2147/OPTH.S500509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kara Grimes,1,* Chisom T Madu,2 Carena Carrington,3 Daniel Laroche4,5,*
1School of Medicine, New York Medical College, Valhalla, NY, USA; 2School of Medicine, City University of New York School of Medicine, New Yorkṭ, NY, USA; 3School of Medicine, SUNY Downstate Health Sciences University, Brooklyn, NY, USA; 4Department of Ophthalmology, New York Eye and Ear Infirmary of Mount Sinai, New York, NY, USA; 5Advanced Eye Care of New York, New York, NY, USA
*These authors contributed equally to this work
Correspondence: Daniel Laroche, Advanced Eye Care of New York, 49 West 127th Street, New York, NY, 10027, USA, Tel +1-212-663-0473, Email [email protected]
Purpose: To assess the validity of a novel, low-cost glaucoma screening calculator in determining glaucoma risk in high-risk New York communities.
Patients and Methods: This prognostic community-based study was conducted in New York City neighborhoods from 2022 to 2024 among participants aged 40 years and older. Glaucoma screenings were held at community gatherings including local fairs, senior citizen homes, places of worship, and in the lobby of medical offices. The screenings were conducted by trained non-physician medical personnel comprised medical students and medical assistants working under physician supervision. Participants’ intraocular pressure (IOP) and central corneal thickness (CCT) were measured in both eyes with a handheld tonometer and pachymeter, respectively. Participants then completed a comprehensive eye exam by an ophthalmologist to confirm glaucoma status. Statistical analysis was completed using MedCalc version 22.023 (MedCalc Software Ltd. Ostend, Belgium) with 95% confidence intervals.
Results: Of the 823 study participants, 716 (mean age 62.9 ± 11.9 years) were eligible to participate and completed the comprehensive follow-up exam. 68% identified as Black, 6.7% identified as Hispanic/Latino, and 52.5% identified as female. The Laroche glaucoma calculator had a sensitivity of 93.5% (CI 89.1– 96.5%), specificity of 91.3% (CI 88.5– 93.6%), positive predictive value of 80.5% (CI 75.7– 84.6%), negative predictive value of 97.3% (CI 95.5– 98.4%) and accuracy of 91.9% (CI 89.6– 93.8%).
Conclusion: The Laroche glaucoma calculator shows high sensitivity, specificity, positive predictive value, negative predictive value, and accuracy using affordable screening methods to determine glaucoma risk.
Keywords: glaucoma risk calculator, affordable glaucoma screening, glaucoma screening tools, community-based glaucoma study, Laroche glaucoma calculator, eye screening
Introduction
Glaucoma is the leading cause of irreversible blindness worldwide and is rapidly rising in the US as the aging population increases.1 The primary risk factors for glaucoma are older age,2 male gender,3 individuals who are Black,3 Hispanic/Latino,4 or Asian,5 those with vascular risk factors including hypertension and diabetes,6 enlarged lens,7 and those with a family history of glaucoma.8 The number of people with glaucoma in the US is expected to increase from 3 million to 6.3 million by 2050, and the aging population worldwide is projected to double to 2.1 billion in the same period of time.5,9,10 Current treatment options available for glaucoma can prevent the progression of the disease but cannot reverse glaucomatous damage. Accordingly, screening and early identification of patients who are at high risk is essential to prevent morbidity and blindness.
The key to decreasing the burden of glaucoma is recognizing the underlying causes of health disparities, including suboptimal allocation of resources prompted by social and economic inequities.11 Due to the slow progression of this disease, many individuals affected by glaucoma are unaware of their diagnosis. By creating efficient and accessible screening methods, those at increased risk for glaucoma can be detected, and vision loss can be prevented. As emphasized by Susanna et al, population-based studies conducted in the US have suggested that over 50% of glaucoma cases remain undiagnosed, highlighting the need for effective screening programs.12 Age-related enlargement of the lens and associated elevation of intraocular pressure can occur silently and insidiously in patients with glaucoma. Despite the 2022 recommendations from the United States Preventive Services Task Force (USPSTF) suggesting that there is insufficient evidence to support glaucoma screening, these findings do not consider the numerous publications reporting the high sensitivity of glaucoma screenings in identifying and treating high-risk individuals, including Black Americans, Hispanics/Latinos, and individuals with decreased access to ophthalmic care.13–17
The Health Resources and Services Administration forecasts a 12% decline in ophthalmologist by 2035 with a 24% increase in demand.18 With predicted shortcomings, it is necessary to consider the cost, accessibility, and efficiency needed to conduct eye examinations when detecting glaucoma as a part of community and medical screening programs. In addressing these factors, the benefits of non-physician led interventions should also be considered. Recent community-based eye health interventions, including the Vision Detroit Project, led by healthcare students under physician supervision have contributed to improved patient education, eye-health knowledge, and access to eye care.19–21 Other studies have detailed the increased use of artificial intelligence in non-physician led interventions with algorithms applied to fundus photos and OCT technology that have been shown to outperform ophthalmologist with non-physician obtaining images.22 However, these technologies used in current screening methods remain higher in cost, creating a gap between resource rich and resource poor areas. The lower cost calculator used in this study fills this gap, reducing the need for more expensive technology as a part of the glaucoma screening.
In this article, we assess the validity of a novel, low-cost calculator in efficiently detecting glaucoma in high-risk New York communities. This calculator fills a critical gap in glaucoma screening because it functions without the need for cup-to-disc ratio or the use of expensive fundus photography, optical coherence tomography (OCT), and visual field (VF) equipment, thus saving the time and money on additional testing for those truly found to be at higher risk with this calculator. The purpose of this study is to validate the use of this calculator as a part of community-based and medical screenings in determining if an individual is low- or high-risk for glaucoma, without the need for a comprehensive ophthalmic examination.
Materials and Methods
This study was approved by the Institutional Review Board of Icahn School of Medicine at Mount Sinai (STUDY-22-01454) and adheres to the Tenets of the Declaration of Helsinki. All participants in this study provided written informed consent.
Study Design
This is a prospective, observational, community-based participatory research study that assessed and evaluated the validity of the Laroche glaucoma calculator in detecting glaucoma and informing the course of follow-up care. This calculator was previously shown to demonstrate statistically significant diagnostic ability in identifying patients with glaucoma in a retrospective study.23
Recruitment Methods
From September 2022 – March 2024, potential participants were identified through flyers shared in-person and on social media. Most participants were recruited in-person at community events hosted by senior housing developments, local organizations, or places of worship and would take place monthly. Participants with upcoming medical appointments were also recruited by study coordinators in-person in the lobby of physician offices. Study coordinators consisted of trained non-physician personnel comprised medical students and medical assistants working under ophthalmologist supervision. Recruitment and screenings took place in New York communities located in South Bronx, Harlem, Southeast Queens, and central Brooklyn.
Inclusion and Exclusion Criteria
Participants were required to be ≥40 years of age to participate in this study. Individuals unable to cooperate or maintain a still position for the duration of the screening were excluded due to interference with obtaining an accurate reading. For individuals <40 years, screening was conducted as a courtesy and data from these participants was not included in our analysis. Individuals who did not complete both the initial screening and the comprehensive ophthalmic examination were excluded from the analysis.
Enrollment
Participants were informed of the study protocol, as well as any potential risks by the medical personnel. The participant was then given the time to ask questions before providing written informed consent. Following consent, the participants completed a short survey about prior health and demographic data (Figure 1).
 |
Figure 1 Prior health and demographic data collected at initial screening. |
Assessment
Prior to the study, non-physician medical personnel completed a training session led by an ophthalmologist to operate the handheld Pachmate 2 pachymeter (DGH Technology) and a Tono-Pen XL applanation tonometer (Medtronic) to measure CCT and IOP, respectively, and how to place topical proparacaine hydrochloride 0.5% eye drop into the eye. Before collecting participant eye measurements, 1 drop(s) of proparacaine hydrochloride 0.5% was administered to each of the participants’ eyes. Once IOP and CCT were collected, the measurements were documented on the glaucoma screening calculator table, along with the participant’s age (Table 1).
 |
Table 1 The Laroche Glaucoma Screening Calculator |
Based on preliminary study findings,23 medical personnel then applied a numerical point value from −3 to +6 corresponding to each of the three risk factors (age, IOP, and CCT), using Table 2. A sum of the point values from the participants age, IOP, and CCT was then calculated to determine the participant’s total glaucoma risk score in each eye. Based on the total score, each eye was either categorized as low risk (with total point(s) ranging from 0 to 5) or high risk (with total points ranging from 6 to 18), as shown in Table 3. All participants were then asked to complete a comprehensive eye examination by a glaucoma specialist (D.L). Carbonless copy paper was used to document the data collected so all participants could receive a copy of their glaucoma risk score at the end of their visit.
 |
Table 2 Age, Intraocular Pressure, and Central Corneal Thickness Risk Factors With Corresponding Numerical Value. Reprinted With Permission From Laroche et al. Reference [19] Copyright 2022, Used Under the Creative Commons Attribution 3.0 License |
 |
Table 3 Determining Glaucoma Risk and Management Reprinted With Permission From Laroche et al. Reference [18] Copyright 2022, Used Under the Creative Commons Attribution 3.0 License |
Ophthalmologist Comprehensive Eye Exam
All study participants were asked to complete a free comprehensive eye exam by a glaucoma specialist (D.L.) within one month of the initial screening. The ophthalmologist was blinded to the participants determined risk category calculated by the Laroche glaucoma calculator. The eye exam was conducted at two medical offices located near screening locations using the gold standard devices to determine the presence of absence of glaucoma or if a patient was a glaucoma suspect. These devices included slit-lamp examination, Goldmann applanation tonometry, ophthalmoscopy, optical coherence tomography (OCT), and Humphrey visual field. Following examination, the clinical judgement of the glaucoma specialist was used to determine if the participant’s diagnosis is glaucoma, glaucoma suspect, or no glaucoma. Patients were diagnosed with glaucoma if they had glaucomatous optic neuropathy, glaucomatous retinal nerve fiber layer loss, or glaucomatous visual field loss. Glaucoma suspects consisted of persons with elevated IOP, larger cup-to-disc ratio, thin corneas, and family history. All patients received counseling on the importance of regular eye exams, lifestyle modification, and if diagnosed with glaucoma initiation of treatment.
Statistical Analysis
All participant data collected from the initial glaucoma screening and the follow-up comprehensive eye exam were de-identified and assigned a random number. Confirmatory factor analysis with a comparative fit index of 0.95, power of 90%, average factor loading of 0.7, significance (α) of 0.05 and expected dropout rate (ndrop) of 20% were used to compute the sample size of n = 171 (ndrop = 214) using the W.N. Arifin Sample Size Calculator (W.N. Arifin Software, Vancouver, British Columbia).24,25 All participants under the age of 40 and those who did not complete the follow-up comprehensive eye exam were excluded from the analysis. Medical personnel transcribed each of the completed questionnaires and calculator findings from paper format to an electronic format. ROC analysis deriving the cut-off point thresholds of 6 shown in Table 2 are further described in the previous study.23
In this cohort, the participant characteristics were described. Sensitivity, specificity, predictive values, likelihood ratios, and accuracy were calculated using MedCalc version 22.023 (MedCalc Software Ltd., Ostend, Belgium) with 95% confidence intervals (CI).26 The sensitivity, specificity and accuracy were calculated using Clopper-Pearson confidence intervals. In our analysis, the comprehensive eye exam (referred to as our gold standard to detect glaucoma) is assumed to be 100% accurate for determining the presence or absence of disease.
Results
Sociodemographic characteristics and questionnaire responses are listed in Table 4.
 |
Table 4 Baseline Characteristics of 716 Participants |
Participant Characteristics
Eight hundred and twenty-three individuals consented to be a part of this study. One hundred and seven participants were excluded from the analytical sample because they did not meet one or more of the following criteria: ≥40 years of age (92/107 participants), were unable to complete the initial screening (2/107 participants), and/or did not complete the follow-up comprehensive eye examination (27/107 participants). The analytic sample included 716 eligible community members (358 female (52.5%), 257 male (35.1%) and 74 (10.1%) unidentified; mean (SD) age of 62 (11.9) years). Of the eligible participants that responded to the questionnaire, 504 (68%) identified as Black and 49 (6.7%) identified as Hispanic/Latino. Additional findings showed that 352 (48%) participants reported having private insurance, 521 (71%) had completed a detailed eye exam at least once in their past, and a majority (79%) did not have a relative with glaucoma or a relative who went blind. Additionally, 87.4% completed a medical exam in the past year and 91% had no past diagnosis of glaucoma.
Laroche Glaucoma Calculator Results
The results yielded from the screening calculator and comprehensive eye exam are summarized in Table 5. Among these 716 participants, 231 (32.3%) were categorized as high risk and 485 (67.7%) were categorized as low risk, as determined by the glaucoma calculator. Using the gold standard comprehensive eye exam, 199 (27.8%) were confirmed to have a diagnosis of glaucoma or to be a glaucoma suspect and 517 (72.2%) were confirmed to have no glaucoma.
 |
Table 5 Glaucoma Status Based on the Laroche Glaucoma Calculator Versus Comprehensive Eye Exam (Gold Standard) |
Of the 716 participants, 45 (6.3%) were false positives indicating that these participants were categorized as high-risk for glaucoma but were determined to have no glaucoma upon comprehensive eye exam. These participants had an average age of 70.7 years, IOP of 14.5 mmHg, and CCT of 502.7 μm, indicating their increased age and/or decreased corneal thickness may have been attributed to their categorization as high-risk. Within this group of false positives, one-third had only one eye categorized as high-risk at the cutoff value of 6. Figure 2 details the percentage of subjects determined to be high-risk by the Laroche glaucoma calculator compared to those determined to have glaucoma or be glaucoma suspects by the gold standard. Those considered false negative consisted of 13 (1.8%) of the 716 participants that were categorized as low-risk and were later determined to have glaucoma or to be considered a glaucoma suspect. The false negative participants had an average age of 59.1 years, IOP of 22.6mmHg, and CCT of 597.3 μm. Their lower age and increased CCT may have been attributed to their categorization as low risk.
 |
Figure 2 Percentage of participants determined to be high risk by the Laroche glaucoma calculator compared to those determined to have glaucoma or be glaucoma suspects by the gold standard. |
The prevalence of glaucoma among participants by selected demographic characteristics and insurance status is shown in Table 6. Increasing age in each 10-year age group correlated with a significant (p < 0.05) increase in likelihood of the Laroche glaucoma calculator categorizing a participant as high risk and the participant having a diagnosis of glaucoma or glaucoma suspect. For example, 79.7% of participants ≥80 years had at least one eye that was calculated as high risk for glaucoma. Of these, 62.5% had a confirmed diagnosis or were considered glaucoma suspects.
 |
Table 6 Prevalence of Glaucoma Among Participants by Selected Demographic Characteristics and Glaucoma Status, Categorized by Laroche Calculator Versus Gold Standard |
Although only 7 participants self-reported being uninsured, this group also had a statistically significant (p < 0.05) difference in being categorized as high-risk and confirmed glaucoma/glaucoma suspect cases in comparison to those with private insurance or Medicare/Medicaid. To note, there was no statistically significant difference in the prevalence of glaucoma when categorizing the participants by sex or by race/ethnicity.
The positive predictive value (PPV) and negative predictive value (NPV) corresponding to a sensitivity of 93.5% and specificity of 91.3% are reported in Table 7. When the prevalence of glaucoma and glaucoma suspects in the study population (27.8%) was used to calculate predictive values, the PPV was 80.5% and the NPV was 97.3%.
 |
Table 7 Validity of the Laroche Glaucoma Calculator as Tested by Sensitivity, Specificity, Likelihood, Predictive Values, and Accuracy |
The average age (standard deviation; SD) of participants determined to be high-risk by the Laroche glaucoma calculator was 70.9 (10.5) years, as shown in Figure 3. The mean CCT (SD) in the high-risk group was lower than that of the low-risk group (513.5 (37.7) μm vs 558.7 (38.3) μm) and the mean IOP in the high-risk group was higher (18.1 (5.8) mmHg) than that of the low-risk group (15.3 (3.8) mmHg).
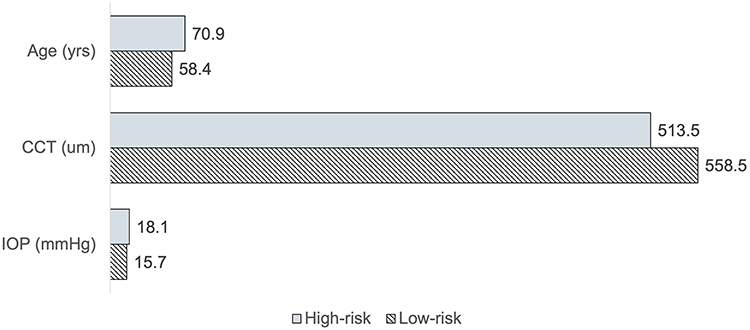 |
Figure 3 Mean of age, central corneal thickness (CCT), and intraocular pressure (IOP) determined by the Laroche glaucoma calculator. |
Clinical Application of the Laroche Glaucoma Risk Calculator
To increase the efficiency of glaucoma screenings, we developed an online version the Laroche glaucoma risk calculator (available free of charge at: https://irp.cdn-website.com/4d783a5d/files/uploaded/Laroche-Glaucoma-Calculator-PDF-KRG-DL-Updated.pdf).
Discussion
The data from this study supports the validity of the Laroche glaucoma calculator as a low-cost tool to determine glaucoma risk and inform the course of follow-up care. The calculator showed high sensitivity (93.5%), specificity (91.3%), and accuracy (91.9%) in detecting glaucoma in high-risk New York populations. This study supported the preliminary findings of the Laroche glaucoma calculator that determined the cut-off values of this tool.23 As a progeny of prior glaucoma calculators, the Laroche glaucoma calculator stands apart in its ability to be utilized both within and outside of clinical settings, requiring only the handheld tonometer and pachymeter for testing. To our knowledge, this is the first glaucoma risk calculator that requires only three variables (age, IOP, and CCT) and can be used by trained non-physician medical personnel.
While several glaucoma risk calculators currently exist, including the widely recognized tool developed by the Ocular Hypertension Treatment Study (OHTS), this novel calculator offers unique advantages. This tool does not require ophthalmoscopy, cup-to-disc ratio assessment, OCT, or VF testing and therefore addresses the current inadequacy of cost-effective glaucoma screening strategies.27 By reducing the reliance on specialized physician expertise and costly equipment for screening, this calculator is a more cost-effective screening tool that enhances accessibility in resource-limited settings. Non-physicians, nurses, technicians, assistants can be trained to conduct the screenings both in office or at locations further away from the office in higher risk communities.
This tool is particularly useful for educating, screening, and identifying individuals at higher risk for glaucoma who can then be referred for more advanced and expensive screening tools to confirm the glaucoma diagnosis. In regions with high-risk populations, such as those with elderly individuals and those of African descent, health policies could support the implementation of this low-cost community-based glaucoma screening approach. Deploying such tools in health centers, churches, and other community venues could facilitate education, early detection of glaucoma, and promotion of general eye health, thereby addressing disparities in eye care and reducing the burden of preventable vision loss. When utilizing this novel calculator and other glaucoma screening tools, it is essential to consider the recommendations from the World Health Organization (WHO), which emphasize that programs for glaucoma detection should only be initiated when adequate services for glaucoma management are available.28 In alignment with these recommendations, this study ensured that glaucoma screenings were conducted in locations with convenient access to comprehensive eye examinations. This approach was intended to minimize barriers to eye care and enhance convenience to the study participants.
Findings from the Laroche glaucoma calculator support predicted demographic changes of those affected by primary open angle glaucoma in the next 25 years. Based on these predictions, Hispanics/Latinos were expected to contribute the highest estimated number of people with glaucoma in the US by 2050.4 In our study, individuals who identified as Hispanic/Latino made up the largest demographic by race/ethnicity to be considered high risk by the Laroche glaucoma calculator (62.7%) and to have a confirmed diagnosis of glaucoma (62.5%) on comprehensive eye exam (Table 6). Contrastingly, although white, non-Hispanic participants had the lowest percentage by racial/ethnic group considered high-risk by the Laroche calculator, this demographic made up the second largest group of confirmed glaucoma cases (25.0% vs 30.0%). Many of those affected by glaucoma are non-Hispanic white Americans, particularly women, due to a high number of this demographic in the aging population.4 Future studies should include a larger participant population.
Given the location of our study in New York communities at high-risk for glaucoma, the results demonstrate a prevalence of 27.8% of glaucoma and glaucoma suspects. Our screening methodology allowed identification of both patients with glaucoma and those glaucoma suspects at risk of developing glaucoma to become educated on this condition and prevent vision loss. Table 6 details the predictive values calculated in this study, detailing the high PPV and NPV at 80.5% and 97.3%, respectively, with an accuracy of 91.9%.
Of the 716 participants, 58 (8.1%) were incorrectly classified by the Laroche glaucoma calculator as either low risk (13 participants) or high risk (45 participants). Participants who were at the extreme ends of one of the three variables (age, IOP, and CCT) may have been misclassified with the current criteria. This included participants over 80 years old, of which 79.7% were considered high risk by the calculator, but only 62.5% were determined to have glaucoma or be glaucoma suspects (Table 6). These are important considerations as the US population continues to age and 17% of the population in the US is over the age of 65. Globally, this decreases to 12% and these individuals have a six-fold greater chance of having glaucoma.29,30 Participants identified as false positive were reassured during their comprehensive ophthalmic examination that factors such as advanced age and thinner corneas likely contributed to their misclassification. Importantly, the proportion of misclassified cases was low, and the slow progression of glaucoma provides an opportunity for patient education and detection of any misclassification during subsequent examinations.
It is also important to consider other non-pathologic causes of extremes of age, IOP, and CCT when evaluating misclassifications. The percentage of individuals with a CCT greater than 600 μm varies depending on the study and population examined. For example, one study identified associations between female sex, increased age, and Black race with thinner corneas.31
A study of 168 eyes from healthy adults aged 19–38 found that 12% of males and 28% of females had corneal thickness measurements below 500 μm.32 Clinically, a CCT less than 500 μm is considered moderately-to-extremely thin, but can be non-pathological in healthy young adults. Conversely, participants in our study who were incorrectly categorized as lower risk (false negative) for glaucoma using the glaucoma calculator may have been misclassified due to their thicker cornea and younger age. Participants identified as false negatives in our study had an average age of 59.1 years and a mean CCT of 597.3 μm, exceeding the average CCT for this age group reported in prior studies.33 The elevated CCT, combined with a relatively lower age, likely contributed to the misclassification of this small subset of participants (1.8%). Nevertheless, raising awareness about the possibility of glaucoma and reinforcing the importance of regular ophthalmic care remain crucial for early detection and management.
There are challenges in identifying glaucomatous damage that may lead to both the underdiagnosis and overdiagnosis of this disease. While one of the purposes of the Laroche glaucoma calculator is to educate and identify undetected cases of glaucoma and glaucoma suspects in the community, it also serves a purpose to recognize individuals as low risk. In doing so, those who are low-risk may defer more expensive glaucoma testing methods and, therefore, the waste of clinical resources and unnecessary medical costs can be reduced, as addressed in the Thessaloniki Eye study.34 The low risk patients will also receive education about the importance of an annual eye examination for general ocular eye health and risk reassessment with increasing age. The small subset of patients identified as false negatives during the initial screening may transition to higher risk categories in subsequent screenings or examinations due to the IOP fluctuations commonly observed in individuals with glaucoma. Additionally, community members identified as high risk may be educated on glaucoma and receive appropriate and adequate, earlier treatment or monitoring as needed. After all, we can prevent glaucoma in those with angle closure with earlier cataract surgery and prevent vision loss with earlier microinvasive glaucoma surgery, which has been shown to preserve visual field in many who go on to develop glaucoma.35
In addition to detecting glaucoma risk, the reported findings from this study may have a psychological impact on participants. Patients with a family risk of glaucoma determined to be low risk by the screening calculator may have a reduced fear of blindness and reduced risk of depression due to fear of developing or having glaucoma. Additionally, those who are low risk can reduce the costs of nonessential further medical testing and reduced side effects of unnecessary treatment. As such, patients determined to be low risk do not require a high level of care by a glaucoma specialist, and the higher level of testing or treatment resources can be used elsewhere.
Future applications of the Laroche glaucoma calculator include adding it to electronic medical record platforms to potentially flag high-risk glaucoma patients and interfusing artificial intelligence (AI) to enhance its effectiveness. Multimodal AI refers to artificial intelligence systems that use multiple data inputs to produce more accurate outputs than unimodal systems. In the future, Multimodal AI can be used to analyze large datasets efficiently while providing real-time data and personalized risk assessments for glaucoma progression to participants. There is also potential use for integration of this risk calculator and AI with telemedicine platforms, to allow for remote monitoring of patients with a family history who may be at low risk and earlier age and may transition to higher risk at a later age or with elevation of intraocular pressure. The low-cost screening method will make future glaucoma screenings more accessible to resource poor communities around the world and create an affordable option for existing general health community clinics.
The primary limitation of this study occurred due to some omitted demographic responses. Nearly 20% of participants omitted responses to the demographic questionnaire, which would have provided more data in better understanding the population being served. This can be addressed in future studies through the creation of an electronic form or by making questionnaire responses mandatory. Additionally, the sample size of this study would benefit from an increased size. To address this limitation, community glaucoma screenings are continuing to take place. As per our study protocol, screening using the Laroche glaucoma calculator identified glaucoma risk in both eyes individually. Contrastingly, during data analysis, we did not distinguish glaucoma status using the gold standard based on either eye. Because of this, we were not able to calculate inter-eye agreement. This can be addressed in future analyses of this study by recording the diagnosis of glaucoma in each eye in the research data.
Conclusion
In summary, this study provided a novel, low-cost screening tool for glaucoma screening both inside and outside of clinical practice. The Laroche glaucoma calculator had high sensitivity, specificity, predictive values and accuracy and was validated in an independent, community population. In using this tool, health care allies can educate and identify patients at risk for glaucoma in the early stages of disease and begin treatment to prevent the progression of irreversible damage. The tool is accessible free online for all providers to implement as a part of detecting glaucoma.
Abbreviations
IOP, intraocular pressure; CCT, central corneal thickness.
Acknowledgments
We would like to acknowledge the National Medical Association Ophthalmology Section and the Pan African Glaucoma Association. The sponsors had no involvement in any stages from study design to submission. The authors would also like to thank Louis R. Pasquale MD and Harriet Lloyd from the Eihorn Clinical Research Center at New York Eye and Ear Infirmary of Mount Sinai for the administrative support. Finally, the authors thank the staff at Advanced Eyecare of New York for their assistance and support.
Author Contributions
All authors made significant contributions to conception, study design, acquisition of data, or analysis and interpretation of data; took part in drafting or writing, or substantially revising or critically reviewing the article; agreed to submit to the current journal; gave final approval of the version to be published; and agree to take responsibility and be accountable for the contents of the article.
Funding
Research grant provided by the Minority Ophthalmology Mentoring program, American Academy of Ophthalmology in partnership with the Association of University Professors of Ophthalmology (AUPO).
Disclosure
Dr Daniel Laroche reports research grants from Alcon, speaker fees from Sight Sciences, non-financial support for equipment for research use from Nidek, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/s2214-109x(17)30393-5
2. Coleman AL, Miglior S. Risk factors for glaucoma onset and progression. Surv Ophthalmol. 2008;53 Suppl1:S3–10. doi:10.1016/j.survophthal.2008.08.006
3. Khachatryan N, Pistilli M, Maguire MG, et al. Primary open-angle African American glaucoma genetics (POAAGG) study: gender and risk of POAG in African Americans. PLoS One. 2019;14(8):e0218804. doi:10.1371/journal.pone.0218804
4. Vajaranant TS, Wu S, Torres M, Varma R. The changing face of primary open-angle glaucoma in the United States: demographic and geographic changes from 2011 to 2050. Am J Ophthalmol. 2012;154(2):303–314.e3. doi:10.1016/j.ajo.2012.02.024
5. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
6. Bonomi L, Marchini G, Marraffa M, Bernardi P. Vascular risk factors for primary open angle glaucoma. Ophthalmology. 2000;107(7):1287–1293
7. Laroche D, Capellan P. The aging lens and glaucoma in persons over 50: why early cataract surgery/refractive lensectomy and microinvasive trabecular bypass can prevent blindness and cure elevated eye pressure. J Natl Med Assoc. 2021;113(4):471–473. doi:10.1016/j.jnma.2021.03.001
8. Le A, Mukesh BN, McCarty CA, Taylor HR. Risk factors associated with the incidence of open-angle glaucoma: the visual impairment project. Invest Ophthalmol Visual Sci. 2003;44(9):3783–3789. doi:10.1167/iovs.03-0077
9. Lage I, Braga F, Almendra M, Meneses F, Teixeira L, Araújo O. Older people living alone: a predictive model of fall risk. Int J Environ Res Public Health. 2023;20(13):6284. doi:10.3390/ijerph20136284
10. Eye Health Data and Statistics. National Eye Institute. Available from: https://www.nei.nih.gov/learn-about-eye-health/eye-health-data-and-statistics.
11. Davuluru SS, Jess AT, Kim JSB, Yoo K, Nguyen V, Identifying XBY. Understanding, and addressing disparities in glaucoma care in the United States. Transl Vis Sci Technol. 2023;12(10):18. doi:10.1167/tvst.12.10.18
12. Susanna R Jr, De Moraes CG, Cioffi GA, Ritch R. Why do people (Still) go blind from glaucoma? Transl Vis Sci Technol. 2015;4(2):1. doi:10.1167/tvst.4.2.1
13. Jin J. Screening for primary open-angle glaucoma. JAMA. 2022;327(20):2030. doi:10.1001/jama.2022.7531
14. Newman-Casey PA, Hark LA, Rhodes LA. It is time to rethink adult glaucoma screening recommendations. J Glaucoma. 2023;32(2):69–71. doi:10.1097/ijg.0000000000002146
15. Girkin CA, Owsley C. Feasibility of glaucoma detection programs for at-risk populations using existing health care infrastructure. J Glaucoma. 2024;33:S5–S8. doi:10.1097/ijg.0000000000002361
16. Hark L, Waisbourd M, Myers JS, et al. Improving access to eye care among persons at high-risk of glaucoma in Philadelphia--design and methodology: the Philadelphia glaucoma detection and treatment project. Ophthalmic Epidemiol. 2016;23(2):122–130. doi:10.3109/09286586.2015.1099683
17. Zhao D, Guallar E, Bowie JV, et al. Improving follow-up and reducing barriers for eye screenings in communities: the stop glaucoma study. Am J Ophthalmol. 2018;188:19–28. doi:10.1016/j.ajo.2018.01.008
18. Berkowitz ST, Finn AP, Parikh R, Kuriyan AE, Patel S. Ophthalmology workforce projections in the United States, 2020 to 2035. Ophthalmology. 2024;131(2):133–139. doi:10.1016/j.ophtha.2023.09.018
19. Goyal A, Richards C, Freedman RL, et al. The Vision Detroit Project: integrated screening and community eye-health education interventions improve eyecare awareness. Ophthal Epidemiol. 2023;30(4):367–375. doi:10.1080/09286586.2022.2127785
20. Ahluwalia A, Morcos D, Koulen P. The impact of having a free community eye clinic located inside a homeless shelter: a retrospective analysis of patient demographics. Front Public Health. 2023;11:1284748. doi:10.3389/fpubh.2023.1284748
21. Devanathan N, Scheive M, Nawash BS, et al. Capabilities and limitations of student-led free vision screening programs in the United States. Transl Vis Sci Technol. 2024;13(1):9. doi:10.1167/tvst.13.1.9
22. Mayro EL, Wang M, Elze T, Pasquale LR. The impact of artificial intelligence in the diagnosis and management of glaucoma. Eye. 2020;34(1):1–11. doi:10.1038/s41433-019-0577-x
23. Laroche D, Rickford K, Mike EV, et al. A novel, low-cost glaucoma calculator to identify glaucoma patients and stratify management. J Ophthalmol. 2022;2022:5288726. doi:10.1155/2022/5288726
24. van Laar S, Braeken J. Understanding the comparative fit index: it’s all about the base! Pract Assess Res Eval. 2021;26(26). doi:10.7275/23663996
25. Kim KH. The relation among fit indexes, power, and sample size in structural equation modeling. Struct Equ Modeling. 2005;12(3):368–390. doi:10.1207/s15328007sem1203_2
26. Diagnostic test evaluation calculator. Available from: https://www.medcalc.org/calc/diagnostic_test.php.
27. Meethal NSK, Sisodia VPS, George R, Khanna RC. Barriers and potential solutions to glaucoma screening in the developing world: a review. J Glaucoma. 2024;33(8S):S33–S38. doi:10.1097/ijg.0000000000002404
28. Thomas R. Glaucoma in developing countries. Ind J Ophthalmol. 2012;60(5):446–450. doi:10.4103/0301-4738.100546
29. Foundation GR. Glaucoma Risks. Glaucoma Research Foundation; 2024.
30. Dyvik EH. Proportion of selected age groups of world population and in regions in 2023. 2024.
31. Wang SY, Melles R, Lin SC. The impact of central corneal thickness on the risk for glaucoma in a large multiethnic population. J Glaucoma. 2014;23(9):606–612. doi:10.1097/ijg.0000000000000088
32. Rashdan H, Shah M, Robertson DM. The frequency of non-pathologically thin corneas in young healthy adults. Clin Ophthalmol. 2019;13:1123–1135. doi:10.2147/opth.S188935
33. Healey PR, Mitchell P, Rochtchina E, Lee AJ, Chia EM, Wang JJ. Central corneal thickness in an older population: the blue mountains eye study. Invest Ophthalmol Visual Sci. 2005;46(13):3520.
34. Founti P, Coleman AL, Wilson MR, et al. Overdiagnosis of open-angle glaucoma in the general population: the Thessaloniki Eye Study. Acta Ophthalmologica. 2018;96(7):e859–e864. doi:10.1111/aos.13758
35. Montesano G, Ometto G, Ahmed IIK, et al. Five-year visual field outcomes of the HORIZON trial. Am J Ophthalmol. 2023;251:143–155. doi:10.1016/j.ajo.2023.02.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.