")
Back to Journals » Clinical Ophthalmology » Volume 18
Visual Outcome and Patient Satisfaction with Implantation of Trifocal Intraocular Lens After Radial Keratotomy
Authors Aljindan M, Neyaz HA , Bin Helayel H , Alwohaibi NN , Rushood AA
Received 31 May 2024
Accepted for publication 26 September 2024
Published 28 October 2024 Volume 2024:18 Pages 3043—3051
DOI https://doi.org/10.2147/OPTH.S471712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mohanna Aljindan,1 Hanan A Neyaz,1,2 Halah Bin Helayel,3 Nada N Alwohaibi,4 Adel Aziz Rushood5
1Department of Ophthalmology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Department of Ophthalmology, Ohud Hospital, Madinah, Saudi Arabia; 3Anterior Segment Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 4Anterior Segment Division, Dhahran Eye Specialist Hospital, Dhahran, Eastern Province, Saudi Arabia; 5Anterior Segment Division, Kahhal Medical Centre, Dammam, Saudi Arabia
Correspondence: Hanan A Neyaz, Imam Abdulrahman bin Faisal University, Ophthalmology Department, Dammam, Saudi Arabia, Tel +966530404999, Email [email protected]
Objective: To investigate the visual outcomes and patient satisfaction following trifocal intraocular lens (IOL) implantation after radial keratotomy (RK).
Methods: This was a retrospective chart review wherein we studied 14 eyes from 7 patients who had undergone cataract surgery and had trifocal intraocular lens (IOL) implanted in the Eastern Province of Saudi Arabia’s King Fahd University Hospital and Kahhal private centre. Data such as demographic characteristics, the time between RK and cataract removal, intraoperative and postoperative complications, preoperative and postoperative uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), and refraction were evaluated. In addition, visual complaints and satisfaction were assessed through a questionnaire.
Results: All eyes included had 8 RK sections. The mean spherical equivalent was +1.81 ± 4.27 D preoperatively and was − 0.41 ± 1.2 D at the last follow-up. The mean uncorrected distance visual acuity (UDVA) increased from 0.32 ± 0.2 prior to surgery to 0.64 ± 0.2 following surgery. The mean efficacy index was 1.01 and a safety index was 1.26. In the last follow-up, 29% reported having 0.5 spherical equivalents, while 86% were within 1D. Improvement in cylindrical correction was noticed in the last follow-up with 36% not more than 0.5 D and 43% within 1D. In total, 80% of patients had a distance-corrected near visual acuity (DCNVA) of better than 20/40. The survey response rate was 100%, and two patients reported a lower degree of satisfaction. Glare and difficulty seeing at night were the most often reported complaints, with a mean of 2.86 ± 1.95 and 22 ± 1.9, respectively.
Conclusion: Our results suggest that implantation of a trifocal IOL is safe and effective in patients with previous RK. However, several factors, including the patient’s preoperative expectations, glare testing, refractive error, number of cuts, optical zone size, and visual phenomena related to RK, should be considered before implantation.
Keywords: cataract surgery, radial keratotomy, trifocal IOL, refractive surgery
Introduction
Radial keratotomy (RK), once a revolutionary refractive surgery technique, was predominantly performed in the 1970s and 1980s to correct myopia and astigmatism until replaced by excimer laser technology in 1990.1 Although no longer common, many patients who underwent RK decades ago are now at an age where cataract development is inevitable, creating a unique and challenging subset of cataract surgery patients.
RK patients present complex challenges during cataract surgery, including corneal instability, difficulty in intraocular lens (IOL) power calculations and diurnal variation.2,3 The weakening of corneal integrity due to previous incisions complicates both the surgical procedure and the prediction of postoperative visual outcome.4
Recent developments in intraocular lens (IOL) technology have demonstrated the possibility of multifocal to treat presbyopia and provide post-cataract surgery spectacle independence in virgin corneas. However, due to concerns regarding visual disturbances like glare, halos, and contrast sensitivity as well as the unpredictability of refractive outcomes their usage in post-RK patients is still under investigation.1,5 Various formulas have been proposed to predict the IOL power in those individuals.6 Despite these challenges, case studies have reported promising results with trifocal IOLs in post-RK patients, showing improvements in uncorrected distance and near vision and high levels of patient satisfaction.1,3,7,8
Given the increasing number of post-RK patients requiring cataract surgery, it is crucial to investigate the effectiveness and safety of trifocal IOL implantation in this population. Therefore, this study aimed to investigate the visual results, patient satisfaction, and quality of vision following cataract surgery with the implantation of a trifocal IOL in patients who had a history of RK. We also discussed the indications, constraints, and potential of this procedure in clinical practice. For those individuals who are desperate to be glasses-free, the findings of this study may help clarify a solution.
Methods
Study Design and Patients
This was a retrospective chart review of patients with a history of RK who had undergone cataract surgery with trifocal IOL implantation between 2017 and 2021 at the Kahhal Private Center and King Fahd University Hospital, Eastern Province, Saudi Arabia. Approval from King Fahd University Hospital’s (KFHU) Research Ethical Committee, of the College of Medicine & College of Applied Medical Sciences of the Imam Abdulrahman Bin Faisal University was acquired prior to the study commencing, and the study was carried out in compliance with the 2013 Helsinki Declaration. Each participant provided written informed consent before beginning the study which is available upon request for the Chief Editor of this journal to evaluate. Data is also available upon request from the corresponding author.
A total of 14 eyes of 7 patients (original, 21 eyes) with minimal 6 months of follow-up were included in this study; 7 eyes of 5 patients were excluded from the analysis due to incomplete data and insufficient follow-up. All patients received an explanation of the surgical risks and benefits before the surgery and provided informed consent. Two experienced surgeons (Adel Rushood and Mohanna Aljindan) performed all operations who used the same surgical method throughout. Patient records were reviewed to collect data on demographics (age and sex), the time between RK and cataract, intraoperative and postoperative complications, slit lamp used to examine anterior segment and RK number, Sellen chart used to assess visual acuity (uncorrected and corrected distance visual acuity [UDVA and CDVA, respectively]), autorefraction, and subjective manifest refraction (D). Keratometry (D) (steep and flat) readings, axial length (mm), anterior chamber depth ACD (mm), and IOL refractive power (D) obtained using IOL Master were also collected.
Surgical Technique and Lens
Eye drops containing phenylephrine (25 mg/mL) and cycloplegic (10 mg/mL) were administered 30 minutes before the surgery. Prior to surgery, topical anesthetic eye drops were used, and the eye was cleaned with 5% povidone-iodine. The same disinfectant (10%) was used to clean the eyelids. Surgeons performed cataract surgery using the standard technique to create a clean cornea with a 2.4-mm keratome. To guarantee that it covers the IOL, a uniform, centered 5-mm diameter capsulorhexis was created. A trifocal IOL was implanted into the capsular bag and rotated to the predetermined correct axis if a toric IOL is used. In all cases, the main wound stroma was hydrated, and no sutures were used.
At the conclusion of the surgery, Intracameral cefuroxime was given, and the patient received constricting agent and antibiotic drops. The ASCRS IOL calculator for eyes with prior RK to calculate IOL power was used,9 and the IOL power closest to emmetropia was selected in all patients. AT LISA tri 839MP or tri toric 939MP (Carl Zeiss Meditec, Germany) was implanted in the capsular bag in all patients. The RK incisions remained intact after the surgery, and the procedures went without any difficulty.
Assessment
Postoperative visual acuity for near, distance, and refraction were measured on day 1 and at the last visit after cataract surgery using Snellen chart that was transferred into logMAR to facilitate data analysis.
The quality of vision questionnaire used in this study was originally developed in English, considering similar surveys published in the literature. It was based on the subjective and intuitive Quality of Vision Questionnaire (QoV), which was developed to assess lifestyle activities and visual quality after cataract surgery.10 To accommodate for other factors impacting patients’ daily lives, a modification was developed.11,12
We used the first eight visual symptoms in the QoV questionnaire and the images in this study to help in explaining the symptoms. The questionnaire contained scores with higher scores representing poorer visual quality. Patients were asked to rate their level of difficulty doing a number of tasks for visual disturbance and lifestyle activity, with a score of 0 being “no difficulty”, 1 being “minimal difficulty”, 2 and 3 being “moderate difficulty”, and 4 and 5 being “severe difficulty”. Patients were asked to rate their dependence on glasses based on how frequently they needed them for different tasks, with 0 being “never”, 1 being “rarely”, 2 being “often”, and 3 being “always”. Lastly, for overall satisfaction, patients were asked to evaluate using a 10-point scale, with 0 indicating least and 10 indicating highest satisfaction.
The questionnaire was translated into Arabic by one author and back into English by another. The writers possessed great language abilities in Arabic and English. An experienced consultant with advanced language skills in both languages double-checked and back-translated the English versions, confirmed the Arabic translation, and fixed any inconsistencies.
The Arabic version of the questionnaire was given to the patient for filing during their last appointment.
Statistical Analysis
The mean (± standard deviation) and median were used to describe continuous variables, whereas frequencies and percentages were used to represent categorical data. Using Spearman correlation test, the relationship between preoperative and postoperative spherical equivalents was assessed. According to the discrepancy between preoperative and postoperative CDVA and UDVA readings, respectively, the effectiveness and safety of the procedure were assessed. Specifically, the postoperative and preoperative CDVA ratios and postoperative UDVA and preoperative CDVA ratios (decimal notation) were calculated. Meanwhile, predictability was assessed using the achieved versus the expected refractive outcomes postoperatively. The STATA for Windows program, version 16, was used to conduct all statistical analyses. Statistical significance was defined as a P value of 0.05.
Results
Visual Outcomes
The mean follow-up was 17.14 ± 12.35 months (median: 11.5 months; range, 6–37 months). Table 1 summarizes the clinicodemographic patient characteristics. All eyes included in this study had 8 RK sections performed between 1985 and 2001. The preoperative spherical equivalent refraction was +1.81 ± 4.27 D (median: +3.5; range, (−5.5, +5.75). Table 2 shows the postoperative monocular visual acuity and refractive outcomes at the last follow-up. Figure 1A illustrates the cumulative UDVA. All eyes (100%) achieved UDVA of 20/80 Snellen or better after the surgery. Figure 1B demonstrates the change in postoperative UDVA in comparison to CDVA. At the last follow-up, 49.6% (7 eyes) had lost one or more lines after surgery. Meanwhile, 7% (1 eye) and 43% (6 eyes) remained the same and gained at least one line postoperatively, respectively. The resulting mean efficacy index of 1.01 shows how UDVA and DCVA changed due to surgery. Before TF implantation, 14% had a spherical equivalent of 0.5 D and 21% within 1.00 D. After implantation of the TF lens, 29% reported having 0.5 spherical equivalents, while 86% were within 1.00 D in the last follow-up, illustrated in Figure 1C. A similar effect was reported in cylindrical correction. Significant improvement in cylindrical correction was noticed postoperatively, with 21% having 0.5 D and 79% with 1.00 D compared to 36% who did not have more than 0.5 D and 43% within 1.00 D, shown in Figure 1D. It should be noted that aberrated eyes after RK are not like regular eyes. No post-operative complications were noted.
 |
Table 1 Summary of Demographic and Biometric Data |
 |
Table 2 Postoperative Monocular and Binocular Visual Acuity and Spherical Equivalent, at Last, Follow Up |
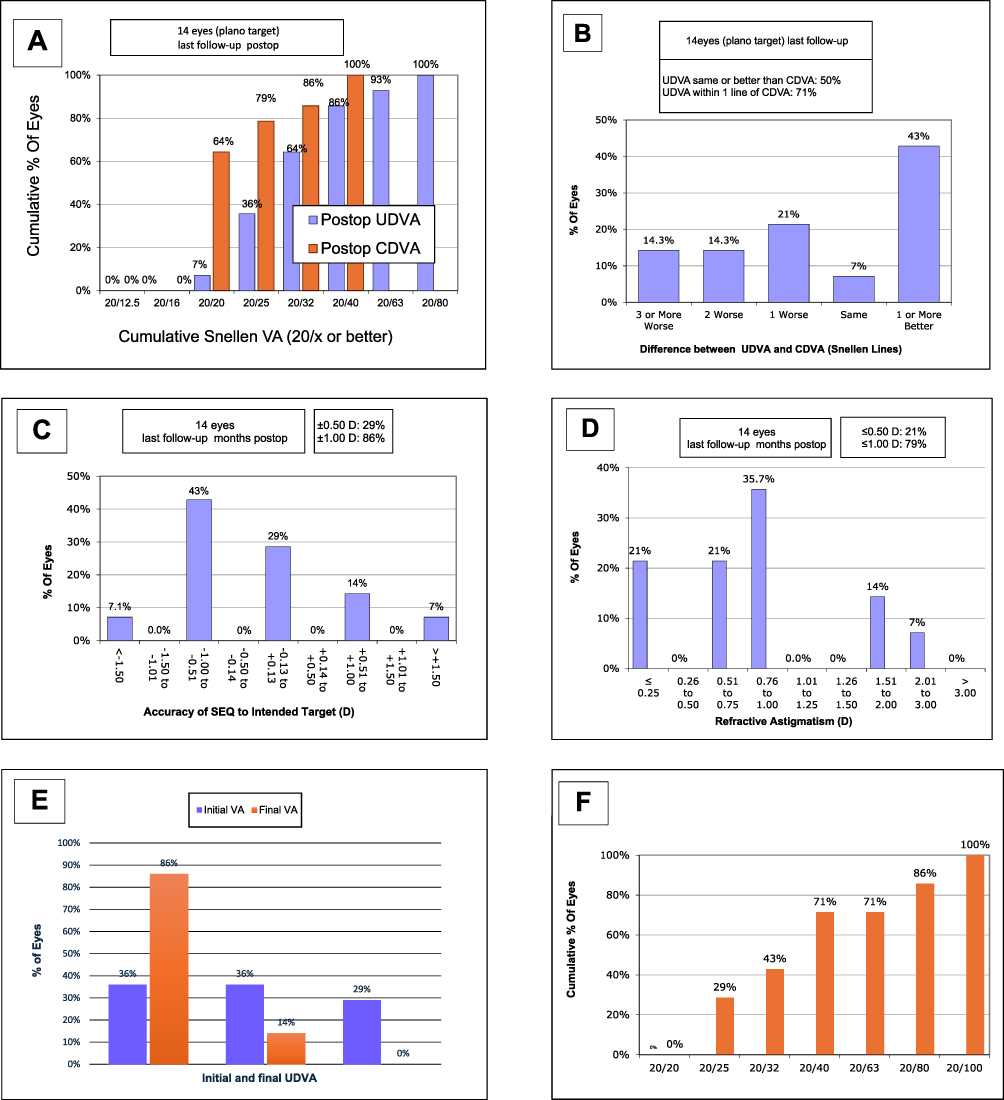 |
Figure 1 (A) Cumulative proportion of eyes with distance corrected visual acuity (CDVA) preoperatively and uncorrected visual acuity (UDVA) values at the last postoperative follow-up. (B) Best-distance-corrected visual acuity (CDVA) at the last follow-up. (C). Postoperative changes in spherical equivalent refraction (SEQ) at last follow-up. (D) Residual cylindrical refractions at the last postoperative follow-up. (E) Initial and final uncorrected distance visual acuity. (F) Cumulative proportion of eyes with best distance-corrected near visual acuity (DCNVA) value at the last postoperative follow-up. |
Figure 1E shows the initial visual acuity for UDVA before implantation of the IOL and the final visual outcome. Figure 1F shows the postoperative changes in distance-corrected near visual acuity (DCNVA) of 14 eyes. At near, 29% of eyes (4) showed a 20/25 Snellen, and 71% of eyes (ten) had a 20/40 Snellen or better cumulative DCNVA.
Quality of Vision
Table 3 shows the patient complaint, and satisfaction with distance, and near vision after implantation of a trifocal IOL. In total, 71.4% of patients scored less than 40 points with a mean score of 29 ± 11.14. Glare and night vision problems were among the most frequently reported complaints. Out of seven patients, two had a low level of satisfaction.
 |
Table 3 Patients Complaints and Satisfaction with Distance, Intermediate, and Near Vision |
Discussion
Various advances in the field and evolving practice patterns have transformed cataract surgery into a modality of refractive surgery. Accordingly, patients can now expect excellent vision without distance aids. With the advent of trifocal IOLs, many patients also desire spectacle independence at near.12 The choices are usually either monovision or presbyopia-correcting IOLs.13 The explantation rate is lower with monovision; however, spectacle independence rates are higher with trifocal IOLs.14 Despite the fact that RK is no longer performed, individuals who had undergone it in the past have developed age-related cataracts. Cataract surgery following RK represents a challenge for surgeons owing to the difficulty in IOL calculation, selection, wound sizing, and location.2,14–16
Patients with RK showed good visual outcomes and acceptable refractive correction after monofocal IOL implantation.2,17 However, patients who have undergone refractive surgery usually desire spectacle independence for near tasks. Despite this, studies investigating visual outcomes of implanting trifocal IOLs in RK patients are lacking. Further investigation of trifocal IOL implants in RK patients is worthwhile.
The current study found no significant change in UDVA at the last postoperative follow-up compared to preoperative CDVA; the efficacy index was 1.01. In addition, the gain in CDVA was more than the loss, with a high safety index of 1.26. These results support that implanting trifocal IOLs after RK is safe and effective for distance vision enhancement and astigmatism correction.
These results differ from those of a prior study in which the authors evaluated the visual and refractive outcomes following cataract surgery and the implantation of multifocal IOLs in 17 eyes that had previously undergone RK. In that study, different multifocal IOLs were implanted, and the patients were followed up for 6 months. At the last follow-up, 29% achieved target refraction.
There were 52.94% of eyes with one line loss of their CDVA, with a safety index of 0.98. The efficacy index was also low at 0.56. However, better results for near visual acuity were obtained, and similar findings were observed in the current study. The authors concluded that although multifocal IOL was safe, it was ineffective for distance vision enhancement.18 However, they used different IOL models in their case series. Conversely, we observed consistently better CDVA in patients in our study. In addition, we used a single model of trifocal IOL. In one of cases reported by Agarwal et al, the patient was implanted with a trifocal toric IOL AT Lisa 939M bilaterally and had already undergone RK and LASIK. The Barrett True K-formula was used for IOL power. Similar to our observation, the patient was happy with his vision but required spectacles for fine distance work and experienced reduced contrast sensitivity.8
We also found three case reports providing evidence for surgical management of cataract and presbyopia in patients with prior RK. Gupta et al reported two cases in which Holladay I and SRK-T formulas were used, and AcrySof IQ ReSTOR multifocal IOL was selected to achieve hybrid monovision with good distance and near vision and spectacle independence.3 There were also two cases reported by Kim et al of refractive lens exchange for RK patients. One patient underwent bilateral multifocal IOL implantation; he had RK in only one eye with long-term use of corrective lenses for monovision. A multifocal IOL in the other patient was implanted in the eye with the worst vision. A high level of satisfaction and acceptable visual outcomes were experienced by both patients. The author used the ASCRS formula and the Oculentis IOL, and no high-order abortion was reported.1
The prospective use of a custom toric multifocal IOL (Soleko FIL611PVT) in a patient with RK, crosslinking, and a subsequent hyperopic shift was also studied by Nuzzi et al. Holladay1 and SRK/T formulae were used. The patient tolerated the IOL well and had good visual acuity (1.0) without refractive regression, after a one-year follow-up.7 Despite the fact that these three case studies used various techniques, they all reported acceptable visual results without drawbacks. In contrast, the majority of the patients in the current study complained of visual phenomena affecting their visual quality despite good UDVA. This may be related to the fact that most patients reported glare preoperatively. These complaints were reported in previous studies in patients with RK.19
In the first three to six months following RK, 50–60% of cases with moderate to severe glare impairment have been documented. After a year, this incidence drops to 0–5%, and after two years, it drops even further.20 After a year following the RK, Neumann further classified the complaints of glare disturbances into “night glare” (30%) and “day glare” (0.7%).19 The degree of visual aberrations after RK has been observed to depend on the extent of a clear optical zone.20 Persistent diurnal fluctuations in refractive error can also result from a varied corneal steepening following RK.20 It should also be considered that patients with RK have weaker corneas, subsequently increasing the risk of refractive regressions and visual acuity fluctuation.2 It might help to explain why fewer than half of the study’s participants had refraction that was within 0.5 diopters of their target refraction.
Another suggestion for this special group of patients is to delay cataract surgery until the cornea has stabilized. Collagen crosslinking may be an alternative to increase corneal refractive stability if the cornea fails to stabilize over time.21 The “trifocal lens effect” caused by the disparity in refractive power between the center and periphery has been seen in RK patients.22,23 Multiple pictures may appear on the retina as a result of power change across the pupil, producing a trifocal effect and pseudoaccommodation. Combining this corneal variability with a trifocal IOL design could degrade retinal images and result in a deterioration of vision.18
Limitations and Recommendations
This was a retrospective study with a small sample size. The nature of the study resulted in recall bias and missing preoperative and postoperative data. In addition, a preoperative visual phenomena questionnaire could not be performed. The lack of patients who underwent more extensive incisional refractive treatments (such as 16-cut RK or additional AK) could have had an impact on the results. Our results may not apply to the entire population of RK patients as they only reflect certain practices. Large sample sizes and comparative monofocal intraocular lenses should be used for subsequent comparative research. Future research should look at the satisfaction,visual,and refractive outcomes of the more recent IOLs, such as extended depth of focus (EDOF), with fewer case reports demonstrating encouraging outcomes24 and accommodative IOLs in patients with RK. Additional testing for contrast sensitivity and glare would also provide additional benefits, eg, IOL designs suitable for each case.
Conclusion
With the good efficacy and safety indices found in this study, trifocal IOL implantation is a viable treatment option for patients with presbyopia and a history of RK following cataract excision. However, the quality of vision is impaired, with patients developing postoperative visual phenomena that may be related to either the RK or the trifocal lens. Thus, if a trifocal IOL is to be implanted, several factors should be considered, including preoperative patient expectation, glare testing, refractive error, number of cuts, and optical zone size.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grants from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Kim K, Seok K, Kim W. Multifocal intraocular lens results in correcting presbyopia in eyes after radial keratotomy. Eye Contact Lens. 2017;43:e22–e25. doi:10.1097/ICL.0000000000000208
2. Alfonso J, Martín-Escuer B, Domínguez-Vicent A, et al. Lensectomy after radial keratotomy: 1-year follow-up. Int Ophthalmol. 2019;39:2561–2568.
3. Gupta I, Oakey Z, Ahmed F, et al. Spectacle Independence after cataract extraction in post-radial keratotomy patients using hybrid monovision with ReSTOR® Multifocal and TECNIS® monofocal intraocular lenses. Case Rep Ophthalmol. 2014;5:157–161. doi:10.1159/000363372
4. Meduri A, Urso M, Signorino GA, Rechichi M, Mazzotta C, Kaufman S. Cataract surgery on post radial keratotomy patients. Int j Ophthal. 2017;10(7):1168–1170. doi:10.18240/ijo.2017.07.23
5. Rosen E, Alio JL, Dick HB, et al. Efficacy and safety of multifocal intraocular lenses following cataract and refractive lens exchange: metaanalysis of peer-reviewed publications. J Cataract Refract Surg. 2016;42:310–328. doi:10.1016/j.jcrs.2016.01.014
6. Turnbull A, Crawford G, Barrett G. Methods for intraocular lens power calculation in cataract surgery after radial keratotomy. Ophthalmology. 127:45–51. doi:10.1016/j.ophtha.2019.08.019
7. Nuzzi R, Monteu F, Tridico F. Implantation of a multifocal toric intraocular lens after radial keratotomy and cross-linking with hyperopia and astigmatism residues: a case report. Case Rep Ophthalmol. 8:440–445. doi:10.1159/000479813
8. Agarwal S, Thornell E. Spectacle Independence in patients with prior radial keratotomy following cataract surgery: a Case Series. Int Med Case Rep J. 2020;13:53–60.
9. Moshirfar M, DeMill DL, Hsu M. Evaluation of the American Society of Cataract and Refractive Surgery intraocular lens calculator for eyes with prior radial keratotomy. Clin Ophthalmo. 5:1243–1247. doi:10.2147/OPTH.S24514
10. McAlinden C, Pesudovs K, Moore J. The development of an instrument to measure quality of vision: the Quality of Vision (QoV) Questionnaire. Invest Ophthalmol Vis Sci. 2010;51:5537–5545. doi:10.1167/iovs.10-5341
11. Gibbons A, Ali T, Waren D, et al. Causes and correction of dissatisfaction after implantation of presbyopia-correcting intraocular lenses. Clin Ophthalmol. 10:1965–1970. doi:10.2147/OPTH.S114890
12. Finkelman Y, Ng J, Barrett G. Patient satisfaction and visual function after pseudophakic monovision. J Cataract Refract Surg. 35:998–1002. doi:10.1016/j.jcrs.2009.01.035
13. Wilkins M, Allan B, Rubin G, et al. Randomized trial of multifocal intraocular lenses versus monovision after bilateral cataract surgery. Ophthalmology. 120:2449–2455.e1. doi:10.1016/j.ophtha.2013.07.048
14. Zhang J, Liu X, Wang J, et al. Outcomes of phacoemulsification using different size of clear corneal incision in eyes with previous radial keratotomy. PLoS One. 2016;11:e0165474. doi:10.1371/journal.pone.0165474
15. Wang J, Liu X, Zhang J, et al. Effects and risks of 3.2-mm transparent corneal incision phacoemulsification for cataract after radial keratotomy. J Int Med Res. 48(3):300060519895679. doi:10.1177/0300060519895679
16. Potvin R, Hill W. New algorithm for post-radial keratotomy intraocular lens power calculations based on rotating Scheimpflug camera data. J Cataract Refract Surg. 39:358–365. doi:10.1016/j.jcrs.2012.09.019
17. Soare C, Patel D, Ionides A. Cataract surgery outcomes in eyes with previous radial keratotomy. Eye (Lond). 36(9):1804–1809. doi:10.1038/s41433-021-01716-6
18. Martín-Escuer B, Alfonso J, Fernández-Vega-Cueto L, et al. Refractive correction with multifocal intraocular lenses after radial keratotomy. Eye (Lond). 33:1000–1007. doi:10.1038/s41433-019-0364-8
19. Neumann AC, Osher RH, Fenzl RE. Radial keratotomy: a comprehensive evaluation. Documenta ophthalmologica. Adv Ophthalmol. 56(3):275–301. doi:10.1007/BF00159078
20. Fan-Paul N, Li J, Miller J, et al. Night vision disturbances after corneal refractive surgery. Surv Ophthalmol. 2002;47:533–546. doi:10.1016/s0039-6257(02)00350-8
21. Elbaz U, Yeung S, Ziai S, et al. Collagen crosslinking after radial keratotomy. Cornea. 33:131–136. doi:10.1097/ICO.0000000000000044
22. Maguire LJ, Bourne WM. A multifocal lens effect as a complication of radial keratotomy. Refract Corneal Surg. 5:394–399.
23. Moreira H, Garbus JJ, Lee M, et al. Multifocal corneal topographic changes after radial keratotomy. Ophthalmic Surg. 23:85–89.
24. Baartman B, Karpuk K, Eichhorn B, et al. Extended depth of focus lens implantation after radial keratotomy. Clin Ophthalmol. 2019;13:1401–1408. doi:10.2147/OPTH.S208550
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.