")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 18
Diagnosis and Management of Gastroesophageal Reflux Disease: Current Insights
Authors Vayal-Veettil A , Gyawali CP
Received 9 June 2025
Accepted for publication 4 July 2025
Published 8 July 2025 Volume 2025:18 Pages 149—162
DOI https://doi.org/10.2147/CEG.S507237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Santosh Shenoy
Abhinav Vayal-Veettil,1,* C Prakash Gyawali2,*
1Department of Internal Medicine, Cleveland Clinic Foundation, Cleveland, Ohio, USA; 2Division of Gastroenterology, Washington University School of Medicine, St. Louis, Missouri, USA
*These authors contributed equally to this work
Correspondence: C Prakash Gyawali, Professor of Medicine Division of Gastroenterology, 660 South Euclid Ave., Campus Box 8124, Saint Louis, Missouri, MO 63110, USA, Tel +1 314-454-8201, Fax +1 314-362-3643, Email [email protected]
Abstract: Gastroesophageal reflux disease (GERD) results from retrograde movement of gastric content into the esophagus and beyond, resulting in symptoms, mucosal injury and long-term complications. Typical symptoms of heartburn and regurgitation are highly suggestive of GERD, but atypical presentations require careful evaluation to rule out alternative diagnoses. Diagnostic modalities, including endoscopy, ambulatory reflux monitoring, and high-resolution manometry, play a pivotal role in confirming GERD and guiding personalized treatment. Management strategies consist of lifestyle modifications, pharmacologic therapy with anti-secretory agents, and adjunctive treatments such as alginates and baclofen. For refractory cases, surgical and endoscopic interventions offer durable symptom relief. Complications of GERD can be esophageal or extraesophageal, and highlight the importance of early diagnosis and effective management. The prognosis for GERD is generally favorable with appropriate treatment, although refractory cases require a tailored approach to address overlapping conditions such as disorders of gut-brain interaction and behavioral disorders. A multidisciplinary, patient-centered approach optimizes outcomes and improves the quality of life for individuals with GERD. This review provides a comprehensive overview of current insights into GERD, focusing on clinical presentation, diagnostic strategies, and therapeutic options.
Keywords: heartburn, laryngopharyngeal symptoms, ambulatory reflux monitoring, proton pump inhibitors, potassium-competitive acid blockers, antireflux surgery
Introduction
Gastroesophageal reflux disease (GERD) is characterized by symptoms and/or complications from the retrograde movement of gastric contents into the esophagus.1 The prevalence of GERD is increasing worldwide and is believed to affect 8–33% of the world population.2 Rates vary by region, with higher prevalence in Western countries and the United States (10–30%), while Western Asia (10–20%), the Middle East (8.7–33.1%), and Eastern Asia (<10%) report lower prevalence.3 The healthcare burden of reflux disease is over $10 billion in the United States alone,4 driven by the costs of diagnostic testing, long-term pharmacotherapy, and management of complications. The economic burden is further compounded by the need for invasive intervention in refractory cases and the ongoing debate about the appropriateness of long-term antisecretory therapy.
The Montreal Consensus introduced a symptomatic definition of GERD, where troublesome symptoms and/or complications could contribute to the diagnosis of GERD.5 However, symptoms attributed to GERD are not always substantiated by objective reflux evidence on esophageal testing.6 Further, as many as half of all patients given empirical proton pump inhibitor (PPI) therapy report inadequate symptom relief.7 The modern definition of actionable GERD requires conclusive evidence of reflux-related pathology, either endoscopic (eg, esophagitis, Barrett’s esophagus) or based on ambulatory reflux monitoring using Lyon consensus thresholds, in the presence of compatible symptoms.8,9 This review aims to provide a comprehensive overview of current insights into the diagnosis and management of GERD, emphasizing evidence-based approaches and recent advancements in the field.
Symptoms of Gastroesophageal Reflux Disease
The spectrum of GERD symptoms can be categorized into typical and atypical symptoms (Table 1). Typical GERD symptoms include heartburn, acid regurgitation, and esophageal chest pain. Heartburn, described as a burning sensation beneath the breastbone, is the most prevalent and recognizable symptom of GERD. Heartburn can be triggered by meals, lying down, or bending over and is often relieved temporarily by antacids or antisecretory medications. Retrosternal chest pain, another typical symptom, can mimic cardiac pain, making it essential to rule out a cardiac etiology first in patients in whom coronary disease could coexist. While empiric treatment with PPIs can provide symptomatic relief in many patients, a significant placebo effect (10–25%) complicates the interpretation of treatment response.10 Moreover, both heartburn and chest pain can arise from other conditions, such as esophageal motor disorders (eg, achalasia) or functional gastrointestinal disorders, emphasizing the need for objective diagnostic confirmation.
 |
Table 1 Typical and Atypical Symptoms of Gastroesophageal Reflux Disease |
Regurgitation, the effortless retrograde movement of gastric contents into the mouth, is another typical symptom of GERD. Unlike heartburn, regurgitation often persists despite acid suppression, which converts acidic reflux into weakly acidic or non-acidic reflux. Regurgitation can cause significant discomfort and impair quality of life. Regurgitation must be carefully differentiated from rumination, a behavioral disorder characterized by an often pleasurable postprandial regurgitation that ceases when the regurgitate becomes acidic.11 Rumination is treated with behavioral therapy and not acid suppression or antireflux surgery, underscoring the importance of accurate symptom differentiation in guiding treatment.
Atypical symptoms of GERD include laryngopharyngeal symptoms (LPS), of which chronic cough, throat clearing, hoarseness, voice change, mucus in throat may have a low but relevant relationship to laryngopharyngeal reflux disease (LPRD) in some individuals.12 Chronic cough and throat clearing are infrequently attributable to GERD but may occur as part of a hyperresponsive state where reflux can be one among several triggers such as abrupt changes in temperature or humidity, prolonged talking, strong odors, and postnasal drip. Wheezing and asthma can sometimes improve with aggressive reflux management, underscoring the relationship to GERD in some instances.13 Globus sensation (the feeling of a lump in the throat) can be a negative predictor of reflux disease and is often influenced by cognitive or behavioral factors.14,15 Hoarseness, dyspepsia, nausea and abdominal pain also have a lower likelihood of being directly caused by reflux. Heartburn may be mischaracterized as epigastric or abdominal pain, where testing can differentiate GERD from other potential causes of these symptoms.16 Gastric belching occurs from venting of swallowed air during transient lower esophageal sphincter relaxations (TLESRs), which are also the primary mechanism underlying reflux; therefore, reflux can occur concurrent with belching in some patients.17 However, supragastric belching is a behavioral disorder, even though this can also trigger reflux, further complicating the diagnostic picture.18
Dysphagia in the context of GERD can occur from reflux-induced esophageal strictures, advanced erosive esophagitis or rarely, esophageal cancer. In the absence of typical symptoms, dysphagia may indicate a non-GERD process such as eosinophilic esophagitis when accompanied by food impaction, or a motility disorder (eg achalasia) or neoplasia when associated with weight loss.
Therefore, although typical symptoms like heartburn and regurgitation are strongly suggestive, they are not pathognomonic of GERD and require corroborative diagnostic evidence. Atypical symptoms, though less specific, can still be associated with GERD in certain contexts, necessitating a comprehensive evaluation to rule out other causes and guide appropriate management.
Diagnosis of Gastroesophageal Reflux Disease
The diagnosis of GERD relies on clinical presentation, response to empiric therapy trials, and findings on objective testing8 (Table 2). While empiric PPI trials are often utilized in patients with typical symptoms, the presence of alarm symptoms, incomplete relief from empiric therapy, and atypical symptoms prompt evaluation using endoscopy, ambulatory reflux monitoring, and esophageal manometry (Figure 1).Isolated atypical symptoms in particular necessitate up-front testing rather than empiric treatment trials in view of high numbers needed to treat for a PPI response.19 A tailored approach based on symptom profile and response to therapy ensures accurate diagnosis and optimizes patient outcomes.
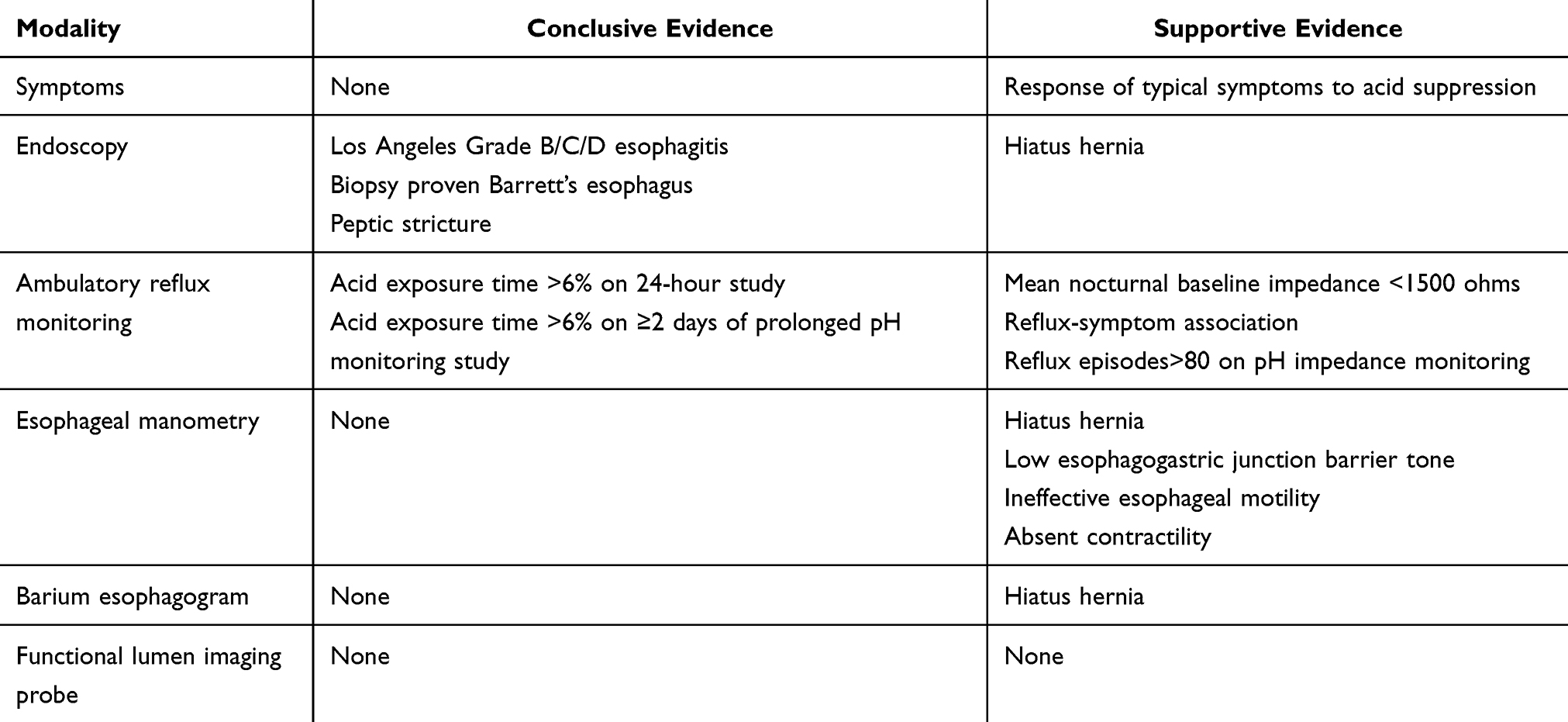 |
Table 2 Conclusive and Supportive Evidence of Gastro-Esophageal Reflux Disease |
Empiric Treatment Trials
Empiric PPI therapy is a pragmatic first step in patients manifesting typical GERD symptoms without alarm features (eg, dysphagia, weight loss, or gastrointestinal bleeding). On meta-analysis, a 1–2 week trial of twice daily PPI trial had a pooled sensitivity of 79% (95% CI 72–84%) and specificity of 45% (95% CI 40–49%) when compared to endoscopy and/or reflux monitoring.20 Up to two-thirds may report benefit from a 4- to 8-week trial of once-daily PPI before breakfast.21 If response is suboptimal, the dose can be increased to twice daily, the agent can be switched to a more potent PPI,22 or replaced with a potassium competitive acid blocker (PCAB).23 The 10–25% placebo effect and overlap with esophageal hypervigilance can confound the interpretation of treatment response.10,24
The likelihood of symptom response is significantly lower in patients with LPS such as chronic cough and hoarseness, with numbers needed to treat ranging from 5 to 10 to as high as 80 in randomized controlled trials.19,25 Since atypical symptoms are less likely to be directly related to reflux, up-front objective testing to identify or rule out reflux disease can be more cost-effective in guiding management.12,26
Endoscopy
A high-quality upper endoscopy has high specificity for objective evidence of GERD, but sensitivity is low since only a third of treatment naïve patients will manifest endoscopic abnormalities.27,28 An upper endoscopy is indicated in patients with alarm symptoms, and when symptoms do not respond or worsen while on acid suppression.29 In patients with no prior objective GERD evidence, termed “unproven GERD”, upper endoscopy serves as the first step in diagnostic evaluation, where conclusive GERD evidence consists of esophagitis graded Los Angeles (LA) grade B or higher, biopsy proven Barrett’s esophagus, or peptic stricture8 (Figure 1). In unproven GERD, upper endoscopy is best performed after withholding acid suppression to increase diagnostic yield of erosive esophagitis and eosinophilic esophagitis.21
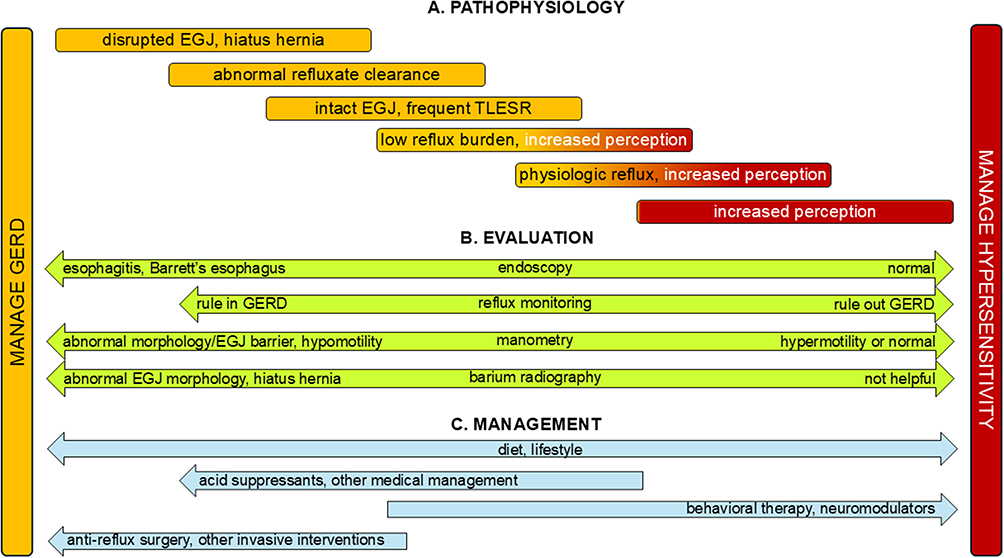 |
Figure 1 The spectrum of GERD pathophysiology, evaluation and management. (A). Pathophysiology. At the severe end of the GERD spectrum, the esophagogastric junction (EGJ) barrier can be disrupted, and a hiatus hernia could be present. Abnormal esophageal clearance from esophageal hypomotility can prolong esophageal reflux exposure. There is a significant overlap with increased esophageal symptom perception when the EGJ is intact, and esophageal hypersensitivity can coexist, with or without pathologic acid exposure. Symptoms identical to reflux can be seen with esophageal hypersensitivity alone in esophageal disorders of gut-brain interaction (E-DGBI).(B). Evaluation. The likelihood of abnormalities on endoscopy and reflux monitoring are higher in the context of EGJ disruption, when hiatus hernia, erosive esophagitis, Barrett’s esophagus and abnormal reflux burden are more likely. Esophageal tests are often normal in E-DGBI. While esophageal manometry can demonstrate hypomotility in advanced GERD phenotypes, manometry is typically not utilized to diagnose GERD. Reflux demonstrated on barium esophagography is not adequate for a GERD diagnosis, although finding EGJ disruption and a hiatus hernia can provide supportive data.(C). Management. The need for invasive management with antireflux surgery and endoscopic GERD management options is higher when there is EGJ disruption and when reflux burden is high. Medical management with acid suppression and adjunctive approaches may suffice when EGJ disruption is limited or absent. Behavioral therapy and neuromodulators are utilized for E-DGBI and for overlap between esophageal hypersensitivity and GERD. Diet and lifestyle measures are recommended for all patients with esophageal symptoms, regardless of where they land on the GERD spectrum. |
Upper endoscopy can provide adjunctive evidence for GERD by identifying disruption of the esophagogastric junction (EGJ), and evidence against GERD by demonstrating features of esophageal outflow obstruction. The EGJ is optimally inspected both anterograde and during retroflexion after adequate gastric insufflation with air, and graded using the Hill and the American Foregut Society (AFS) grading systems.27 The esophageal lumen and EGJ can be inspected and scored on a 0–2 Likert scale for Content (none, liquids, solids), Anatomy (non-dilated, dilated, severely dilated), EGJ Resistance to endoscope passage (none, mild, severe) and Stasis changes (none, stasis changes, candida) to generate the CARS score.30 A CARS score ≥4 has 68% sensitivity and 99% specificity for esophageal outflow obstruction from achalasia spectrum disorders.
Additional diagnostic modalities can be paired with upper endoscopy to increase the diagnostic yield. If no esophagitis or LA grade A esophagitis is seen, a prolonged wireless pH monitoring probe can be placed at the index endoscopy for ambulatory reflux monitoring.8,21 High-definition white light endoscopy and narrow-band imaging (NBI) can augment visualization of minor reflux change and Barrett’s esophagus. Functional lumen imaging probe (FLIP) can evaluate EGJ distensibility and esophageal body secondary peristalsis, but does not provide GERD diagnosis; instead, this modality has highest value in either establishing normal esophageal motor function, or in diagnosing achalasia spectrum disorders, especially when combined with the CARS score.31 Mucosal devices to evaluate baseline impedance during index endoscopy continue to be studied.32
Ambulatory Reflux Monitoring
Ambulatory reflux monitoring is indicated in two specific situations: a) to diagnose or rule out GERD in patients with unproven GERD, when typical symptoms fail to improve on empiric acid suppression, or up-front in patients with isolated atypical symptoms (unproven GERD), and b) to diagnose or rule out refractory GERD in patients with proven GERD who fail to improve on optimized reflux management (proven GERD).8,33 The choice of monitoring method depends on symptom presentation, whether GERD is unproven or proven, and why the test is being performed.
In unproven GERD with typical reflux symptoms, prolonged wireless pH monitoring (ideally for 96 hours) off acid suppression is the preferred diagnostic tool since this can be placed at index endoscopy if no conclusive GERD evidence is found.8,21 Wireless pH monitoring may also be appropriate in LPS associated with typical symptoms.12 Wireless pH monitoring overcomes day-to-day variability in acid exposure but only measures acid reflux episodes with a single recording site.34 Catheter-based pH impedance monitoring can detect both acidic and weakly/non-acidic reflux episodes, height of reflux migration proximally, and air containing esophageal events such as air swallowing and belching, but is performed unsedated, and requires high-resolution manometry (HRM) for accurate probe positioning. Importantly, pH impedance monitoring can also measure esophageal baseline impedance, which is a longitudinal marker of reflux related mucosal damage.34 However, wireless monitoring is better tolerated by patients compared to catheter-based systems.
Patients with proven GERD with persistent symptoms despite optimized PPI therapy benefit from catheter-based pH-impedance monitoring on therapy, where abnormal reflux metrics indicate refractory GERD that may benefit from escalation to PCAB or to invasive surgical options.8,35 Conversely, normal metrics indicate controlled GERD. On-therapy pH impedance monitoring in unproven GERD may identify refractory GERD, but does not discriminate between no GERD and controlled GERD; thus on-therapy testing of this kind is limited to proven GERD with persisting symptoms.8
The Lyon Consensus 2.0 identifies acid exposure time (AET) as the key metric from ambulatory reflux monitoring that defines conclusive GERD off-therapy and refractory GERD on-therapy (Table 2).8 Adjunctive metrics of varying importance include mean nocturnal baseline impedance (MNBI) and total reflux episodes from pH impedance monitoring, as well as reflux symptom association (RSA) from either wireless pH monitoring or pH impedance monitoring.8 The Lyon Score, designed from the Lyon Consensus 2.0 metrics, segregates esophageal symptom phenotypes, predicts response from antireflux management with better performance characteristics than the individual metrics that make up the score.36
Esophageal Manometry
Esophageal manometry is often normal in GERD, but hypomotility patterns such as ineffective esophageal motility (IEM) and absent contractility may be seen in reflux disease.37,38 Standard HRM cannot be used to diagnose GERD, but is important in ruling out achalasia spectrum disorders in PPI non-response and prior to antireflux surgery (ARS).39,40 Additionally, HRM is useful in characterizing EGJ tone and morphology. The Milan score, derived from HRM, utilizes esophageal hypomotility, EGJ barrier tone, EGJ morphology and response to the straight leg raise (SLR) maneuver, quantifies EGJ dysfunction and correlates with abnormal reflux burden in predicting response to GERD management, particularly ARS.41
Other Tests
Barium studies characterize esophageal and EGJ anatomy and morphology and can demonstrate hiatus hernias and structural abnormalities resulting from reflux, especially in patients with dysphagia. However, reflux visualized on a barium study does not predict abnormal reflux burden, and lack of reflux on a barium study does not rule out pathologic GERD.42 Therefore, barium esophagography is not a substitute for ambulatory reflux monitoring in the diagnosis of objective GERD.42,43
Identification of esophageal outflow obstruction and achalasia can be optimized using FLIP, but FLIP evaluation of EGJ barrier function in GERD does not discriminate symptomatic GERD from controls.44,45 Therefore, FLIP does not have a role in the diagnosis of GERD or in deciding need for antireflux surgery.46
Salivary pepsin assays have been studied as non-invasive tools for the diagnosis of GERD, but have variable performance characteristics, and are not currently recommended for routine clinical use.47–49 Scintigraphy has been used in research for evaluating esophageal transit but is not useful as a clinical tool for GERD diagnosis.
Differential Diagnosis
Several conditions can mimic GERD symptoms and need to be distinguished using appropriate diagnostic tests.
Eosinophilic Esophagitis
EoE, a chronic immune-mediated disorder with esophageal mucosal eosinophilia, can manifest chest pain, heartburn, dysphagia and food impaction.50 Endoscopy can reveal circumferential rings, longitudinal furrows, luminal narrowing and white exudates, but endoscopy can also be visually normal. Esophageal biopsies with ≥15 eosinophils per high-power field makes the diagnosis of EoE after exclusion of other causes of eosinophilia.51 EoE may respond to acid suppression, therefore diagnostic yield can be higher if endoscopy is performed after withholding acid suppression for 2–4 weeks when the diagnosis is uncertain. Other treatment strategies include topical budesonide, dietary exclusion of food allergens, and biologic therapy targeting the immune cascade mediated by interleukin 4 and interleukin 13.51
Achalasia Spectrum Disorders
The primary pathophysiologic abnormality in achalasia is abnormal esophageal inhibitory function resulting in incomplete LES relaxation and abnormal or absent esophageal body peristalsis.52 Patients with achalasia can have chest pain, and along with regurgitation, this can be misidentified as GERD. In fact, achalasia spectrum disorders are identified on HRM in 1–2.5% of patients referred for ARS.39 Achalasia can also be diagnosed in patients with dysphagia and absent contractility on HRM, especially in the absence of a hiatus hernia.53 Careful evaluation, including use of adjunctive tests such as a timed upright barium esophagram and FLIP, can ensure that achalasia is identified when patients with esophageal symptoms do not respond to acid suppressive therapy,54 since achalasia is managed very differently compared to GERD.
Supragastric Belching and Rumination
Supragastric belching and rumination syndrome are behavioral disorders that can overlap with GERD with symptoms such as regurgitation and belching. Air is involuntarily injected or sucked into the esophagus followed by rapid expulsion with often loud and repetitive belches in supragastric belching.18 The characteristic presentation of rumination syndrome consists of effortless regurgitation of recently ingested food, often with re-chewing or re-swallowing.55 Both conditions can occur in isolation, or in conjunction with GERD, and the diagnosis can be confirmed using pH-impedance monitoring and/or HRM with post prandial monitoring in patients with characteristic symptoms.56 Management includes behavioral interventions and treatment of underlying affective disorders.57
Esophageal Disorders of Gut-Brain Interaction
Several esophageal disorders of gut-brain interaction (E-DGBI), also called functional esophageal disorders, have identical symptoms as GERD.58 Functional heartburn and functional chest pain present with troublesome esophageal symptoms that do not respond to acid suppression and have normal endoscopy and normal esophageal reflux burden on ambulatory reflux monitoring. Reflux hypersensitivity presents with the same symptoms of heartburn and chest pain, but there is reflux-symptom correlation indicating esophageal hypersensitivity to reflux events.58 Increased esophageal symptom perception, anxiety and esophageal hypervigilance can participate in E-DGBI, and can also overlap with conclusive GERD.24 Management consists of neuromodulators and behavioral therapy, and acid suppression is continued only if there is clear clinical benefit (Figure 1).
Management Of Gastroesophageal Reflux Disease
Management options in GERD range from lifestyle and behavioral modifications, to acid suppression and adjunctive pharmacotherapy, to permanent augmentation of the EGJ using endoscopic and surgical techniques (Figure 1). Tailoring management to the individual patient allows personalization of treatment taking into consideration symptom severity, pathophysiology, patient preferences, and available local expertise.
Lifestyle And Dietary Modifications
Simple lifestyle changes consist of eating smaller meals, not lying down within 2–3 hours of eating, and sleeping with the head end of the bed raised.59 Sleeping in the left lateral position is associated with less supine reflux compared to the right lateral position, and electronic devices have been developed to alert patients when they turn on their right side.60 If dietary triggers such as spicy foods, citrus fruits, caffeine, chocolate, carbonated beverages, and fatty or fried meals bring on symptoms, these can be avoided.61 Stopping smoking and excessive alcohol consumption are additional lifestyle modifications that can be helpful in reducing GERD symptoms.
Obesity is an important risk factor for GERD, and GERD prevalence is higher in obese individuals with an odds ratio of 1.73 (95% confidence intervals 1.46–2.06) compared to those without obesity.3 Weight loss can reduce intrabdominal pressure and can result in lower esophageal acid burden. Even modest reduction of 5–10% of excess body weight can improve GERD symptoms and reduce the need for pharmacologic GERD therapy.62
Acid Suppression Therapy
Pharmacologic therapy with acid suppressive agents is an important component of GERD management, not just for symptom control, but also for healing of erosive esophagitis and maintenance of healing (Figure 1).
Proton Pump Inhibitors
PPIs irreversibly inhibit the gastric H+/K+ ATPase enzyme to reduce gastric acid secretion and have remained first-line agents for GERD management over the past three decades.19,63 For optimal efficacy, PPIs are administered 30–45 minutes before the first meal of the day, and similarly before the evening meal for twice daily dosing, to coincide with activation of proton pumps by the meal. PPIs have demonstrable efficacy in healing erosive esophagitis and maintaining healing in >80% of patients in meta-analysis of randomized controlled trials.64 PPIs prevent complications such as peptic strictures and progression of Barrett’s esophagus. PPIs are also effective in alleviating typical GERD symptoms,19 especially in confirmed GERD,65 with long-term efficacy matching that from laparoscopic antireflux surgery (ARS).66
Although long-term PPI use has been linked to several potential risks, only an increased risk of gastrointestinal infections (eg, Clostridioides difficile) has been conclusively demonstrated in a large prospective study comparing PPI use with placebo in the rivaroxaban vs aspirin trial over >53,000 patient-years of follow-up.67 When used for appropriate indications, PPI benefits far outweigh risks.63 However, PPI continue to be prescribed for inconsistent indications, and careful scrutiny of the reason why a PPI is prescribed is important in determining need for long-term use.21
Histamine-2 Receptor Antagonists (H2RAs)
H2RAs, such as ranitidine and famotidine block histamine-mediated acid secretion in the stomach and are generally less potent than PPIs.64 These agents are alternatives for patients with mild GERD symptoms, especially as a step-down approach when symptoms improve on PPI.68 H2RAs have been studied as adjunctive bedtime options to control night-time GERD symptoms for nocturnal acid breakthrough.69 However, these medications may lose efficacy over time due to tachyphylaxis.70 H2RAs are often used as rescue therapy for breakthrough symptoms and pre-emptively prior to meals that could provoke heartburn.
Potassium-Competitive Acid Blockers (PCABs)
PCABs competitively and reversibly block the potassium binding site of the H+/K+ ATPase enzyme on the gastric parietal cell and thus can dissociate from inactivated proton pumps to block additional pumps.71,72 They also do not require to be administered before meals and can block unstimulated proton pumps. Thus, PCABs such as vonoprazan, tegoprazan and fexuprazan offer rapid and sustained acid inhibition, including control of nocturnal acid breakthrough.72 PCABs have been demonstrated to have rates of healing of advanced grade esophagitis significantly higher than with PPIs.73 These agents rapidly control typical GERD symptoms more often than placebo.23,74 Thus, PCABs have an important role in both symptom control and healing of advanced grade esophagitis, and have been elevated to first-line use in GERD as an alternative to PPIs in some regions of the world.75
Adjunctive Therapies
Adjunctive therapies can target specific mechanisms in patients with breakthrough symptoms or persistent symptoms in the context of GERD.
Antacids, Alginates and Mucosal Protective Agents
Antacids neutralize acid in the esophagus and stomach, providing short-term GERD symptom relief.76 Alginates are derived from seaweed and form a physical barrier at the interface between gastric contents and the esophagus. They also coat the mucosa of the esophagus. Alginates, either by themselves or in combination with antacids, used as needed or scheduled, are particularly effective for postprandial and nocturnal symptoms.77 Sucralfate, a mucosal protective agent, binds to eroded mucosa and can be used to promote healing of erosive esophagitis.78 This agent has also been used in pregnant women with reflux symptoms, since it is not absorbed.
Baclofen
Baclofen is a gamma-aminobutyric acid (GABA-B) agonist that reduces frequency of TLESRs and thereby reduces reflux events and esophageal acid exposure.79,80 This agent may be particularly effective in regurgitation-predominant reflux, and in belching-related symptoms. Baclofen use is limited by side effects such as dizziness, fatigue, and sleepiness.
Prokinetics
Although prokinetics (eg metoclopramide, domperidone) can augment esophageal peristalsis, adding a prokinetic only modestly improves symptoms, without improvement in healing or esophageal peristalsis, and potential increase in side effects, although gastric emptying could improve in patients with concurrent gastroparesis.81,82
Diaphragmatic Breathing
By consciously engaging the diaphragm during breathing, frequency of reflux episodes can be reduced by strengthening the diaphragmatic component of the anti-reflux barrier, thereby reducing the frequency of reflux episodes.83 Diaphragmatic breathing can be recommended as an adjunct in patients with post-prandial reflux, belching symptoms, and rumination syndrome.21
Cognitive Behavioral Therapy (CBT) and Gut Directed Hypnotherapy
Hypervigilance and symptom-specific anxiety are prevalent in patients with persisting esophageal symptoms despite seemingly adequate GERD therapy.21,84,85 Behavioral interventions, including CBT and hypnotherapy, have shown promise in patients with symptoms exacerbated by stress, anxiety, or esophageal hypervigilance.86 These therapies aim to reduce the psychological burden of GERD and improve coping mechanisms, leading to better symptom control and quality of life.87
Surgical and Endoscopic Interventions
Invasive management options for GERD consist of surgical and endoscopic interventions that aim to restore EGJ integrity and reduce reflux episodes (Figure 1). These are options for patients with objective refractory GERD despite optimized medical management, for patients with well-characterized GERD who wish to avoid long-term medication use, and for patients with significant disruption of the anti-reflux barrier with large hiatus hernias.88
Laparoscopic Fundoplication
The standard invasive anti-reflux procedure is laparoscopic fundoplication, which consists of repair of the diaphragmatic hiatus, restoration of the intra-abdominal location of the LES, and wrapping of the gastric fundus around the LES, either completely (Nissen fundoplication) or partially (Toupet or Dor fundoplication).19 Long-term symptom control achieved in 80–90% of patients, although many patients resume medical management with a PPI after varying periods of time.89 New symptoms including dysphagia, gas-bloat, dumping syndrome and symptoms related to delayed gastric emptying are potential complications that patients need to be aware.
Transoral Incisionless Fundoplication (TIF)
Reinforcement of the EGJ similar to that achieved with fundoplication can be achieved with TIF, a minimally invasive endoscopic alternative to traditional fundoplication. TIF is performed using a specialized device inserted through the mouth, without the need for external incisions. TIF is particularly suitable for patients with regurgitation-predominant GERD without a large hiatus hernia who prefer a less invasive option.90 When a hiatus hernia is present, a modification of the procedure that involves laparoscopic hiatus repair (C-TIF) has been investigated as an alternative to fundoplication. Short- and intermediate-term efficacy has been demonstrated.91
Magnetic Sphincter Augmentation (MSA)
A bracelet of magnetic titanium beads implanted around the LES enhances sphincter competency while allowing physiological function and swallow induced esophageal emptying, termed MSA.92 MSA is an option for control of regurgitation-predominant symptoms while preserving the ability to belch and vomit, and a lower risk of gas-bloat syndrome compared to laparoscopic fundoplication.93 Long-term studies have demonstrated good symptom control and high patient satisfaction scores with MSA, although dysphagia and device erosion into the esophagus are risks necessitating explant of the device.94
Roux-En-Y Gastric Bypass
When GERD is diagnosed in obese individuals, a Roux-en-Y gastric bypass can control reflux symptoms while also facilitating significant weight loss.19 In contrast, a sleeve gastrectomy can induce de novo GERD symptoms or exacerbate existing symptoms, and is not recommended in patients with GERD.95 Roux-en-Y gastric bypass is considered the anti-reflux procedure of choice in obese patients with GERD, as it addresses both body weight and GERD simultaneously.96,97
Complications
Complications can arise from chronic exposure of the esophageal mucosa to gastric acid and other refluxate components, as well as from the effects of reflux on adjacent organs (Table 2).
Esophageal Strictures
Chronic inflammation from repeated acid exposure can lead to narrowing of the esophageal lumen from fibrosis and scarring to form strictures.98 The primary manifestation is intermittent solid food dysphagia. Strictures can be identified during endoscopy, when therapeutic dilation can be performed using balloon or bougie dilators. While symptoms improve with dilation, strictures can recur, and repeat dilation is often needed at varying intervals.99 Continuous acid suppression can help reduce recurrence. Steroid injection into rents created by dilation can increase interval to symptom recurrence in refractory strictures.99
Barrett’s Esophagus
In predisposed individuals, the normal esophageal squamous epithelium may be replaced with metaplastic columnar epithelium in long standing reflux disease, termed Barrett’s esophagus. While this is a protective response to chronic acid exposure and may reduce reflux symptom perception, it confers an increased risk of esophageal adenocarcinoma. The diagnosis is made during endoscopic screening, which is indicated in high-risk populations, including long-standing GERD (≥5 years), male gender, age >50 years, obesity, and a family history of Barrett’s or esophageal cancer.100 Barrett’s esophagus appears as tongues or circumferential segments of salmon colored mucosa in the distal esophagus, and histopathology demonstrating intestinal metaplasia with goblet cells is required to confirm the diagnosis. Surveillance biopsies are recommended every 3–5 years to detect dysplasia or early malignancy, at intervals determined by the degree of dysplasia.100 Patients with dysplasia can be managed with endoscopic therapies such as radiofrequency ablation and/or endoscopic mucosal resection, with high rates of success in eradicating dysplasia and preventing progression to adenocarcinoma when combined with continued surveillance.
Esophageal Adenocarcinoma
Esophageal adenocarcinoma typically arises from dysplastic changes within Barrett’s esophagus, although many patients with esophageal adenocarcinoma may not have had a prior GERD or Barrett’s esophagus diagnosis.101 The risk of progression from Barrett’s esophagus to adenocarcinoma is approximately 0.1–0.5% per year, underscoring the importance of maintenance GERD management and regular surveillance in at-risk individuals.100 Early detection and advances in endoscopic therapies have improved outcomes for patients with high-grade dysplasia or early-stage cancer.
Pulmonary Aspiration Syndromes
Chronic aspiration of gastric contents into the airways can lead to a spectrum of pulmonary complications, including recurrent pneumonia, bronchitis, and bronchiectasis.102 The risk of aspiration syndromes may be higher in patients with nocturnal reflux, especially when protective reflexes are impaired, such as the elderly or patients with neurological disorders. Symptoms may include chronic cough, wheezing, and recurrent respiratory infections. Diagnosis can be challenging, as the mere presence of coexistent GERD may not imply causality; furthermore, aspiration can occur silently without overt symptoms. Ambulatory pH-impedance monitoring and bronchoscopy with bronchoalveolar lavage can provide evidence for pulmonary aspiration of gastric refluxate.102,103 Patients with recurrent aspiration benefit from gravitational measures including elevating the head of the bed and avoiding late-night meals and using prokinetic agents to improve gastric emptying when gastroparesis coexists.102
Idiopathic Pulmonary Fibrosis
A potential link between chronic GERD and idiopathic pulmonary fibrosis (IPF), a progressive and often fatal lung disease characterized by fibrosis of the pulmonary parenchyma.102 Microaspiration of gastric contents may trigger an inflammatory response in the lungs, leading to fibrosis in predisposed individuals.104 There is limited evidence suggesting that aggressive acid suppression or anti-reflux surgery may slow disease progression. Further research is needed to establish a definitive causal relationship and guide management. Aggressive acid suppression and lifestyle modifications are recommended, and in select cases, anti-reflux surgery may be reasonable.102
Asthma
While GERD is common in asthmatics, causality is difficult to establish despite as many as 75% of asthmatics reporting reflux symptoms. The relationship between GERD and asthma is bidirectional: reflux can trigger bronchospasm through vagal reflexes or direct aspiration, while asthma can exacerbate reflux by increasing intra-abdominal pressure.105 Additionally, bronchodilators can reduce LES tone and promote reflux. Patients with difficult-to-control asthma need to be evaluated for GERD, as focused reflux management may improve respiratory symptoms. However, the response to acid suppression therapy is variable, and not all patients experience significant improvement in asthma control.106 In severe cases with well-documented GERD, surgical interventions such as fundoplication may be necessary.
Prognosis
The overall prognosis for patients with GERD is generally good, particularly when the condition is diagnosed early and managed effectively. With appropriate medical treatment, most patients achieve significant symptom relief and improved quality of life. ARS offers comparable long-term outcomes and provides durable symptom improvement in well-selected patients.
When symptoms persist despite adequate management, GERD can be refractory to medical management, especially when the antireflux barrier is disrupted. Symptoms may also persist from overlapping mechanisms such as reflux hypersensitivity or functional heartburn, which require alternative management strategies. Esophageal physiologic testing can help identify the mechanism for refractoriness of symptoms in previously proven GERD, which can lead to focused management ranging from escalated medical management to ARS. Overall, with timely and individualized management, the prognosis for GERD remains favorable even in refractory GERD.
Disclosure
CPG reports consulting for Medtronic, Alimentiv, Braintree, Phathom; speaker for Carnot. The authors report no other conflicts of interest in this work.
References
1. Fass R. Gastroesophageal reflux disease. N Engl J Med. 2022;387:1207–1216. doi:10.1056/NEJMcp2114026
2. El-Serag HB, Sweet S, Winchester CC, et al. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014;63:871–880. doi:10.1136/gutjnl-2012-304269
3. Eusebi LH, Ratnakumaran R, Yuan Y, et al. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut. 2018;67:430–440. doi:10.1136/gutjnl-2016-313589
4. Shaheen NJ, Hansen RA, Morgan DR, et al. The burden of gastrointestinal and liver diseases, 2006. Am J Gastroenterol. 2006;101:2128–2138. doi:10.1111/j.1572-0241.2006.00723.x
5. Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–1920. doi:10.1111/j.1572-0241.2006.00630.x
6. Dent J, Vakil N, Jones R, et al. Accuracy of the diagnosis of GORD by questionnaire, physicians and a trial of proton pump inhibitor treatment: the diamond study. Gut. 2010;59:714–721. doi:10.1136/gut.2009.200063
7. Bytzer P, Jones R, Vakil N, et al. Limited ability of the proton-pump inhibitor test to identify patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2012;10:1360–1366. doi:10.1016/j.cgh.2012.06.030
8. Gyawali CP, Yadlapati R, Fass R, et al. Updates to the modern diagnosis of GERD: Lyon consensus 2.0. Gut. 2024;73:361–371. doi:10.1136/gutjnl-2023-330616
9. Gyawali CP, Kahrilas PJ, Savarino E, et al. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018;67:1351–1362. doi:10.1136/gutjnl-2017-314722
10. Cremonini F, Ziogas DC, Chang HY, et al. Meta-analysis: the effects of placebo treatment on gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2010;32:29–42. doi:10.1111/j.1365-2036.2010.04315.x
11. Nakagawa K, Sawada A, Hoshikawa Y, et al. Persistent postprandial regurgitation vs rumination in patients with refractory gastroesophageal reflux disease symptoms: identification of a distinct rumination pattern using ambulatory impedance-pH monitoring. Am J Gastroenterol. 2019;114:1248–1255. doi:10.14309/ajg.0000000000000295
12. Yadlapati R, Weissbrod P, Walsh E, et al. The san diego consensus for laryngopharyngeal symptoms and laryngopharyngeal reflux disease. Am J Gastroenterol. 2025. doi:10.14309/ajg.0000000000003482
13. Zheng Z, Luo Y, Li J, et al. Randomised trials of proton pump inhibitors for gastro-oesophageal reflux disease in patients with asthma: an updated systematic review and meta-analysis. BMJ Open. 2021;11:e043860. doi:10.1136/bmjopen-2020-043860
14. Zerbib F, Rommel N, Pandolfino J, et al. ESNM/anms review. diagnosis and management of globus sensation: a clinical challenge. Neurogastroenterol Motil. 2020;32:e13850. doi:10.1111/nmo.13850
15. Krause AJ, Kaizer AM, Carlson DA, et al. Validated clinical score to predict gastroesophageal reflux in patients with chronic laryngeal symptoms: cOuGH RefluX. Clin Gastroenterol Hepatol. 2024;22:1200–1209e1. doi:10.1016/j.cgh.2024.01.021
16. Pleyer C, Bittner H, Locke GR, et al. Overdiagnosis of gastro-esophageal reflux disease and underdiagnosis of functional dyspepsia in a USA community. Neurogastroenterol Motil. 2014;26:1163–1171. doi:10.1111/nmo.12377
17. Sawada A, Guzman M, Nikaki K, et al. Identification of different phenotypes of esophageal reflux hypersensitivity and implications for treatment. Clin Gastroenterol Hepatol. 2021;19:690–698e2. doi:10.1016/j.cgh.2020.03.063
18. Kessing BF, Bredenoord AJ, Aj S. The pathophysiology, diagnosis and treatment of excessive belching symptoms. Am J Gastroenterol. 2014;109:1196–203). doi:10.1038/ajg.2014.165
19. Gyawali CP, Fass R. Management of gastroesophageal reflux disease. Gastroenterology. 2018;154:302–318. doi:10.1053/j.gastro.2017.07.049
20. Ghoneim S, Wang J, El Hage Chehade N, et al. Diagnostic accuracy of the proton pump inhibitor test in gastroesophageal reflux disease and noncardiac chest pain: a systematic review and meta-analysis. J Clin Gastroenterol. 2023;57:380–388. doi:10.1097/MCG.0000000000001686
21. Yadlapati R, Gyawali CP, Pandolfino JE, et al. AGA clinical practice update on the personalized approach to the evaluation and management of GERD: expert review. Clin Gastroenterol Hepatol. 2022;20:984–994e1. doi:10.1016/j.cgh.2022.01.025
22. Graham DY, Tansel A. interchangeable use of proton pump inhibitors based on relative potency. Clin Gastroenterol Hepatol. 2018;16:800–808e7. doi:10.1016/j.cgh.2017.09.033
23. Laine L, Spechler S, Yadlapati R, et al. Vonoprazan is efficacious for treatment of heartburn in non-erosive reflux disease: a randomized trial. Clin Gastroenterol Hepatol. 2024;22:2211–2220e10. doi:10.1016/j.cgh.2024.05.004
24. Guadagnoli L, Yadlapati R, Taft T, et al. Esophageal hypervigilance is prevalent across gastroesophageal reflux disease presentations. Neurogastroenterol Motil. 2021;33:e14081. doi:10.1111/nmo.14081
25. Katzka DA, Pandolfino JE, Kahrilas PJ. Phenotypes of gastroesophageal reflux disease: where Rome, Lyon, and Montreal meet. Clin Gastroenterol Hepatol. 2020;18:767–776. doi:10.1016/j.cgh.2019.07.015
26. Carroll TL, Werner A, Nahikian K, et al. Rethinking the laryngopharyngeal reflux treatment algorithm: evaluating an alternate empiric dosing regimen and considering up-front, pH-impedance, and manometry testing to minimize cost in treating suspect laryngopharyngeal reflux disease. Laryngoscope. 2017;127(Suppl 6):S1–S13. doi:10.1002/lary.26806
27. Yadlapati R, Early D, Iyer PG, et al. Quality Indicators for Upper GI Endoscopy. Am J Gastroenterol. 2025;120:290–312. doi:10.14309/ajg.0000000000003252
28. Qumseya BJ, Bukannan A, Gendy S, et al. Systematic review and meta-analysis of prevalence and risk factors for Barrett’s esophagus. Gastrointest Endosc. 2019;90:707–717e1. doi:10.1016/j.gie.2019.05.030
29. Shaheen NJ, Weinberg DS, Denberg TD, et al. Upper endoscopy for gastroesophageal reflux disease: best practice advice from the clinical guidelines committee of the American College of Physicians. Ann Intern Med. 2012;157:808–816. doi:10.7326/0003-4819-157-11-201212040-00008
30. Ellison A, Peller M, Nguyen AD, et al. An endoscopic scoring system for achalasia: the CARS score. Gastrointest Endosc. 2024;100:417–428e1. doi:10.1016/j.gie.2024.02.020
31. Carlson DA, Li M, Fass O, et al. a combined endoscopy and functional lumen imaging probe panometry approach can expedite diagnosis of esophageal motility disorders. Gastrointest Endosc. 2025. doi:10.1016/j.gie.2025.03.1329
32. Patel DA, Higginbotham T, Slaughter JC, et al. Development and validation of a mucosal impedance contour analysis system to distinguish esophageal disorders. Gastroenterology. 2019;156:1617–1626e1. doi:10.1053/j.gastro.2019.01.253
33. Katz PO, Dunbar KB, Schnoll-Sussman FH, et al. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2022;117:27–56.
34. Sifrim D, Gyawali CP. Prolonged wireless pH monitoring or 24-hour catheter-based ph impedance monitoring: who, when, and why? Am J Gastroenterol. 2020;115:1150–1152. doi:10.14309/ajg.0000000000000648
35. Gyawali CP, Tutuian R, Zerbib F, et al. Value of pH impedance monitoring while on twice-daily proton pump inhibitor therapy to identify need for escalation of reflux management. Gastroenterology. 2021;161:1412–1422. doi:10.1053/j.gastro.2021.07.004
36. Gyawali CP, Marchetti L, Rogers BD, et al. the Lyon score: a novel reflux scoring system based on the Lyon consensus 2.0 that associates with treatment outcome from antireflux therapy. Am J Gastroenterol. 2025;120:1009–1018. doi:10.14309/ajg.0000000000003083
37. Rogers BD, Rengarajan A, Mauro A, et al. Fragmented and failed swallows on esophageal high-resolution manometry associate with abnormal reflux burden better than weak swallows. Neurogastroenterol Motil. 2019;e13736.
38. Gyawali CP, Zerbib F, Bhatia S, et al. Chicago Classification update (V4.0): technical review on diagnostic criteria for ineffective esophageal motility and absent contractility. Neurogastroenterol Motil. 2021;33:e14134. doi:10.1111/nmo.14134
39. Chan WW, Haroian LR, Gyawali CP. Value of preoperative esophageal function studies before laparoscopic antireflux surgery. Surg Endosc. 2011;25:2943–2949. doi:10.1007/s00464-011-1646-9
40. Salvador R, Pandolfino JE, Costantini M, et al. The role of high-resolution manometry before and following antireflux surgery: the padova consensus. Ann Surg. 2025;281:124–135. doi:10.1097/SLA.0000000000006297
41. Siboni S, Kristo I, Rogers BD, et al. Improving the diagnostic yield of high-resolution esophageal manometry for GERD: the “straight leg-raise. International Study.
42. Saleh CM, Smout AJ, Bredenoord AJ. The diagnosis of gastro-esophageal reflux disease cannot be made with barium esophagograms. Neurogastroenterol Motil. 2015;27:195–200. doi:10.1111/nmo.12457
43. Bhardwaj R, Davis TA, Franz A, et al. Reflux seen on a barium swallow is not a substitute for ambulatory reflux monitoring in symptomatic patients. J Clin Gastroenterol. 2025. doi:10.1097/MCG.0000000000002133
44. Kwiatek MA, Pandolfino JE, Hirano I, et al. Esophagogastric junction distensibility assessed with an endoscopic functional luminal imaging probe (EndoFLIP). Gastrointest Endosc. 2010;72:272–278. doi:10.1016/j.gie.2010.01.069
45. Tucker E, Sweis R, Anggiansah A, et al. Measurement of esophago-gastric junction cross-sectional area and distensibility by an endoluminal functional lumen imaging probe for the diagnosis of gastro-esophageal reflux disease. Neurogastroenterol Motil. 2013;25:904–910. doi:10.1111/nmo.12218
46. Nguyen AD, Carlson DA, Patel A, et al. AGA Clinical practice update: incorporating Functional Lumen Imaging Probe (FLIP) into clinical esophageal practice: expert review. Gastroenterology. 2025.
47. Hayat JO, Gabieta-Somnez S, Yazaki E, et al. Pepsin in saliva for the diagnosis of gastro-oesophageal reflux disease. Gut. 2015;64:373–380. doi:10.1136/gutjnl-2014-307049
48. Dy F, Amirault J, Mitchell PD, et al. Salivary pepsin lacks sensitivity as a diagnostic tool to evaluate extraesophageal reflux disease. J Pediatr. 2016;177:53–58. doi:10.1016/j.jpeds.2016.06.033
49. Yadlapati R, Adkins C, Jaiyeola DM, et al. Abilities of oropharyngeal ph tests and salivary pepsin analysis to discriminate between asymptomatic volunteers and subjects with symptoms of laryngeal irritation. Clin Gastroenterol Hepatol. 2016;14:535–542e2. doi:10.1016/j.cgh.2015.11.017
50. Dellon ES, Liacouras CA, Molina-Infante J, et al. Updated international consensus diagnostic criteria for eosinophilic esophagitis:
51. Dellon ES, Muir AB, Katzka DA, et al. ACG clinical guideline: diagnosis and management of eosinophilic esophagitis. Am J Gastroenterol. 2025;120:31–59.
52. Savarino E, Bhatia S, Roman S, et al. Achalasia. Nat Rev Dis Primers. 2022;8:28. doi:10.1038/s41572-022-00356-8
53. Patel P, Rogers BD, Rengarajan A, et al. Identification of achalasia within absent contractility phenotypes on high-resolution manometry: prevalence, predictive factors, and treatment outcome. Am J Gastroenterol. 2024.
54. Vaezi MF, Pandolfino JE, Yadlapati RH, et al. ACG clinical guidelines: diagnosis and management of achalasia. Am J Gastroenterol. 2020;115:1393–1411. doi:10.14309/ajg.0000000000000731
55. Kessing BF, Smout AJ, Bredenoord AJ. Current diagnosis and management of the rumination syndrome. J Clin Gastroenterol. 2014;48:478–483. doi:10.1097/MCG.0000000000000142
56. Zerbib F, Bredenoord AJ, Fass R, et al. ESNM/ANMS consensus paper: diagnosis and management of refractory gastro-esophageal reflux disease. Neurogastroenterol Motil. 2021;33:e14075. doi:10.1111/nmo.14075
57. Sawada A, Anastasi N, Green A, et al. Management of supragastric belching with cognitive behavioural therapy: factors determining success and follow-up outcomes at 6-12 months post-therapy. Aliment Pharmacol Ther. 2019;50:530–537. doi:10.1111/apt.15417
58. Aziz Q, Fass R, Gyawali CP, et al. Functional Esophageal Disorders. Gastroenterology. 2016;150:1368–1379. doi:10.1053/j.gastro.2016.02.012
59. Fujiwara Y, Machida A, Watanabe Y, et al. Association between dinner-to-bed time and gastro-esophageal reflux disease. Am J Gastroenterol. 2005;100:2633–2636. doi:10.1111/j.1572-0241.2005.00354.x
60. Schuitenmaker JM, Kuipers T, Oude Nijhuis RAB, et al. Sleep positional therapy for nocturnal gastroesophageal reflux: a double-blind, randomized, sham-controlled trial. Clin Gastroenterol Hepatol. 2022;20:2753–2762e2. doi:10.1016/j.cgh.2022.02.058
61. Fox M, Gyawali CP. Dietary factors involved in GERD management. Best Pract Res Clin Gastroenterol. 2023;62-63:101826.
62. Mehta RS, Nguyen LH, Ma W, et al. Association of diet and lifestyle with the risk of gastroesophageal reflux disease symptoms in us women. JAMA Intern Med. 2021;181:552–554. doi:10.1001/jamainternmed.2020.7238
63. Gyawali CP. Proton pump inhibitors in gastroesophageal reflux disease: friend or foe. Curr Gastroenterol Rep. 2017;19:46. doi:10.1007/s11894-017-0586-5
64. Chiba N, De Gara CJ, Wilkinson JM, et al. Speed of healing and symptom relief in grade II to IV gastroesophageal reflux disease: a meta-analysis. Gastroenterology. 1997;112:1798–1810. doi:10.1053/gast.1997.v112.pm9178669
65. Patel A, Sayuk GS, Gyawali CP. Parameters on esophageal pH-impedance monitoring that predict outcomes of patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2015;13:884–891. doi:10.1016/j.cgh.2014.08.029
66. Lundell L, Attwood S, Ell C, et al. Comparing laparoscopic antireflux surgery with esomeprazole in the management of patients with chronic gastro-oesophageal reflux disease: a 3-year interim analysis of the LOTUS trial. Gut. 2008;57:1207–1213. doi:10.1136/gut.2008.148833
67. Moayyedi P, Eikelboom JW, Bosch J, et al. Safety of proton pump inhibitors based on a large, multi-year, randomized trial of patients receiving rivaroxaban or aspirin. Gastroenterology. 2019;157:682–691e2. doi:10.1053/j.gastro.2019.05.056
68. Inadomi JM, Jamal R, Murata GH, et al. Step-down management of gastroesophageal reflux disease. Gastroenterology. 2001;121:1095–1100. doi:10.1053/gast.2001.28649
69. Mainie I, Tutuian R, Castell DO. Addition of a H2 receptor antagonist to PPI improves acid control and decreases nocturnal acid breakthrough. J Clin Gastroenterol. 2008;42:676–679. doi:10.1097/MCG.0b013e31814a4e5c
70. Fackler WK, Ours TM, Vaezi MF, et al. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology. 2002;122:625–632. doi:10.1053/gast.2002.31876
71. Scarpignato C, Hunt RH. Editorial: potassium-competitive acid blockers for acid-related diseases-tegoprazan, a new kid on the block. Aliment Pharmacol Ther. 2019;50:960–962. doi:10.1111/apt.15480
72. Spechler S, Kolb JM, Dunbar KB, et al. American foregut society white paper report on the use of potassium-competitive acid blockers in the treatment of gastroesophageal reflux disease. Foregut. 2025. doi:10.1177/26345161251325874
73. Laine L, DeVault K, Katz P, et al. Vonoprazan versus lansoprazole for healing and maintenance of healing of erosive esophagitis: a randomized trial. Gastroenterology. 2023;164:61–71. doi:10.1053/j.gastro.2022.09.041
74. Kim SH, Cho KB, Chun HJ, et al. Randomised clinical trial: comparison of tegoprazan and placebo in non-erosive reflux disease. Aliment Pharmacol Ther. 2021;54:402–411. doi:10.1111/apt.16477
75. Jung HK, Tae CH, Song KH, et al. 2020 Seoul consensus on the diagnosis and management of gastroesophageal reflux disease. J Neurogastroenterol Motil. 2021;27:453–481. doi:10.5056/jnm21077
76. Weberg R, Berstad A. Symptomatic effect of a low-dose antacid regimen in reflux oesophagitis. Scand J Gastroenterol. 1989;24:401–406. doi:10.3109/00365528909093066
77. De Ruigh A, Roman S, Chen J, et al. Gaviscon Double Action Liquid (antacid & alginate) is more effective than antacid in controlling post-prandial oesophageal acid exposure in GERD patients: a double-blind crossover study. Aliment Pharmacol Ther. 2014;40:531–537. doi:10.1111/apt.12857
78. Simon B, Ravelli GP, Goffin H. Sucralfate gel versus placebo in patients with non-erosive gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 1996;10:441–446. doi:10.1111/j.0953-0673.1996.00441.x
79. Vela MF, Tutuian R, Katz PO, et al. Baclofen decreases acid and non-acid post-prandial gastro-oesophageal reflux measured by combined multichannel intraluminal impedance and pH. Aliment Pharmacol Ther. 2003;17:243–251. doi:10.1046/j.1365-2036.2003.01394.x
80. Blondeau K, Boecxstaens V, Rommel N, et al. Baclofen improves symptoms and reduces postprandial flow events in patients with rumination and supragastric belching. Clin Gastroenterol Hepatol. 2012;10:379–384. doi:10.1016/j.cgh.2011.10.042
81. Ren LH, Chen WX, Qian LJ, et al. Addition of prokinetics to PPI therapy in gastroesophageal reflux disease: a meta-analysis. World J Gastroenterol. 2014;20:2412–2419. doi:10.3748/wjg.v20.i9.2412
82. Shibli F, Kitayama Y, Fass R. Novel therapies for gastroesophageal reflux disease: beyond proton pump inhibitors. Curr Gastroenterol Rep. 2020;22:16. doi:10.1007/s11894-020-0753-y
83. Halland M, Bharucha AE, Crowell MD, et al. Effects of diaphragmatic breathing on the pathophysiology and treatment of upright gastroesophageal reflux: a randomized controlled trial. Am J Gastroenterol. 2021;116:86–94. doi:10.14309/ajg.0000000000000913
84. Riehl ME, Keefer L. Hypnotherapy for esophageal disorders. Am J Clin Hypn. 2015;58:22–33. doi:10.1080/00029157.2015.1025355
85. Luo Y, Keefer L. The Clinical value of brain-gut behavioral therapies for functional esophageal disorders and symptoms. Neurogastroenterol Motil. 2022;
86. Hurtte E, Rogers BD, Richards C, et al. The clinical value of psycho-gastroenterological interventions for functional esophageal symptoms. Neurogastroenterol Motil. 2022;34:e14315. doi:10.1111/nmo.14315
87. Guadagnoli L, Yadlapati R, Pandolfino J, et al. Behavioral therapy for functional heartburn: recommendation statements. Clin Gastroenterol Hepatol. 2024;22:1709–1718e3. doi:10.1016/j.cgh.2024.03.004
88. Pauwels A, Boecxstaens V, Andrews CN, et al. How to select patients for antireflux surgery? The ICARUS guidelines (international consensus regarding preoperative examinations and clinical characteristics assessment to select adult patients for antireflux surgery). Gut. 2019. doi:10.1136/gutjnl-2019-318260
89. Galmiche JP, Hatlebakk J, Attwood S, et al. Laparoscopic antireflux surgery vs esomeprazole treatment for chronic GERD: the LOTUS randomized clinical trial. JAMA. 2011;305:1969–1977. doi:10.1001/jama.2011.626
90. Hunter JG, Kahrilas PJ, Bell RC, et al. Efficacy of transoral fundoplication vs omeprazole for treatment of regurgitation in a randomized controlled trial. Gastroenterology. 2015;148:324–333e5. doi:10.1053/j.gastro.2014.10.009
91. ASoP C, Desai M, Ruan W, et al. American Society for Gastrointestinal Endoscopy guideline on the diagnosis and management of GERD: summary and recommendations. Gastrointest Endosc. 2025;101:267–284. doi:10.1016/j.gie.2024.10.008
92. Bell R, Lipham J, Louie B, et al. Laparoscopic magnetic sphincter augmentation versus double-dose proton pump inhibitors for management of moderate-to-severe regurgitation in GERD: a randomized controlled trial. Gastrointest Endosc. 2019;89:14–22e1. doi:10.1016/j.gie.2018.07.007
93. Bell RCW. Management of regurgitation in patients with gastroesophageal reflux disease. Curr Opin Gastroenterol. 2020;36:336–343. doi:10.1097/MOG.0000000000000649
94. Patel A, Gyawali CP. The role of magnetic sphincter augmentation in the gastroesophageal reflux disease treatment pathway: the gastroenterology perspective. Dis Esophagus. 2023;36. doi:10.1093/dote/doad005
95. Patel P, SHobbs P, Rogers BD, et al. Reflux symptoms increase following sleeve gastrectomy despite triage of symptomatic patients to roux-en-y gastric bypass. J Clin Gastroenterol. 2022.
96. Madalosso CA, Gurski RR, Callegari-Jacques SM, et al. The impact of gastric bypass on gastroesophageal reflux disease in morbidly obese patients. Ann Surg. 2016;263:110–116. doi:10.1097/SLA.0000000000001139
97. Kim M, Navarro F, Eruchalu CN, et al. Minimally invasive Roux-en-Y gastric bypass for fundoplication failure offers excellent gastroesophageal reflux control. Am Surg. 2014;80:696–703. doi:10.1177/000313481408000726
98. Ruigomez A, Garcia Rodriguez LA, Wallander MA, et al. Esophageal stricture: incidence, treatment patterns, and recurrence rate. Am J Gastroenterol. 2006;101:2685–2692. doi:10.1111/j.1572-0241.2006.00828.x
99. Sami SS, Haboubi HN, Ang Y, et al. UK guidelines on oesophageal dilatation in clinical practice. Gut. 2018;67:1000–1023. doi:10.1136/gutjnl-2017-315414
100. Shaheen NJ, Falk GW, Iyer PG, et al. Diagnosis and management of barrett’s esophagus: an updated ACG guideline. Am J Gastroenterol. 2022;117:559–587. doi:10.14309/ajg.0000000000001680
101. Sharma P. Barrett esophagus: a review. JAMA. 2022;328:663–671. doi:10.1001/jama.2022.13298
102. Chan WW, Sharma N, Gyawali CP. The role of gastroesophageal reflux in airway inflammation. Am J Gastroenterol. 2025;120:60–64. doi:10.14309/ajg.0000000000003205
103. Rangan V, Borges LF, Lo WK, et al. Novel advanced impedance metrics on impedance-ph testing predict lung function decline in idiopathic pulmonary fibrosis. Am J Gastroenterol. 2022;117:405–412. doi:10.14309/ajg.0000000000001577
104. Zhou JC, Gavini S, Chan WW, et al. Relationship between esophageal disease and pulmonary fibrosis. Dig Dis Sci. 2023;68:1096–1105. doi:10.1007/s10620-023-07908-2
105. Okwara NC, Chan WW. Sorting out the relationship between esophageal and pulmonary disease. Gastroenterol Clin North Am. 2021;50:919–934. doi:10.1016/j.gtc.2021.08.006
106. Chan WW, Chiou E, Obstein KL, et al. The efficacy of proton pump inhibitors for the treatment of asthma in adults: a meta-analysis. Arch Intern Med. 2011;171:620–629. doi:10.1001/archinternmed.2011.116
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.