")
Back to Journals » Journal of Inflammation Research » Volume 17
Vitamin D and Molecules Related to Vitamin D Metabolism in Children with Sepsis
Authors Huang C , Zhang C, Zhang J
Received 30 July 2024
Accepted for publication 29 November 2024
Published 6 December 2024 Volume 2024:17 Pages 10547—10556
DOI https://doi.org/10.2147/JIR.S489233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Caizhi Huang, Cong Zhang, Jie Zhang
Department of Laboratory Medicine, Hunan Children’s Hospital, Changsha, Hunan Province, 410007, People’s Republic of China
Correspondence: Caizhi Huang, Department of Laboratory Medicine, Hunan Children’s Hospital, No. 86 Ziyuan Road, Yuhua District, Changsha, 410007, People’s Republic of China, Tel +86-731-85356927, Email [email protected]
Objective: This study aimed to evaluate the association between vitamin D and molecules related to vitamin D metabolism in children with sepsis.
Methods: A total of 98 hospitalized children with sepsis were included in this study. Blood samples were collected within the first 4 h of admission. Blood vitamin D; molecules related to vitamin D metabolism including vitamin-D-binding protein (VDBP), 7-dehydrocholesterol reductase (DHCR7), 25-hydroxylase (CYP2R1), 24-hydroxylase (CYP24A1), and cathelicidin (CATH); and other inflammatory markers including interleukin-6 (IL-6), procalcitonin (PCT), C-reactive protein (CRP), and white blood cell count (WBC) were measured.
Results: Of the enrolled children, 23.47% (23/98) were confirmed to have severe sepsis, and 10.20% (10/98) died. The prevalence of hypovitaminosis D was 46.94% (46/98) in the children with sepsis. Children with hypovitaminosis D had lower levels of CYP2R1 and CATH and higher levels of CYP24A1, PCT, and IL-6 compared to children with vitamin D sufficiency. Blood vitamin D level was positively correlated with blood VDBP, CYP2R1, and CATH and negatively correlated with CYP24A1, PCT, and IL-6. Blood vitamin D was not independently associated with severe sepsis and mortality, but it was independently associated with the requirement of intensive care unit (ICU) stay.
Conclusion: Molecules related to vitamin D metabolism such as VDBP, CYP2R1, and CYP24A1 are involved in regulating the levels of circulating vitamin D. Children with sepsis had a high prevalence of hypovitaminosis D. Hypovitaminosis D was independently associated with the requirement of ICU stay in children with sepsis.
Keywords: sepsis, vitamin D, vitamin D metabolism, children
Introduction
Vitamin D is a steroid hormone that plays an important role in human health and diseases. Vitamin D is mainly produced in the skin from 7-dehydrocholesterol (7-DHC) via exposure to ultraviolet light. 7-DHC can be converted to vitamin D through a nonenzymatic process, as well as to cholesterol through the enzymatic effect of 7-dehydrocholesterol reductase (DHCR7). Therefore, DHCR7 activity determines the quantity of 7-DHC that would be available for vitamin D production. Vitamin D is biologically inactive and needs to be bound to vitamin-D-binding protein (VDBP), which is the major transport protein for vitamin D and its metabolites.1 Additionally, it requires two sequential hydroxylations to be converted to calcitriol [1, 25-dihydroxy vitamin D (1,25(OH)2D)], the biologically active form. The first hydroxylation of vitamin D occurs in the liver and produces 25-hydroxyvitamin D [25(OH)D]. This is mediated by CYP2R1, which is considered to be the main 25-hydroxylase.2 25(OH)D is the main and the most stable metabolites of vitamin D, which is widely used as a suitable and reliable biomarker to investigate individual vitamin D status and establish vitamin D sufficiency. 25(OH)D can be subsequently transported to the kidneys via VDBP and finally hydroxylated into 1,25(OH)2D by 1α-hydroxylase (CYP27B1). Inactivation and degradation of 25(OH)D and 1, 25(OH)2D are mediated by 24-hydroxylase (CYP24A1), which generates a variety of hydroxylated products that are targeted for excretion through well-established pathways.3
Vitamin D insufficiency and deficiency is an important public health problem among children worldwide. Besides its well-known role in calcium and bone homeostasis, vitamin D also plays a key role in regulating innate and adaptive immunity and is closely associated with various conditions such as inflammatory disease, autoimmune disease, cardiovascular disease, cancer, and metabolic disorders.4–8 The immunomodulation function of vitamin D and its ability to induce cathelicidin (CATH) expression are important factors in the development of sepsis, which is a systemic immune over response of host cells and a major cause of pediatric mortality.9 Although the causal relationship between hypovitaminosis D and sepsis is not yet clear, there is accumulating evidence of the association between 25(OH)D and increased risk of morbidity and mortality in adult patients.10–15 However, the progress of research on vitamin D and outcomes in children with sepsis is limited, and the results are inconsistent.16–18 Moreover, there is a paucity of studies on the relationship between vitamin D, molecules related to vitamin D metabolism, and sepsis in children. Further evidence from the pediatric population is needed to address the issues. Therefore, this investigation was conducted to preliminarily explore the association of vitamin D with molecules related to vitamin D metabolism (VDBP, CYP2R1, DHCR7, CYP24A1, and CATH) in children with sepsis.
Materials and Methods
Study Population
This retrospective, observational study was approved by the Ethics Committee of Hunan Children’s Hospital (HCHLL-2024-285). The protocol conformed to the provisions of the Declaration of Helsinki. Informed consent was obtained from the legal guardians of all children at admission for the collection and use of medical records and residual samples from routine clinical testing for clinical research. Children admitted to the Hunan Children’s Hospital from April 2020 to June 2021 with sepsis were involved in this study. Diagnostic criteria and definitions for sepsis, severe sepsis, and septic shock were in accordance with the International Pediatric Sepsis Consensus Conference.19
Exclusion criteria included missing data of measurements, blood samples not obtained within 4 h of admission, children with malignant tumors, children who received immunomodulatory therapy or vitamin D preparations in the past 4 weeks, and repeated patients during the study period. A total of 175 children with sepsis were initially enrolled, but 77 were excluded based on the exclusion criteria. Finally, 98 of the children were included for this analysis. Among the children included, there were 75 with sepsis and 23 with severe sepsis (including septic shock), 58 with intensive care unit (ICU) stay and 40 without ICU stay, and 88 children survived (survivors) and 10 died (non-survivors). The flowchart of children in the study is shown in Figure 1.
 |
Figure 1 Flow chart of the study. Patients with severe sepsis included those with septic shock (n=18) and without septic shock (n=5). Abbreviations: ICU, intensive care unit; 25(OH)D, 25-hydroxyvitamin D. |
Data Collection
Blood samples were collected within 4 h of admission and centrifuged to separate the serum from whole blood as soon as possible. The human serum samples for 25(OH)D measurement were stored at 4 °C and tested within 24 h. The samples for VDBP, CYP2R1, DHCR7, CYP24A1, and CATH measurement were stored at −70 °C and tested within one week. Serum 25(OH)D level was determined by chemiluminescent immunoassay (ADVIA Centaur XP; Siemens, Erlangen, Germany). Serum VDBP, CYP2R1, DHCR7, CYP24A1, and CATH levels were detected by ELISA (reagent kit from China). The definition of vitamin D levels in Hunan Children’s Hospital included deficiency (< 37.50 nmoL/L), insufficiency (37.5–50.0 nmoL/L), and sufficiency (50.0–250.0 nmoL/L). Hypovitaminosis D was defined as 25(OH)D < 50.0 nmoL/L, including insufficiency and deficiency. Other laboratory parameters including white blood cell count (WBC); C-reactive protein (CRP), procalcitonin (PCT), and interleukin-6 (IL-6) levels; and the rate of positive blood culture were also collected for further analysis. All tests were performed by the Laboratory Medicine Department of Hunan Children’s Hospital.
Statistical Analysis
All data were analyzed using SPSS version 19.0 software (Armonk, NY, United States). Serum biomarkers data were expressed as medians (interquartile ranges) according to the data distribution and compared using the Mann–Whitney U-test. Categorical variables were presented as numbers and percentages (%) and compared using the chi-squared test. The Spearman rank correlation test was applied to analyze relationships between two continuous variables. Binary multivariate logistic regression analysis was performed to further analyze the statistically significant factors determined by univariate analysis. P-values < 0.05 were considered statistically significant.
Results
Patient Characteristics
A total of 98 children were included in this study. Of these, 52 (53.06%) had vitamin D sufficiency, and 46 (46.94%) had hypovitaminosis D, including 33 (33.67%) with vitamin D deficiency and 13 (13.27%) with vitamin D insufficiency. The characteristics of the study population are shown in Table 1. There were no significant differences in sex and laboratory parameters including VDBP, DHCR7, CRP, WBC, and positive blood culture rate between the vitamin D sufficiency and hypovitaminosis D groups. However, children in the hypovitaminosis D group were older and had a higher rate of ICU admission, vasopressors support, mechanical ventilation, and hospital mortality compared with children in the vitamin D sufficiency group (P < 0.05). While blood 25(OH)D, CYP2R1, and CATH levels were significantly lower, blood CYP24A1, PCT, and IL-6 levels were significantly higher in the hypovitaminosis D group than in the vitamin D sufficiency group (P < 0.05).
 |
Table 1 Demographic and Clinical Characteristics Based on Vitamin D Levels |
Relationship Between Vitamin D and Molecules Related to Vitamin D Metabolism and Other Inflammatory Biomarkers in Children with Sepsis
Spearman’s rank correlation test revealed that blood 25(OH)D level was positively correlated with blood VDBP, CYP2R1, and CATH (r = 0.247, P = 0.014; r = 0.283, P = 0.005; r = 0.310, P = 0.002, respectively) and negatively correlated with CYP24A1, PCT, and IL-6 (r = −0.587, P < 0.001; r = −0.388, P < 0.001; r = −0.352, P < 0.001, respectively) in children with sepsis. However, blood 25(OH)D level was not correlated with blood DHCR7 and CRP levels and WBC (P > 0.05) (Figure 2).
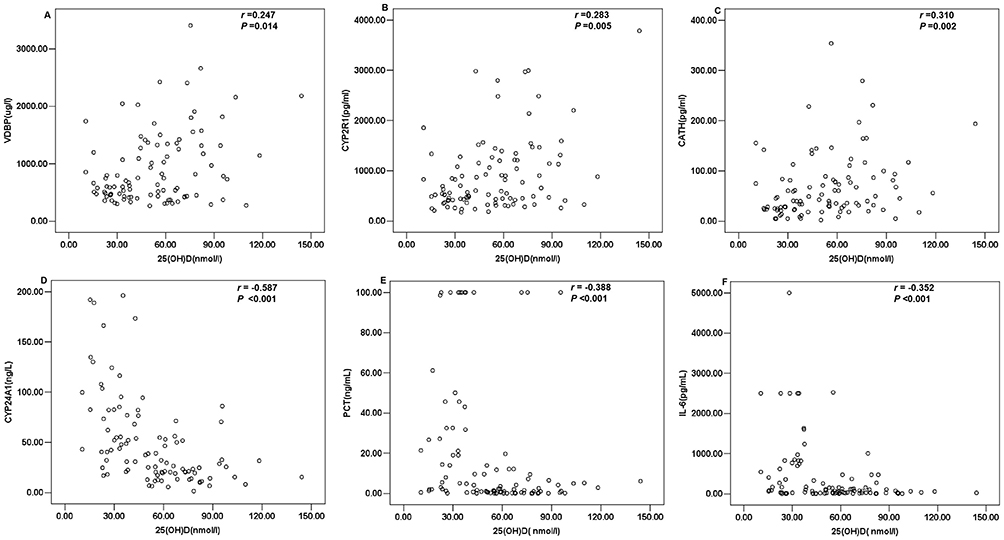 |
Figure 2 Distribution and correlation of vitamin D and molecules related to vitamin D metabolism and other inflammatory biomarkers in children with sepsis. (A–F) Correlation of blood 25(OH)D level with VDBP, CYP2R1, CATH, CYP24A1, PCT, and IL-6. Abbreviations, 25(OH)D, 25-hydroxyvitamin D; VDBP, vitamin-D-binding protein; CYP2R1, 25-hydroxylase; CATH, cathelicidin; CYP24A1, 24-hydroxylase; PCT, procalcitonin; IL-6, interleukin-6. |
Association of Vitamin D, Molecules Related to Vitamin D Metabolism, and Other Inflammatory Biomarkers with Severe Sepsis
Children with severe sepsis had significantly lower 25(OH)D level compared to children with sepsis. The levels of CYP24A1, PCT, and IL-6 were significantly higher in children with severe sepsis than in those with sepsis. However, the levels of VDBP, CYP2R1, DHCR7, CATH, CRP, and WBC did not significantly differ between the two groups (P > 0.05). Although our univariate analysis revealed that patients with severe sepsis had lower 25(OH)D level and higher CYP24A1, PCT, and IL-6 levels, the multivariate logistic regression analysis demonstrated that only IL-6 was independently associated with the development of severe sepsis (Table 2).
 |
Table 2 Vitamin D, Molecules Related to Vitamin D Metabolism, and Other Inflammatory Biomarkers in Children with Sepsis versus Severe Sepsis |
Association of Vitamin D, Molecules Related to Vitamin D Metabolism, and Other Inflammatory Biomarkers with Sepsis Mortality
Of the 98 children with sepsis, 10 died. Blood 25(OH)D level was significantly lower in the non-survivor group than in the survivor group. The patients in the non-survivor group were older and had significantly higher blood levels of PCT and IL-6 compared with the survivor group. However, the levels of VDBP, CYP2R1, DHCR7, CYP24A1, CATH, CRP, and WBC did not significantly differ between the two groups (P > 0.05). Multivariate logistic regression analysis showed that only IL-6 was independently associated with sepsis mortality (Table 3).
 |
Table 3 Vitamin D, Molecules Related to Vitamin D Metabolism, and Other Inflammatory Biomarkers in Survivor versus Non-Survivor Group |
Association of Vitamin D, Molecules Related to Vitamin D Metabolism, and Other Inflammatory Biomarkers with ICU Admission
Of the 98 children with sepsis, 58 had ICU stay. Blood 25(OH)D level was significantly lower in children with ICU stay than in those without ICU stay. The patients with ICU stay had significantly lower WBC and higher blood levels of PCT and IL-6 compared with those without ICU stay. However, the levels of VDBP, CYP2R1, DHCR7, CYP24A1, CATH, and CRP were not significantly different between the two groups (P > 0.05). After adjusting for confounding due to sex, multivariate logistic regression analysis showed that lower 25(OH)D and WBC were independently associated with the requirement of ICU admission (Table 4).
 |
Table 4 Vitamin D, Molecules Related to Vitamin D Metabolism, and Other Inflammatory Biomarkers in Patients with and without ICU Stay |
Discussion
Herein, blood 25(OH)D levels in children with sepsis were determined on admission, along with its correlation with molecules related to vitamin D metabolism and other inflammatory biomarkers involved in the development of sepsis. About half of the children with sepsis had vitamin D insufficiency or deficiency. Children with hypovitaminosis D had lower levels of CYP2R1 and CATH and higher levels of CYP24A1, PCT, and IL-6 compared to children with vitamin D sufficiency. 25(OH)D level was positively correlated with blood VDBP, CYP2R1, and CATH levels and negatively correlated with CYP24A1, PCT, and IL-6 levels in children with sepsis. Although blood 25(OH)D may not predict the development of severe sepsis and mortality, it was independently associated with the requirement of ICU stay in children with sepsis.
Vitamin D status varies in different pediatric populations with sepsis.16–18 In the present study, the prevalence of hypovitaminosis D [(25(OH)D < 50.0 nmoL/L] in children with sepsis was 46.94%, suggesting that determining vitamin D level may be necessary in children hospitalized with sepsis. The variations in hypovitaminosis D prevalence in children with sepsis could be attributed to the differences in diet, climate and geographical locations, sunlight exposure, skin pigmentation, ultraviolet index, detection methods used for vitamin D analysis, cutoff values used for vitamin D insufficiency and deficiency, and the underlying disease conditions and patient cohorts.17,20
Although the immunomodulatory role of vitamin D and the association of vitamin D insufficiency or deficiency with sepsis has been shown across studies, the progress of research on hypovitaminosis D and clinical outcomes in children with sepsis is rather slow compared to adult patients. Whether vitamin D deficiency is the cause or effect of sepsis is still unclear, and the clinical impact of hypovitaminosis D is poorly understood in children with sepsis. Previous published studies have shown controversial results on the association between hypovitaminosis D and adverse outcomes such as prolonged ICU stay, increased mortality, and illness severity.17,18,21,22 Several investigations demonstrated that a low vitamin D level was independently associated with longer PICU length of stay, increased illness severity, higher mortality rates, and increased duration of mechanical ventilation based on the pediatric intensive care unit population.16,22,23 In the present study, children with sepsis diagnosed with hypovitaminosis D had a higher rate of ICU admission, vasopressors support, mechanical ventilation, and hospital mortality compared to children with sufficient vitamin D. Severe sepsis and non-survivor children had lower 25(OH)D levels (both median < 37.50 nmoL/L). However, further multivariate regression analysis showed that vitamin D level was not an independent risk factor for severe sepsis or mortality in line with the findings of previous studies.17,18 And the 10 non-survivors eventually died of multiple organ failure. Interestingly, our study also revealed that low 25(OH)D level was independently associated with the requirement of ICU stay, indicating, to some extent, an association between vitamin D status and severity of sepsis in children. The discrepancies in the results might be because the sample size of the study was not large enough for subgroup analysis, different cutoff values of vitamin D level were selected for analysis, and due to the heterogeneity spectrum of the cohort study population and the underlying disease conditions.
Vitamin D is associated with anti-inflammatory mechanisms, and its deficiency may result in an increased predisposition to infections. When infection occurs, pathogen-associated molecules are recognized by immune cells, which trigger the activation of enzymes involved in the synthesis of active vitamin D, resulting in the production of the biologically active form of vitamin D. Active vitamin D binds to vitamin D receptors and vitamin D response elements and induces the expression of CATH antimicrobial peptide,9 which is a potent mediator of antibacterial and antiviral activity. Moreover, vitamin D stimulates other antimicrobial factors, including reactive oxygen species, nitric oxide synthase, and interleukin-1β, and modulates the innate and adaptive immunity, which alters the inflammatory response and reduces tissue damage. Therefore, a low vitamin D level may indicate susceptibility to infectious diseases and be associated with a positive blood culture.24 In the present study, culture positivity in children with sepsis and hypovitaminosis D was not significantly different from that in children with sepsis and sufficient vitamin D, which was in agreement with another reported study.25 The heterogeneous results might be due to the use of antibiotics in local hospitals before patients are transported to our tertiary hospital. A published randomized controlled trial demonstrated that vitamin D administration resulted in lower IL-6, tumor necrosis factor-α level, cardiovascular sequential organ failure assessment score, and lower incidence of septic shock.26 Another previous study showed a positive association of 25(OH)D and CATH among critically ill patients, and the two mediators were both at low levels.27 In the current study, children with sepsis and hypovitaminosis D had significantly lower CATH level and higher PCT and IL-6 levels. Moreover, 25(OH)D level was positively correlated with CATH and negatively correlated with PCT and IL-6 in children with sepsis. These results are in agreement with the previous studies and suggest that hypovitaminosis D is probably associated with the development of sepsis in children and might play an important role in further modulating the course of the illness.
The circulating level of vitamin D is closely associated with its synthesis, degradation, and transportation.28,29 Therefore, the molecules that take part in vitamin D metabolism also serve as vital components for maintaining vitamin D concentration in the organism.30 VDBP, primarily produced in the liver and expressed in several organs and tissues, has numerous physiological roles, such as transporting vitamin D and its metabolites, regulating bone development, scavenging actin, and regulating the immune and inflammation process.31,32 DHCR7, CYP2R1, and CYP24A1 are not only responsible for regulating the production, activation, and deactivation of vitamin D, respectively, but are also reported to be associated with some conditions.29,30,33 In this study, children with sepsis diagnosed with hypovitaminosis D had significantly lower CYP2R1 and significantly higher CYP24A levels. Additionally, 25(OH)D level was positively correlated with VDBP and CYP2R1 and negatively correlated with CYP24A1. However, multivariate logistic regression analysis showed that these molecules were all not independently associated with severe sepsis, the requirement of ICU stay, and mortality in children with sepsis. The results indicated that the expression of VDBP, CYP2R1, and CYP24A1 regulated the variation of vitamin D concentration and therefore reduced its immunomodulation and anti-inflammation effect, although they may not be directly involved in the pathophysiological process of sepsis. In our study, DHCR7 was not significantly associated with vitamin D level. The detailed reasons remain unknown due to limited understanding of the regulation mechanism of DHCR7. However, this may be partly because the modulating effect was insufficient to affect the circulating level of vitamin D in our study population.2
There are several limitations in this study. First, the sample size of the study population could have been larger for better analysis of the data among the various pediatric subgroups. Second, the findings of this study cannot be generalized because it is a single-center study with participants being children with sepsis. Third, our study is an association study and not a cause-effect research. Fourth, the prevalence of vitamin D insufficiency or deficiency in the overall hospitalized population is unknown, as this study only investigated the prevalence in children diagnosed with sepsis. However, despite these limitations, our study is one of the few studies to evaluate the association of vitamin D and molecules related to vitamin D metabolism with clinical outcomes in children with sepsis and might provide preliminary data in planning future observational and interventional trials in children with sepsis.
Conclusions
Our study revealed that children with sepsis had a high prevalence of hypovitaminosis D. Low vitamin D level was independently associated with the requirement of ICU stay in children with sepsis. The molecules related to vitamin D metabolism, such as VDBP, CYP2R1, and CYP24A1, were involved in regulating the level of circulating vitamin D, thereby reducing its anti-inflammation function in children with sepsis. This study sets the stage for conducting multicenter and large-scale studies to determine whether early intervention is beneficial for children with sepsis who have hypovitaminosis D.
Abbreviations
ICU, intensive care unit; 25(OH)D, 25-hydroxyvitamin D; VDBP, vitamin-D-binding protein; CYP2R1, 25-hydroxylase; DHCR7, 7-dehydrocholesterol reductase; CYP24A1, 24-hydroxylase; CATH, cathelicidin; CRP, C-reactive protein; PCT, procalcitonin; IL-6, interleukin-6; WBC, white blood cell count.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors wish to thank Doctor Liya Mo from the Department of Laboratory Medicine of Hunan Children’s Hospital for her helpful suggestions about this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Scientific Research Project of Hunan Provincial Health Commission in China (grant number 20200017).
Disclosure
All authors declare that they have no conflict of interest regarding the publication of this article.
References
1. Bouillon R, Schuit F, Antonio L, Rastinejad F. Vitamin D binding protein: a historic overview. Front Endocrinol. 2020;10:910. doi:10.3389/fendo.2019.00910
2. Christakos S, Li S, De La Cruz J, Bikle DD. New developments in our understanding of vitamin metabolism, action and treatment. Metabolism. 2019;98:112–120. doi:10.1016/j.metabol.2019.06.010
3. Jones G, Prosser DE, Kaufmann M. Cytochrome P450-mediated metabolism of vitamin D. J Lipid Res. 2014;55(1):13–31. doi:10.1194/jlr.R031534
4. Bouillon R. Vitamin D and cardiovascular disorders. Osteoporos Int. 2019;30(11):2167–2181. doi:10.1007/s00198-019-05098-0
5. Li Y, Ding S. Serum 25-hydroxyvitamin d and the risk of mortality in adult patients with sepsis: a meta-analysis. BMC Infect Dis. 2020;20(1):189. doi:10.1186/s12879-020-4879-1
6. Hahn J, Cook NR, Alexander EK, et al. Vitamin D and marine omega 3 fatty acid supplementation and incident autoimmune disease: VITAL randomized controlled trial. BMJ. 2022;376:e066452. doi:10.1136/bmj-2021-066452
7. Li X, Liu Y, Zheng Y, Wang P, Zhang Y. The effect of vitamin D supplementation on glycemic control in type 2 diabetes patients: a systematic review and meta-analysis. Nutrients. 2018;10(3):375. doi:10.3390/nu10030375
8. Ghaseminejad-Raeini A, Ghaderi A, Sharafi A, et al. Immunomodulatory actions of vitamin D in various immune-related disorders: a comprehensive review. Front Immunol. 2023;14:950465. doi:10.3389/fimmu.2023.950465
9. Gois PHF, Ferreira D, Olenski S, Seguro AC. Vitamin D and infectious diseases: simple bystander or contributing factor? Nutrients. 2017;9(7):651. doi:10.3390/nu9070651
10. Malinverni S, Ochogavia Q, Lecrenier S, et al. Severe vitamin D deficiency in patients admitted to the emergency department with severe sepsis is associated with an increased 90-day mortality. Emerg Med J. 2023;40(1):36–41. doi:10.1136/emermed-2021-211973
11. Asdie RH, Mulya DP, Nainggolan M. Assessment of 28-day survival of patients with sepsis based on vitamin D status: a hospital-based prospective cohort study in Indonesia. Pan Afr Med J. 2023;45:76. doi:10.11604/pamj.2023.45.76.36336
12. Vanichkulbodee A, Romposra M, Inboriboon PC, Trongtrakul K. Effects of vitamin D insufficiency on sepsis severity and risk of hospitalisation in emergency department patients: a cross-sectional study. BMJ Open. 2023;13(1):e064985. doi:10.1136/bmjopen-2022-064985
13. Seok H, Kim J, Choi WS, Park DW. Effects of vitamin D deficiency on sepsis. Nutrients. 2023;15(20):4309. doi:10.3390/nu15204309
14. Yang X, Ru J, Li Z, Jiang X, Fan C. Lower vitamin D levels and VDR FokI variants are associated with susceptibility to sepsis: a hospital-based case-control study. Biomarkers. 2022;27(2):188–195. doi:10.1080/1354750X.2021.2024598
15. Tosoni A, Cossari A, Paratore M, et al.; on Behalf Of The Internal Medicine Sepsis Study Group. Delta-procalcitonin and vitamin D can predict mortality of internal medicine patients with microbiological identified sepsis. Medicina. 2021;57(4):331. doi:10.3390/medicina57040331
16. He M, Cao T, Wang J, Wang C, Wang Z, Abdelrahim MEA. Vitamin D deficiency relation to sepsis, paediatric risk of mortality III score, need for ventilation support, length of hospital stay, and duration of mechanical ventilation in critically ill children: a meta-analysis. Int J Clin Pract. 2021;75(4):e13908. doi:10.1111/ijcp.13908
17. Kubsad P, Ravikiran SR, Bhat KG, et al. Hypovitaminosis D and parathyroid hormone response in critically Ill Children with sepsis: a case-control study. Indian J Crit Care Med. 2021;25(8):923–927. doi:10.5005/jp-journals-10071-23913
18. Mkk DS, Biswal N, Parameswaran N, Nanda N, Nanda N. Vitamin D status at admission and its association with mortality in children admitted to the pediatric intensive care Unit. Cureus. 2020;12(6):e8413. doi:10.7759/cureus.8413
19. Goldstein B, Giroir B, Randolph A; International Consensus Conference on Pediatric Sepsis. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6(1):2–8. doi:10.1097/01.PCC.0000149131.72248.E6
20. Padur Sivaraman R. Vitamin D deficiency in critically Ill children with sepsis: what is the road ahead? Indian J Crit Care Med. 2021;25(8):843–844. doi:10.5005/jp-journals-10071-23952
21. Xiao D, Zhang X, Ying J, et al. Association between vitamin D status and sepsis in children: a meta-analysis of observational studies. Clin Nutr. 2020;39(6):1735–1741. doi:10.1016/j.clnu.2019.08.010
22. McNally JD, Menon K, Chakraborty P, et al.; Canadian Critical Care Trials Group. The association of vitamin D status with pediatric critical illness. Pediatrics. 2012;130(3):429–436. doi:10.1542/peds.2011-3059
23. Cariolou M, Cupp MA, Evangelou E, Tzoulaki I, Berlanga-Taylor AJ. Importance of vitamin D in acute and critically ill children with subgroup analyses of sepsis and respiratory tract infections: a systematic review and meta-analysis. BMJ Open. 2019;9(5):e027666. doi:10.1136/bmjopen-2018-027666
24. Onwuneme C, Carroll A, Doherty D, et al. Inadequate vitamin D levels are associated with culture positive sepsis and poor outcomes in paediatric intensive care. Acta Paediatr. 2015;104(10):e433–438. doi:10.1111/apa.13090
25. Yaghoobi MH, Taher A, Seifrabie MA, Sabahi M, Rahimi-Bashar F. Serum vitamin D level was not associated with severity of ventilator associated pneumonia. Rom J Intern Med. 2019;57(1):55–60. doi:10.2478/rjim-2018-0033
26. Wang Y, Yang Z, Gao L, Cao Z, Wang Q. Effects of a single dose of vitamin D in septic children: a randomized, double-blinded, controlled trial. J Int Med Res. 2020;48(6):300060520926890. doi:10.1177/0300060520926890
27. Equils O, Naiki Y, Shapiro AM, et al. 1,25-Dihydroxyvitamin D inhibits lipopolysaccharide- induced immune activation in human endothelial cells. Clin Exp Immunol. 2006;143(1):58–64. doi:10.1111/j.1365-2249.2005.02961.x
28. George B, Amjesh R, Paul AM, Santhoshkumar TR, Pillai MR, Kumar R. Evidence of a dysregulated vitamin D endocrine system in SARS-CoV-2 infected patient’s lung cells. Sci Rep. 2021;11(1):8570. doi:10.1038/s41598-021-87703-z
29. Pereira F, Fernández-Barral A, Larriba MJ, Barbáchano A, González-Sancho JM. From molecular basis to clinical insights: a challenging future for the vitamin D endocrine system in colorectal cancer. FEBS J. 2024;291(12):2485–2518. doi:10.1111/febs.16955
30. Linowiecka K, Wolnicka-Głubisz A, Brożyna AA. Vitamin D endocrine system in breast cancer. Acta Biochim Pol. 2021;68(4):489–497. doi:10.18388/abp.2020_5961
31. Huang CZ, Zhang J, Zhang L, Yu CH, Mo Y, Mo LY. Serum vitamin D and vitamin-D-binding protein levels in children with chronic hepatitis B. World J Gastroenterol. 2021;27(3):255–266. doi:10.3748/wjg.v27.i3.255
32. Lisowska-Myjak B, Jóźwiak-Kisielewska A, Łukaszkiewicz J, Skarżyńska E. Vitamin D-binding protein as a biomarker to confirm specific clinical diagnoses. Expert Rev Mol Diagn. 2020;20:49–56. doi:10.1080/14737159.2020.1699064
33. Chen XQ, Mao JY, Wang CS, et al. CYP24A1 involvement in inflammatory factor regulation occurs via the wnt signaling pathway. Curr Med Sci. 2022;42(5):1022–1032. doi:10.1007/s11596-022-2564-x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.