")
Back to Journals » Journal of Inflammation Research » Volume 17
Xuanbi Yuyang Decoction Ameliorates DSS-Induced Colitis by Inhibiting Pyroptosis via Blocking of IL-17 Pathway Activation
Authors Huang X, Li L, Zheng C, Li J, Chen G, Chen Y
Received 22 May 2024
Accepted for publication 11 July 2024
Published 5 August 2024 Volume 2024:17 Pages 5235—5249
DOI https://doi.org/10.2147/JIR.S472812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xiaoyan Huang,* Liqun Li,* Chaowei Zheng, Jianfeng Li, Guangwen Chen, Yalu Chen
Department of Gastroenterology, The First Affiliated Hospital of Guangxi University of Chinese Medicine, Nanning City, Guangxi Zhuang Autonomous Region, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyan Huang, Department of Gastroenterology, The First Affiliated Hospital of Guangxi University of Chinese Medicine, 89-9 Dongge Road, Qingxiu District, Nanning City, Guangxi Zhuang Autonomous Region, 530023, People’s Republic of China, Tel +00867715667460, Email [email protected]
Background: Ulcerative colitis (UC), a highly relapsing non-specific disease, is difficult to cure completely. The investigation aims to determine the protective effect and potential action mechanism of Xuanbi yuyang decoction (XBD) on UC.
Methods: The chemical composition of XBD was determined through non-targeted metabolomics analysis. Subsequently, experimental mice were orally given 3% DSS for 6 days, followed by XBD treatment (0.3 mL, 0.4 mL). In vitro, the human colon epithelial cells were co-treated with DSS and medicated serum. The therapeutic effects of XBD on UC were evaluated in vivo and vitro. The mechanisms of XBD against UC were determined by detecting hallmarks related to pyroptosis and Interleukin (IL)-17 pathways using Western blot and ELISA. The recombinant human interleukin 17A (rhIL17A) and was applied for further verifying the effect of XBD on IL-17 pathway in UC cells.
Results: XBD supplementation restored DSS-induced weight loss, colon shortening and tissue damage, and reduced DAI. Moreover, XBD enhanced viability, repaired the intestinal mucosal barrier of colitis, decreased pro-inflammatory cytokines levels, and inhibited pyroptosis. Additionally, DSS increased the expression of IL-17 pathway was and cytokines (IL-17A, IL-6), which were blocked by XBD treatment. The rhIL17A treatment attenuated protective effect against DSS-induced colitis and could also enhance pyroptosis.
Conclusion: XBD has a favorable protective effect against DSS-induced colitis through restraining pyroptosis via inhibition of IL-17 signaling pathway activation, suggesting XBD may be a new and effective treatment therapy for UC.
Keywords: ulcerative colitis, Xuanbi yuyang decoction, pyroptosis, IL-17 pathway, inflammation
Introduction
Ulcerative colitis (UC), one of the two major forms of inflammatory bowel disease (IBD),1 is a chronic nonspecific disease leading to intestinal epithelial cell erosion and inflammatory invasion with diarrhea, bloody stool, and weight loss as the main clinical symptoms.2 There is an increase in the prevalence and incidence of UC worldwide, and individuals with colitis are more likely to develop colorectal cancer, which is the most deadly and devastating consequence of UC.3 At present, the clinical drugs for UC mainly include biologics, corticosteroids, immunomodulators, while these treatments are often accompanied with side effects such as dizziness and nausea.4,5 Moreover, the exact pathogenesis of UC is still unclear, and it is widely accepted including immune dysregulation, changes in intestinal microbiota, genetic background, and environmental factors.6,7 Therefore, there is an urgent need to understand the complex pathogenesis against UC, and find novel drugs with slighter side effects and higher efficacy to enrich the current treatment options.
Extensive evidence has highlighted multiple Chinese herbal medicines exhibit antioxidant, anti-inflammatory, immunomodulatory and other active pharmacological effects.8–10 Besides, they also show significant recovery effects in the treatment of UC, as reflected by reducing colon damage, reducing disease activity index (DAI), and regulating mucosal immunity.11,12 For instance, Polygonum multiflorum has become the ingredient of several prescriptions owing to its extensive pharmacological action like anti-inflammatory effects.13,14 Therein, emodin, the main active components in Polygonum multiflorum, can reduce inflammatory cell infiltration, and also have certain therapeutic effects on experimental colitis in mice.15,16 Similarly, other Chinese herbal medicines such as Poria cocos, Rhizoma alismatis, Herba Patriniae, also display good anti-inflammatory effects.17–19 Xuanbi Yuyang decoction (XBD) was extracted from more than 10 kinds of Chinese herbal medicines, including the above-mentioned herbs. However, the therapeutic effect and potential mechanisms of action of XBD on UC remains unclear.
Pyroptosis, referring to an inflammatory cell death form attributes to the cleavage of Gasdermin D (GSDMD) by caspase-1 that is accompanied with the release of inflammatory cytokines and eventually leading to severe inflammatory illnesses.20 The occurrence of UC is usually linked to pyroptosis and the release of inflammatory factors.21,22 Moreover, the interleukin (IL)-17 is a pivotal cytokine in the Th17 immune response, exhibit synergizing or enhancing the effects of many other inflammatory mediators.23,24 Many studies have confirmed that IL-17-related proteins and cytokines play an important function in the development of multiple inflammatory diseases, such as rheumatoid arthritis and psoriasis.25–27 Furthermore, in UC and Crohn’s disease, the expressions of IL-17 family members are increased.28 Additionally, IL-17 can induce pyroptosis of intestinal stem cells and enterocytes, which may further contribute to the progression of IBD.29 However, whether XBD affects the progression of UC by regulating pyroptosis via the IL-17 signaling pathway remains poorly elaborated.
Currently, the protective properties of XBD and its related action mechanisms in UC remain unclear. The novelty of this study lies in uncovering that XBD could ameliorate DSS-induced colitis by reducing inflammation and enhancing intestinal barrier integrity, which were mediated by the mechanism involved in restricting pyroptosis through blockade of IL-17 pathway activation.
Methods and Materials
Establishment of UC Model and Administration of Xuanbi Yuyang Decoction
All ingredients of XBD prescription were provided by The First Affiliated Hospital of Guangxi University of Chinese Medicine, and the XBD was prepared as follows: 15 g of Inula japonica Thunb, 15 g of Rubia cordifolia L, 15 g of pleuropterus Multiflorus, 30 g of Red Peony, 20 g of Poria cocos, 30 g of Alismatis Rhizoma, 15 g of Tree Peony Bark, 30 g of Herba Patriniae, 10 g of Radix Glycyrrhizae, 30 g of Chinese wolfberry root-bark, 15 g of Rhizoma Cimicifugae were mixed, pulverized, and then extracted using ultrasonication three times (60 min each time) with 70% alcohol and 30% pure water. Finally, the collected supernatant underwent rotary evaporation to remove alcohol, then freeze-dried to obtain a powdered form. Before use, an appropriate concentration of XBD was 6.6g powder diluted with 12 mL distilled water to 0.55 g/mL.
The experimental animal study design was based on the previously report described.30 In detail, male BALB/c mice (6–8 weeks, 18–20 g) were purchased from SPF Biotechnology Co., Ltd (Beijing, China), and housed in standard environment. The mice were randomly divided into four groups: Control, dextran sodium sulfate-induced colitis (DSS), low-dose XBD treatment (L-XBD) and high-dose XBD treatment (H-XBD) group (n = 10 per group). In addition to the control group, the mice were allowed to drink 3% DSS (3 g dissolved in 100 mL distilled water) to induce UC, then were monitored daily for body weight changes, diarrhea, and rectal bleeding rectal bleeding. For the control group, the mice were received normal distilled water without DSS. Beginning on day 6, the mice were observed serious rectal bleeding, thus the mice were initiated XBD treatment. The dose of XBD was converted by the body surface area method,31 and the doses for low-, and high-dose groups were set 0.3 mL and 0.4 mL per day, respectively. Meanwhile, the control group and DSS group were intragastrically given distilled water. After consecutive 15 days of XBD treatment, the mice were euthanized through inhalation of isoflurane for 2–3 min, then blood and colon tissues were taken. The animal experiment was approved by the Ethical Committee of The First Affiliated Hospital of Guangxi University of Chinese Medicine (approved number: DW20230525-099) and was conducted in strict compliance with the Animal Care and Use guidelines of The First Affiliated Hospital of Guangxi University of Chinese Medicine.
DAI Score
DAI was analyzed based on a combination of body weight loss, fecal consistency and rectal bleeding score following criteria.32,33 Weight loss: (0, no weight loss; 1, 1–3% weight loss; 2, 3–6% weight loss; 3, 6–9% weight loss; 4, >9% weight loss). The consistency of stool: (0, normal; 1, soft and well-formed; 2, soft without pellets; 4, diarrhea). Rectal bleeding: (0, no blood; 1, visible blood in rectum; 2, grossing bleeding in rectum; 4, visible blood on fur).
Hematoxylin and Eosin (H&E) Staining
The tissues were fixed and cut into 4 μm sections after paraffin embedding. The sections were roasted and dried, dewaxed and hydrated with xylene and ethanol, stained with hematoxylin, differentiated with 0.7% hydrochloric alcohol, and then stained with eosin solution, graded ethanol and xylene were transparent and sealed with neutral glue, and observed under microscope (IX71, Olympus, Tokyo, Japan). In addition, all tissue sections were scored as previously described: inflammatory infiltration (0–5), crypt injury (0–4), ulcer (0–3), and presence or absence of edema (0 or 1).34
Immunohistochemistry (IHC)
Paraffin sections were hydrated with xylene and ethanol and heated in sodium citrate solution, followed by treatment with 0.3% hydrogen peroxide. After blocking, the sections were incubated with primary Anti-Occludin antibody (1:200, ab216327, Abcam) and Anti-ZO-1 antibody (1:500, ab221547, Abcam) overnight at 4°C. Following incubation with secondary antibody (1:500, ab288151, Abcam), the slides were stained with DAB, counterstained with hematoxylin, and visualized using a microscope (Olympus).
Real-Time Quantitative PCR (RT-qPCR)
Total RNA was extracted by TRIZOL reagent (Invitrogen, MA, USA). cDNA templates were synthesized by reverse transcription using PCR amplification apparatus. Real-Time fluorescence quantitative PCR experiments were performed with the ABI7500 quantitative PCR instrument (Applied Biosystems, Waltham, MA, USA). The reaction procedure is: predenaturation at 95°C for 30 s, denaturation at 95°C for 10s, annealing at 60°C for 30 s, 40 cycles. GAPDH was used as the internal parameter, and the experiment was repeated 3 times. Relative mRNA expression of target genes was analyzed by 2−ΔΔCt method. The primer sequences were synthesized by Sangon Biotech Co., Ltd (Shanghai, China) and shown in Supplement Table 1.
Elisa
Pro-inflammatory cytokines such as TNF-α, IL-1β, IFN-γ, IL-17A, IL-6 levels in serum and supernatant of cells were measured using commercial enzyme-linked immunosorbent assay (ELISA) kits (Eusebio, Shanghai, China), following the kit instructions. And the absorbance at 450 nm was detected by a microplate reader (VL0000D0, Thermo Fisher Scientific, Waltham, MA, USA).
Western Blot
The protein samples were extracted and subjected to SDS-PAGE gel electrophoresis, then transferred to PVDF membranes and blocked for 2 h. The membranes were incubated with primary antibody at 4°C overnight and the following antibodies were used for primary antibody incubation: Caspase-1 (1:1000, ab207802, Abcam), GSDMD (1:1000, ab210070, Abcam), NLRP3 (1:1000, ab263899, Abcam), IL-17RA (1:1000, ab180904, Abcam), ACT1 (1:1000, ab137395, Abcam), NF-kB p65 (1:1000, ab32536, Abcam), P-NF-kB p65 (1:1000, ab76302, Abcam), Occludin (1:1000, ab216327, Abcam), ZO-1 (1:1000, ab307799, Abcam), Claudin 1 (1:1000, ab307692, Abcam), GAPDH (1:2500, ab9485, Abcam). The membranes were rinsed with TBST, and incubated with the secondary antibody (1:5000, ab288151, Abcam) for 1 h at room temperature. The blots were photographed and the levels of protein expression were quantified.
Bioinformatics Analysis
First, the gene expression profiles data were collected from the Gene Expression Omnibus (GEO, https://www.ncbi.nih.gov/geo/). Then, in order to select the appropriate dataset, an advanced search was performed by inserting the search term: “colitis”. Three datasets (GSE36807, GSE47908, GSE48958) were determined after screening.
The datasets were processed using GEO2R (www.ncbi.nlm.nih.gov/geo/geo2r) and the genes of the datasets with |logFC|≥1.5 and P<0.05 were considered as differentially expressed genes (DEGs) (UC vs Normal). And visualized DEGs through volcano plot and heat map. Venn diagrams were created to visualize the common DEGs between the three datasets.
Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analysis of DEGs were performed using the Database for Annotation, Visualization, and Integrated Discovery (DAVID, https://david.ncifcrf.gov/summary.jsp) and the results were visualized using R language.
Preparation of Medicated Serum
Male Sprague Dawley rats were respectively given L-XBD, H-XBD and distilled water by gavage for 7 days, twice a day, with 10 rats in each group. On day 7, abdominal aorta blood was collected 1 h after gavage. The serum was extracted by centrifugation, sterilized in a water bath at 56°C for 30 minutes, and stored at −20°C.
Cell Culture
The human colon epithelial cells (NCM460) were purchased from iCell Bioscience Inc (Shanghai, China). The cells were cultured in a modified 1640 medium. Except the control group, the cells were treated with 2% DSS for 24 h. For L-XBD group and H-XBD group, the corresponding medicated containing serum was added after treatment with 2% DSS. Additionally, the cells were treated with IL-17 pathway activator, recombinant human interleukin 17A (rh IL17A; 50ng/mL; Peprotech, Rocky Hill, NJ, USA) for 24h.
Cell Counting Kit-8 (CCK-8)
CCK-8 method was used to detect the viability of cells in each group. The cells at the density of 1 × 103/well were grown in 96-well plates for 0, 24, 48, 72 and 96 h. Then, 10 µL of diluted CCK-8 regents (Beyotime, Shanghai, China) were added to each well for an additional 2 h incubation. The absorbance at 450 nm was finally measured by Microplate Reader (Thermo Fisher Scientific).
Non-Targeted Metabolomics Analysis
Metabolite extraction: The samples were unfreezed on the ice, then vortexed for 30 s, and centrifuged at 12,000 rpm (Heraeus Fresco17; Thermo Fisher Scientific) at 4°C for 15 min. 300 μL of supernatant obtained was transferred to EP tubes, next mixed with 1000 μL extracted solution (methanol: water = 4:1) containing 10 μg/mL of internal standard. Then the samples were vortexed for 30 s, sonicated in an ice-water bath for 1 h and incubated at −40°C for 1 h, and next underwent centrifugation at 12000 rpm at 4°C for 15 min. Finally, the resulting supernatant was filtered through a 0.22 μm microporous membrane and placed at −80°C until subsequent analysis.
Method conditions: Vanquish ultra-high performance liquid chromatography (UHPLC) 1290 system (Thermo Fisher Scientific) equipped with a Waters UPLC BEH C18 column (2.1 × 100 mm ID, particle size 1.7 μm, Waters, USA) was performed for LC-MS/MS analysis. Each sample injection volume was set at 5 μL. The mobile phase consisted of (A) water with 0.1% formic acid and (B) acetonitrile with 0.1% formic acid and conditions in detail are listed in Supplementary Table 2. The primary and secondary mass spectrometry data acquisition (MS/MS) were acquired through the Q Exactive Focus mass spectrometer under the control of the control software (Xcalibur, Thermo) based on the IDA acquisition mode. During each acquisition cycle, the mass range was from 100 to 1500, and the top three of every cycle were screened and the corresponding MS/MS data were further acquired. Specifications were as follows: sheath gas flow rate: 30 Arb, auxiliary gas flow rate: 10 Arb, capillary temperature: 350°C, full ms resolution: 70000, MS/MS resolution: 17500, collision energy: 15/30/45 in NCE mode, spray voltage: 5.5 kV (positive) or −4.0 kV (negative).
Statistical Analysis
All statistical analyses were performed using GraphPad Prism 8.0 software (GraphPad Software, Inc., La Jolla, CA, USA). Data were expressed as mean ± standard deviation. Student’s t-test was utilized to verify differences between two sets of data. One-way analysis of variance (ANOVA) followed by Tukey post hoc analysis was applied when evaluating differences among multiple groups. All experiments were performed at least three times and P<0.05 was considered statistically significant.
Results
The Chemical Composition of XBD
The chemical composition of XBD was determined through UHPLC-QE-MS assay with top 10 chemical components labelled in the positive and negative electrospray ionization modes, respectively, suggesting XBD had multiple pharmacological effects (Figure 1A and B, Supplementary Tables 3 and 4).
 |
Figure 1 Xuanbi yuyang decoction (XBD) chemical components was detected by UHPLC-QE-MS assay. (A) The total ion chromatography of XBD with top 10 chemical components labelled in the positive electrospray ionization modes. (B) The total ion chromatography of XBD with top 10 chemical components labelled in the negative electrospray ionization modes. |
XBD Attenuates DSS-Induced Murine Colitis
The potential therapeutic impact of XBD on UC was scrutinized by establishing a DSS-induced colitis mice model, which is illustrated in Figure 2A. Compared with control group, mice treated with DSS showed the body weight loss and increased the trend of DAI scores (P<0.001), which were alleviated after XBD treatment and this therapeutic effect became more pronounced with higher doses of XBD supplementation (Figure 2B and C). Furthermore, the colon length in the DSS group was shorter than that in the control group (P<0.001), while XBD supplementation restored DSS-induced colon shortening (Figure 2D). Meanwhile, disordered colon tissue cells reduced the number of normal cells, inflammatory cell infiltration, and elevated histopathology scores were observed in the DSS group, which were mitigated by XBD treatment including more normal cells, slightly normal villi, and a reduction in inflammatory cells (Figure 2E and F). These results suggested that XBD improved the pathologic symptoms of colitis and high dose XBD exhibited preferable therapeutic effect.
 |
Figure 2 The protective effect of Xuanbi yuyang decoction (XBD) on DSS-induced colitis mice. (A) DSS-induced colitis mouse model construction and XBD treatment process diagram. (B and C) The body weight and disease activity index (DAI) of these mice during the experimental period were depicted. (D) Representative images of colon lengths from a macroscopic perspective and quantitative measurement of colon length. (E) The pathological features of colitis were depicted by HE staining (Amplification: 200×, Scale: 100 μm). (F) The histopathology score of each group. ***P<0.001 vs Control; ###P<0.001, ##P<0.01, #P<0.05 vs DSS. |
XBD Repairs the Integrity of the Intestinal Epithelial Barrier
To determine whether XBD treatment of UC was associated with repair of the intestinal epithelial barrier, we examined the expression of TJs-related proteins. The IHC results showed that DSS caused a remarkable decrease in Occludin and zonula occludens-1 (ZO-1) proteins expression in colon tissues, whereas XBD inhibited their decrease, and this inhibitory effect was more apparent in the H-XBD group (Figure 3A). Consistently, the mRNA expression of Occludin, ZO-1 and Claudin-1 was decreased after DSS induction compared to the control group, which were partially reversed upon XBD treatment (Figure 3B). Collectively, the above data indicated that XBD can help repair the damage of intestinal epithelial barrier caused by DSS in mice.
 |
Figure 3 The effect of intestinal epithelial barrier repair of Xuanbi yuyang decoction (XBD) on DSS-induced colitis mice. (A) The expression of Occludin and ZO-1 was indicated by immunohistochemistry assay (Amplification: 200×, Scale: 100 μm). (B) RT-qPCR was used to measure the levels of intestinal tight junction proteins such as Occludin, ZO-1, and Claudin-1. ***P<0.001 vs Control; ###P<0.001, ##P<0.01, #P<0.05 vs DSS. |
XBD Decreases the Expression Level of Proinflammatory Factor and Inhibits Pyroptosis in Mice with Colitis
Next, we evaluated the role of XBD on the inflammatory response induced by DSS in vivo. The expression levels of pro-inflammatory factors (TNF-α, IL-1β, IFN-γ) in each group were detected by ELISA, and the results showed that DSS triggered elevated levels of the above factors in serum compared to controls (P<0.001, Figure 4A). Conversely, XBD supplementation remarkably attenuated this tendency. To verify the effect of XBD on pyroptosis, we examined the hallmarks related to pyroptosis. The expressions of Caspase-1, GSDMD and NLRP3 in colitis model mice presented an increased trend compared to the control group (P<0.001, Figure 4B), while XBD treatment displayed an effective decrease in their expression levels. In conclusion, XBD reduced the inflammation resulting from DSS, in part by downregulating the expression of inflammation-associated genes and further inhibited the occurrence of pyroptosis.
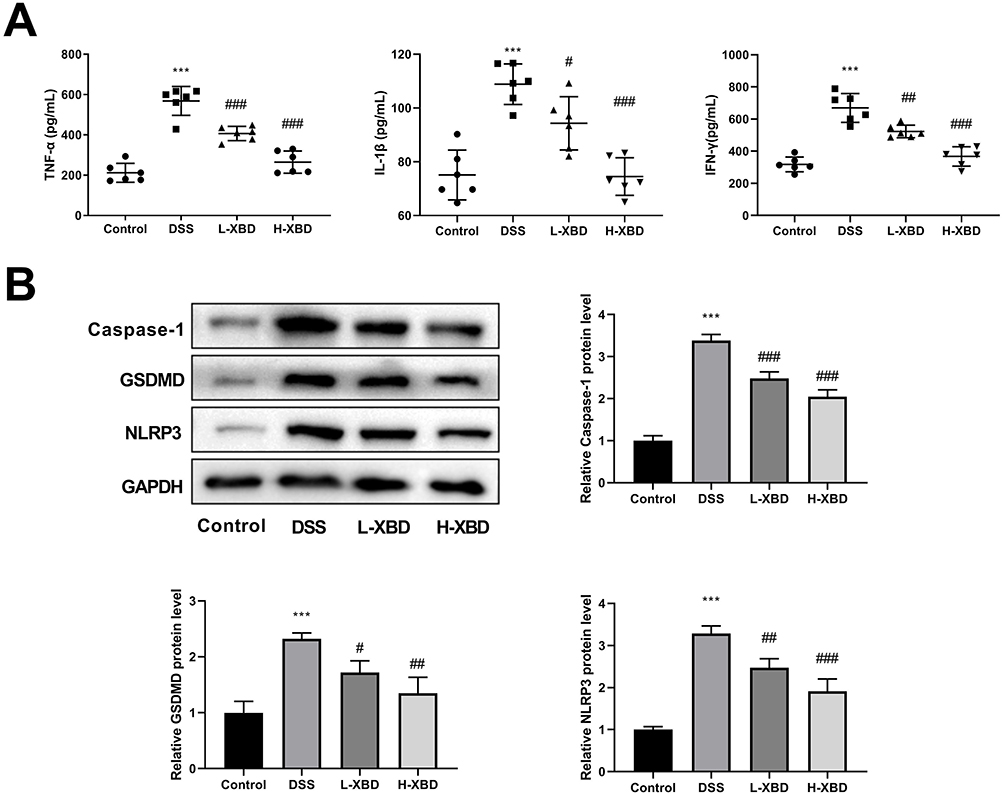 |
Figure 4 Xuanbi yuyang decoction (XBD) reduced the level of pro-inflammatory cytokines and inhibited pyroptosis in dextran sulfate sodium (DSS)-induced colitis mice. (A) Serum levels of inflammatory factors (TNF-α, IL-1β, IFN-γ) were detected by ELISA. (B) The expression of pyroptosis related proteins (Caspase-1, GSDMD, NLRP3) was detected by Western blot. ***P<0.001 vs Control; ###P<0.001, ##P<0.01, #P<0.05 vs DSS. |
Effects of XBD on UC Cell Model
We then investigated XBD potential role in DSS-induced NCM460 cells. The viability was decreased in DSS group compared to the control group (P<0.001), while it was improved after XBD treatment especially in H-XBD group (Figure 5A). Furthermore, the levels of inflammatory cytokines in the DSS group were more markedly elevated than those in the control group (P<0.001), and XBD reduced the increase in TNF-α, IL-1β, and IFN-γ levels (Figure 5B). Upon the treatment of XBD, the damage of intestinal epithelial barrier was alleviated, as evidenced by the increase of protein expression of Occludin, ZO-1 and Claudin-1 (Figure 5C). Additionally, the protein expression levels of Caspase-1, GSDMD and NLRP3 were higher in DSS group than those in the control group (P<0.001), whereas the decreased expressions were found in L-XBD group, and more obvious in H-XBD group (Figure 5D).
 |
Figure 5 Effects of XBD on UC cell model. (A) Cell viability was measured by a CCK-8 assay. (B) The levels of TNF-α, IL-1β, and IFN-γ were detected by ELISA. (C) The protein expression levels of Occludin, ZO-1 and Claudin-1 were determined. (D) The levels of Caspase-1, GSDMD and NLRP3 were evaluated using Western blot. ***P<0.001, **P<0.01 vs Control; ###P<0.001, ##P<0.01, #P<0.05 vs DSS. |
Analysis of Potential Pathways Involved in Colitis
In this study, three datasets GSE36807, GSE47908 and GSE48958 were selected based on the keyword “colitis”. The gene datasets GSE36807, GSE47908 and GSE48958 contained colitis samples (15 samples) vs healthy controls (7 samples), colitis samples (19 samples) vs healthy controls (15 samples) and colitis samples (7 samples) vs healthy controls (8 samples), respectively. After processing using the GEO2R, 303 DEGs were screened out by GSE36807, 681 DEGs by GSE47908, and 461 DEGs by GSE489585. Volcano plots were drawn for the DEGs (Supplement Figure 1A-C) and datasets enrichment analysis was performed, and the three most significant pathways were selected for display (Supplement Figure 1D-F). Heat maps of the top 15 up- and down-regulated genes by DEGs in their respective datasets were drawn for visualization (Supplement Figure 2A-C). Venn diagrams were drawn for three datasets, and 124 common DGEs were screened out (Supplement Figure 2D).
Next, we explored the possible functions of these common DEGs and the signaling pathways affected. The GO enrichment analysis of DEGs contained three parts: biological process (BP), cell component (CC), and molecular function (MF). The results showed that the BP were enriched in antimicrobial humoral immune response mediated by antimicrobial peptide, neutrophil chemotaxis, inflammatory response, cellular response to lipopolysaccharide, chemokine-mediated signaling pathway, and response to lipopolysaccharide. The CC were enriched in extracellular region, extracellular space, extracellular matrix, extracellular exosome, and apical plasma membrane. The MF were enriched in CXCR chemokine receptor binding, chemokine activity, serine-type endopeptidase activity, oligosaccharide binding, and CXCR3 chemokine receptor binding (Figure 6A). In addition, the KEGG analysis showed that the DEGs were largely enriched in IL-17 signaling pathway, tryptophan metabolism, complement and coagulation cascades, amoebiasis, pertussis, and rheumatoid arthritis (Figure 6B).
 |
Figure 6 Functional enrichment analysis of common differentially expressed genes. (A) Bar chart of GO enrichment analysis result. (B) KEGG enrichment analysis bubble chart, the color depth of the points indicates the corrected P-value, and the size of the points refers to the number of genes involved. |
The Regulation of XBD on IL-17 Signaling Pathway
To confirm the potential regulatory action of XBD on the IL-17 pathway, we examined the expression levels of IL-17 pathway-related proteins in colon tissues and NCM460 cells of each group. The data indicated that IL-17RA, Act1 and P-NF-κB P65/NF-κB P65 protein expression levels were elevated in DSS group than those in the control group (P<0.001), while were decreased with the intervention of XBD (Figure 7A and B). In addition, compared to the control group, the concentration of cytokines including IL-17A and IL-6 in serum were up-regulated in the DSS group (P<0.001), but were suppressed with significant differences after the XBD treatment (Figure 7C). Consistently, XBD reduced the effect of DSS on reducing IL-17A and IL-6 in the supernatant of NCM460 cells (Figure 7D). These results indicated that XBD may be involved in the regulation of expression of IL-17 pathway in DSS-induced colitis.
 |
Figure 7 The regulation of XBD on IL-17 signaling pathway. (A) The expression of IL-17 pathway related proteins (IL-17RA, Act1, NF-κB P65, p-NF-κB P65) in colon tissues of each group was detected by Western blot. (B) The protein expression of IL-17RA, Act1, NF-κB P65, and p-NF-κB P65 in NCM460 cells of each group were determined. (C) ELISA was used to detect the expression levels of cytokines IL-17A and IL-6 in serum of each group. (D) The content of IL-17A and IL-6 in the supernatant of each group were assessed. ***P<0.001 vs Control; ###P<0.001, ##P<0.01, #P<0.05 vs DSS. |
XBD Improves DSS-Induced Colitis via IL-17 Pathway and Pyroptosis
To investigate whether XBD can regulate pyroptosis through IL-17 signaling pathway to improve DSS-induced colitis, the IL-17 pathway activator, rhIL17A was employed. The rhIL17A treatment partially reversed the improved effect of H-XBD intervention on viability (Figure 8A). The levels of inflammatory cytokines in H-XBD+rhIL17A treatment group exhibited significant increase than those in H-XBD group (P<0.01, Figure 8B). Upon the treatment of rhIL17A, the damage of intestinal epithelial barrier was aggravated compared to the H-XBD group, as evidenced by the decrease of protein expression of Occludin, ZO-1 and Claudin-1 (P<0.01, Figure 8C). Additionally, compared to the H-XBD group, the protein expression levels of Caspase-1, GSDMD and NLRP3 were elevated in the H-XBD+rhIL17A treatment group (P<0.01, Figure 8D). The above findings indicated that XBD may regulate pyroptosis through IL-17 signaling pathway to alleviate DSS-induced colitis.
 |
Figure 8 XBD improves DSS-induced colitis via IL-17 pathway and pyroptosis. (A) Cell viability was detected by CCK-8 assay. (B) ELISA was used to detect the levels of pro-inflammatory cytokines TNF-α, IL-1β and IFN-γ. (C) Western blot was used to detect the expression of tight junction related proteins Occludin, ZO-1 and Claudin-1. (D) The protein expression levels of Caspase-1, GSDMD and NLRP3 were measured using Western blot. ***P<0.001, vs Control; ###P<0.001 vs DSS. $$$P<0.001, $$P<0.01 vs H-XBD. |
Discussion
UC is a chronic inflammatory disease with increasing incidence, extremely high recurrence rate and low cure, which makes it a hot spot in clinical research. Hence, further analyzing the etiology of UC help us to gain a better understanding of UC and find more potent therapeutic options. In this study, we found that XBD treatment attenuated DSS-induced colitis, as indicated by increased weight, decline of DAI score, restored the intestinal epithelial barrier, and decreased the inflammatory response, which may modulate pyroptosis via IL-17 signaling pathway.
Abundant Chinese herbal medicines and agents have been shown to have powerful anti-inflammatory effect and play a certain therapeutic effect on intestinal diseases.11 For instance, Poria cocos can alleviate drug-induced experimental colon injury, and its oligosaccharides improve DSS-induced colitis by reversing the changes of intestinal microbiota in mice indigestion.19,35,36 Traditional Chinese medicine formulations such as Huaihua Powder, Huangqin Decoction, Lizhong Decoction, Rhubarb Peony Decoction are proved to improve the pathological symptoms of UC by regulating colon barrier dysfunction, balancing intestinal microflora and reducing inflammatory response.37–41 In this study, we found that XBD could significantly reduce the weight loss, colon shortening and inflammatory cell infiltration in mice with DSS-induced colitis, suggesting that XBD treatment can be a useful way to relieve the clinical symptoms of colitis.
The defect of intestinal TJ barrier is also an important factor leading to various intestinal inflammation.42,43 It is found that IL-1β can promote intestinal inflammation by destroying intestinal TJ barrier,44 thus reducing proinflammatory cytokines release and the repair of intestinal TJ barrier are usually deemed as therapeutic targets for intestinal inflammatory diseases.6,45 Furthermore, the expression of pro-inflammatory cytokines has been confirmed to be significantly increased under intestinal inflammatory conditions and was further increased after DSS induction, highlighting the potentially essential contribution of these cytokines in the etiopathogenesis of IBD.46,47 Herein, our study was concerned with both the anti-inflammatory and intestinal mucosal repair effects of XBD in colitis. The results showed that XBD could restore intestinal epithelial barrier damage by up-regulating the contents of Occludin, ZO-1, and Claudin-1 expression, and inhibit the release of TNF-α, IL-1β and IFN-γ. Similar effects were also observed in DSS+XBD group of human colon epithelial cells in vitro, which further confirmed the role of XBD in the protection of UC.
IL-17 has also been implicated as a major pathogenic factor in IBD.48 More pro-inflammatory factors such as TNF-α and IL-6 are released after IL-17 signaling pathway activation, which leads to aggravation of inflammation.49 It is also observed that the expression of IL-17 is elevated in the serum of UC patients.50 Qingchang Suppository exhibited the inhibitory role in the IL-17A signaling pathway in HT-29 cells and DSS-induced mice.51 Cheng et al have found that Qingchang Wenzhong Decoction can treat UC, which is highly associated with the IL-17 signaling pathway.52 It is worth noting that pyroptosis is closely related to a sustained inflammatory response, and the link between pyroptosis and UC has attracted strong interest from researchers.22 Herein, we demonstrated that IL-17 pathway was participated in UC using bioinformatics analysis, and then confirmed that IL-17 pathway was abnormally activated in DSS-treated cell and mice model, which were remarkably depressed after XBD intervention. Moreover, we verified that DSS treatment promoted pyroptosis in vivo and vitro, and XBD intervention was able to attenuate the DSS-induced increase in the expression of Caspase-1, GSDMD, and NLRP3, implying that the curative action of XBD on UC was relevant to the inhibition of pyroptosis. In addition, the rhIL17A treatment partially reversed the effect of H-XBD intervention on improved viability, decreased inflammatory cytokines levels, restored the damage of intestinal epithelial barrier, and the downregulated protein expression levels of pyroptosis hallmarks.
To summarize, this study indicated that XBD could alleviate DSS-induced colitis by reducing inflammation and enhancing intestinal barrier integrity, which may restrain pyroptosis through inhibition of IL-17 signaling pathway activation. Collectively, our research demonstrated the feasibility of XBD as a therapeutic medicine for UC and provided new ideas and options for the clinical treatment of UC with herbal medicine in the future.
Data Sharing Statement
The data are available on request from the corresponding author.
Ethical Approval
The animal experiment was approved by the Ethical Committee of The First Affiliated Hospital of Guangxi University of Chinese Medicine (approved number: DW20230525-099) and was conducted in strict compliance with the Animal Care and Use guidelines of The First Affiliated Hospital of Guangxi University of Chinese Medicine in accordance with the ARRIVE guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was supported by National Natural Science Foundation of China (82360907), National Administration of Traditional Chinese Medicine, Guangxi TCM Key Research Office (GZYYKJF 2023 No. 9), Department of Science and Technology of Guangxi Zhuang Autonomous Region (2020GXNSFAA238009) and Guangxi Medical and Health Key Disciplines Declaration Project (GWKJF 2023 No.1).
Disclosure
Xiaoyan Huang and Liqun Li are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Xavier RJ, Podolsky DK. Unravelling the pathogenesis of inflammatory bowel disease. Nature. 2007;448(7152):427–434. doi:10.1038/nature06005
2. Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults: American college of gastroenterology, practice parameters committee. Am J Gastroenterol. 2010;105(3):501–523; quiz524. doi:10.1038/ajg.2009.727
3. Yashiro M. Ulcerative colitis-associated colorectal cancer. World J Gastroenterol. 2014;20(44):16389–16397. doi:10.3748/wjg.v20.i44.16389
4. Shafran I, Burgunder P, Wei D, Young HE, Klein G, Burnett BP. Management of inflammatory bowel disease with oral serum-derived bovine immunoglobulin. Ther Adv Gastroenterol. 2015;8(6):331–339. doi:10.1177/1756283X15593693
5. Troncone E, Monteleone G. The safety of non-biological treatments in ulcerative colitis. Expert Opin Drug Saf. 2017;16(7):779–789. doi:10.1080/14740338.2017.1340936
6. Kobayashi T, Siegmund B, Le Berre C, et al. Ulcerative colitis. Nature Reviews Disease Primers. 2020;6(1):74. doi:10.1038/s41572-020-0205-x
7. Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet. 2017;389(10080):1756–1770.
8. Li L, Zhang Y, Luo Y, et al. The molecular basis of the anti-inflammatory property of astragaloside iv for the treatment of diabetes and its complications. Drug Des Devel Ther. 2023;17:771–790. doi:10.2147/DDDT.S399423
9. Waswa EN, Li J, Mkala EM, et al. Ethnobotany, phytochemistry, pharmacology, and toxicology of the genus Sambucus L. (Viburnaceae). J Ethnopharmacol. 2022;292:115102. doi:10.1016/j.jep.2022.115102
10. Mutinda ES, Mkala EM, Ren J, et al. A review on the traditional uses, phytochemistry, and pharmacology of the genus Veronicastrum (Plantaginaceae). J Ethnopharmacol. 2023;300:115695. doi:10.1016/j.jep.2022.115695
11. Yang Y, Wang Y, Zhao L, et al. Chinese herbal medicines for treating ulcerative colitis via regulating gut microbiota-intestinal immunity axis. Chin Herb Med. 2023;15(2):181–200. doi:10.1016/j.chmed.2023.03.003
12. Lu PD, Yuan MC, Quan XP, Chen JF, Zhao YH. Preclinical studies of licorice in ulcerative colitis: a systematic review with meta-analysis and network pharmacology. J Ethnopharmacol. 2022;296:115444. doi:10.1016/j.jep.2022.115444
13. Lin L, Ni B, Lin H, et al. Traditional usages, botany, phytochemistry, pharmacology and toxicology of Polygonum multiflorum Thunb.: a review. J Ethnopharmacol. 2015;159:158–183. doi:10.1016/j.jep.2014.11.009
14. Dong X, Fu J, Yin X, et al. Emodin: a Review of its Pharmacology, Toxicity and Pharmacokinetics. Phytother Res. 2016;30(8):1207–1218.
15. Wang X, Zhao L, Han T, Chen S, Wang J. Protective effects of 2,3,5,4’-tetrahydroxystilbene-2-O-beta-d-glucoside, an active component of Polygonum multiflorum Thunb, on experimental colitis in mice. Eur J Pharmacol. 2008;578(2–3):339–348.
16. Li D, Zhang N, Cao Y, et al. Emodin ameliorates lipopolysaccharide-induced mastitis in mice by inhibiting activation of NF-κB and MAPKs signal pathways. Eur J Pharmacol. 2013;705(1–3):79–85. doi:10.1016/j.ejphar.2013.02.021
17. Gong L, Zou W, Zheng K, Shi B, Liu M. The Herba Patriniae (Caprifoliaceae): a review on traditional uses, phytochemistry, pharmacology and quality control. J Ethnopharmacol. 2021;265:113264. doi:10.1016/j.jep.2020.113264
18. Tian T, Chen H, Zhao YY. Traditional uses, phytochemistry, pharmacology, toxicology and quality control of Alisma orientale (Sam.) Juzep: a review. J Ethnopharmacol. 2014;158:373–387. doi:10.1016/j.jep.2014.10.061
19. Zou YT, Zhou J, Wu CY, et al. Protective effects of Poria cocos and its components against cisplatin-induced intestinal injury. J Ethnopharmacol. 2021;269:113722. doi:10.1016/j.jep.2020.113722
20. He WT, Wan H, Hu L, et al. Gasdermin D is an executor of pyroptosis and required for interleukin-1β secretion. Cell Res. 2015;25(12):1285–1298.
21. Zhang C, Zhu H, Jie H, Ding H, Sun H. Arbutin ameliorated ulcerative colitis of mice induced by dextran sodium sulfate (DSS). Bioengineered. 2021;12(2):11707–11715. doi:10.1080/21655979.2021.2005746
22. Chen K, Shang S, Yu S, Cui L, Li S, He N. Identification and exploration of pharmacological pyroptosis-related biomarkers of ulcerative colitis. Front Immunol. 2022;13:998470.
23. Eyerich K, Dimartino V, Cavani A. IL-17 and IL-22 in immunity: driving protection and pathology. Eur J Immunol. 2017;47(4):607–614. doi:10.1002/eji.201646723
24. Chiricozzi A, Guttman-Yassky E, Suárez-Fariñas M, et al. Integrative responses to IL-17 and TNF-α in human keratinocytes account for key inflammatory pathogenic circuits in psoriasis. J Invest Dermatol. 2011;131(3):677–687. doi:10.1038/jid.2010.340
25. Taams LS, Steel KJA, Srenathan U, Burns LA, Kirkham BW. IL-17 in the immunopathogenesis of spondyloarthritis. Nat Rev Rheumatol. 2018;14(8):453–466. doi:10.1038/s41584-018-0044-2
26. Brembilla NC, Senra L, Boehncke WH. The IL-17 Family of Cytokines in Psoriasis: IL-17A and Beyond. Front Immunol. 2018;9:1682.
27. Berry SPD, Dossou C, Kashif A, et al. The role of IL-17 and anti-IL-17 agents in the immunopathogenesis and management of autoimmune and inflammatory diseases. Int Immunopharmacol. 2022;102:108402. doi:10.1016/j.intimp.2021.108402
28. Fujino S, Andoh A, Bamba S, et al. Increased expression of interleukin 17 in inflammatory bowel disease. Gut. 2003;52(1):65–70. doi:10.1136/gut.52.1.65
29. Lee C, Song JH, Cha YE, Chang DK, Kim YH, Hong SN. Intestinal epithelial responses to IL-17 in adult stem cell-derived human intestinal organoids. J Crohn’s Colitis. 2022;16(12):1911–1923. doi:10.1093/ecco-jcc/jjac101
30. Liu J, Lin H, Cao M, et al. Shifts and importance of viable bacteria in treatment of DSS-induced ulcerative colitis mice with FMT. Front Cell Infect Microbiol. 2023;13:1124256. doi:10.3389/fcimb.2023.1124256
31. Reagan-Shaw S, Nihal M, Ahmad N. Dose translation from animal to human studies revisited. FASEB J. 2008;22(3):659–661.
32. Zhang Z, Kong L, Lv M, et al. PVA enema ameliorates DSS-induced acute colitis in mice. BMC Gastroenterol. 2023;23(1):368.
33. Guo H, Guo H, Xie Y, et al. Mo3Se4 nanoparticle with ROS scavenging and multi-enzyme activity for the treatment of DSS-induced colitis in mice. Redox Biol. 2022;56:102441.
34. Peng Y, Yan Y, Wan P, et al. Gut microbiota modulation and anti-inflammatory properties of anthocyanins from the fruits of Lycium ruthenicum Murray in dextran sodium sulfate-induced colitis in mice. Free Radic Biol Med. 2019;136:96–108.
35. Ji HJ, Kang N, Chen T, et al. Shen-ling-bai-zhu-san, a spleen-tonifying Chinese herbal formula, alleviates lactose-induced chronic diarrhea in rats. J Ethnopharmacol. 2019;231:355–362. doi:10.1016/j.jep.2018.07.031
36. Lan K, Yang H, Zheng J, et al. Poria cocos oligosaccharides ameliorate dextran sodium sulfate-induced colitis mice by regulating gut microbiota dysbiosis. Food Funct. 2023;14(2):857–873. doi:10.1039/D2FO03424G
37. Liu P, Bian Y, Liu T, et al. Huai hua san alleviates dextran sulphate sodium-induced colitis and modulates colonic microbiota. J Ethnopharmacol. 2020;259:112944. doi:10.1016/j.jep.2020.112944
38. Yang Y, Chen G, Yang Q, et al. Gut microbiota drives the attenuation of dextran sulphate sodium-induced colitis by Huangqin decoction. Oncotarget. 2017;8(30):48863–48874. doi:10.18632/oncotarget.16458
39. Zou J, Shen Y, Chen M, et al. Lizhong decoction ameliorates ulcerative colitis in mice via modulating gut microbiota and its metabolites. Appl Microbiol Biotechnol. 2020;104(13):5999–6012. doi:10.1007/s00253-020-10665-1
40. Luo S, Wen R, Wang Q, et al. Rhubarb Peony Decoction ameliorates ulcerative colitis in mice by regulating gut microbiota to restoring Th17/Treg balance. J Ethnopharmacol. 2019;231:39–49. doi:10.1016/j.jep.2018.08.033
41. Li MY, Luo HJ, Wu X, et al. Anti-inflammatory effects of huangqin decoction on dextran sulfate sodium-induced ulcerative colitis in mice through regulation of the gut microbiota and suppression of the Ras-PI3K-Akt-HIF-1α and NF-κB pathways. Front Pharmacol. 2019;10:1552.
42. König J, Wells J, Cani PD, et al. Human intestinal barrier function in health and disease. Clin Transl Gastroenterol. 2016;7(10):e196. doi:10.1038/ctg.2016.54
43. Salvo Romero E, Alonso Cotoner C, Pardo Camacho C, Casado Bedmar M, Vicario M. The intestinal barrier function and its involvement in digestive disease. Rev Esp Enferm Dig. 2015;107(11):686–696. doi:10.17235/reed.2015.3846/2015
44. Rawat M, Nighot M, Al-Sadi R, et al. IL1B increases intestinal tight junction permeability by up-regulation of MIR200C-3p, which degrades occludin mRNA. Gastroenterology. 2020;159(4):1375–1389.
45. Ho GT, Cartwright JA, Thompson EJ, Bain CC, Rossi AG. Resolution of inflammation and gut repair in IBD: translational steps towards complete mucosal healing. Inflamm Bowel Dis. 2020;26(8):1131–1143.
46. Yao D, Dong M, Dai C, Wu S. Inflammation and inflammatory cytokine contribute to the initiation and development of ulcerative colitis and its associated cancer. Inflamm Bowel Dis. 2019;25(10):1595–1602.
47. Neurath MF. Cytokines in inflammatory bowel disease. Nat Rev Immunol. 2014;14(5):329–342. doi:10.1038/nri3661
48. McGeachy MJ, Cua DJ, Gaffen SL. The IL-17 Family of Cytokines in Health and Disease. Immunity. 2019;50(4):892–906. doi:10.1016/j.immuni.2019.03.021
49. Gaffen SL, Jain R, Garg AV, Cua DJ. The IL-23-IL-17 immune axis: from mechanisms to therapeutic testing. Nat Rev Immunol. 2014;14(9):585–600.
50. Moschen AR, Tilg H, Raine T. IL-12, IL-23 and IL-17 in IBD: immunobiology and therapeutic targeting. Nat Rev Gastroenterol Hepatol. 2019;16(3):185–196. doi:10.1038/s41575-018-0084-8
51. Zhou G, Kong WS, Li ZC, Xie RF, Yu TY, Zhou X. Effects of Qing Chang suppository powder and its ingredients on IL-17 signal pathway in HT-29 Cells and DSS-induced Mice. Phytomedicine. 2021;87:153573. doi:10.1016/j.phymed.2021.153573
52. Cheng Y, Li J, Zhang X, et al. Protective effect of qingchang wenzhong decoction on colitis and colitis-related carcinogenesis by regulating inflammation and intestinal fibrosis. J Inflamm Res. 2023;16:1479–1495. doi:10.2147/JIR.S402395
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.