")
Back to Journals » Patient Preference and Adherence » Volume 19
Exploring the Perspectives of Lung Cancer Chemotherapy Patients on Self-Management: A Qualitative Interview Study Using the COM-B Model
Authors Jia R , Xie N , Li Y, Zhang Y
Received 19 February 2025
Accepted for publication 28 June 2025
Published 12 July 2025 Volume 2025:19 Pages 1991—2002
DOI https://doi.org/10.2147/PPA.S522066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ruimei Jia,1,* Nina Xie,1,* Yue Li,2 Yu Zhang2
1School of Nursing, Shaanxi University of Chinese Medicine, Xianyang, People’s Republic of China; 2Department of Internal Medicine, Shaanxi Provincial Cancer Hospital, Xi’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Zhang, Department of Internal Medicine, Shaanxi Provincial Cancer Hospital, Xi’an, People’s Republic of China, Email [email protected]
Purpose: Lung cancer chemotherapy patients’ self-management behaviors were not satisfactory, especially treatment-related management scored low compared to other management. This study used the capability, opportunity, and motivation-behavior (COM-B) model of behavioral change to explore the perspectives when performing self-management.
Methods: The study employed semi-structured interviews with 15 patients undergoing chemotherapy for lung cancer. The COM-B model was utilized to guide the development of interview themes and to inform the content analysis methods applied.
Results: The study identified three main themes and eight sub-themes. These included: (1) Competency factors, which encompassed poor management of symptoms and chemotherapy side effects, as well as a lack of patient self-management awareness; (2) Motivational factors, which involved the complexity of the chemotherapy regimen reducing patients’ confidence in treatment management, insufficient family support, and a lack of patients’ sense of meaning in life with low future expectations; and (3) Opportunity factors, which included financial burden preventing patients from practicing self-management of their disease, lack of access to authoritative knowledge, and limited opportunities to practice self-management.
Conclusion: This study proposes targeted interventions based on the research findings, including strengthening symptom management for patients, enhancing patients’ knowledge of self-management of health through health training, seminars, and peer exchange meetings, and providing further opportunities for patient self-management by establishing family support networks, community peer support groups, and constructing authoritative health information platforms. By linking social resources, the economic pressure on patients is alleviated. Our research results will contribute to comprehensive self-management for lung cancer chemotherapy patients.
Keywords: lung cancer chemotherapy, behavioral research, ability, opportunity, motivation-behavior model, qualitative interviews
Introduction
Lung cancer is a malignant tumor originating from the mucosal epithelium of the bronchial tubes. 2024 data released by the National Cancer Center of China showed that there were 1,060,600 new cases of lung cancer in China in 2022, accounting for 18.20% of all new cancer cases, and lung cancer is still the first malignant tumor with the highest incidence rate in China.1 Chemotherapy, as one of the three major methods for cancer treatment, can selectively kill cancer cells while also damaging normal human cells, leading to adverse reactions such as nausea and vomiting in patients,2 which seriously affects the quality of patients’ lives. Multiple cycles of chemotherapy and various combinations of treatment, frequent hospital entrances and exits, etc., make lung cancer chemotherapy patients prone to the existence of care, information, sharing, and many needs in the areas of emotion and work economy.3,4 Self-management is described as the patient’s ability to actively participate in treatment,5 referring to an individual’s behavioral management, role management, and emotional management of the disease during the treatment process by proactively identifying challenges and resolving disease-related problems.6 Studies have shown that self-management improves health, healthcare, and doctor-patient relationships and communication, reduces depression, fatigue, pain, and emergency room admissions,7–10 and that cancer patients who self-manage have a better disease management experience and quality of life.11 Although some studies have attempted to construct self-management interventions for lung cancer patients, these studies still have certain limitations in terms of intervention objectives, subjects, and evaluation indicators. For example, one study12 conducted peer support education based on a mobile application platform to explore its impact on psychological resilience and coping styles in patients with middle and advanced lung cancer, but its primary outcome indicators did not focus on the improvement of self-management behaviors; another study13 used mobile health technology to develop a self-management intervention program for lung cancer patients, which had strong generalizability, but its intervention subjects covered a wide range and failed to specifically target the chemotherapy patient population for tailored design.
At this stage, studies have shown that the self-management behaviors of lung cancer chemotherapy patients are not ideal, and the exploration of the factors affecting the self-management of lung cancer chemotherapy patients focuses more on the relationship between patients’ self-management behaviors and their knowledge, social support, self-efficacy, and general demographic factors and other objective indicators, and pays less attention to the patient’s own psychological and opportunistic factors.14 The applicability and effectiveness of the Capability, Opportunity, and Motivation-Behavior (COM-B) model in investigating the barriers and facilitators influencing patient behavior have been confirmed in multiple studies.15 Therefore, the purpose of this paper is to talk with patients in depth through the interview outline constructed based on the capability, opportunity, and motivation-behavior (COM-B) model to understand the difficulties and problems of lung cancer chemotherapy patients in self-management, to provide healthcare professionals with a better understanding of the difficulties and problems of self-management for lung cancer chemotherapy patients in their clinical work. To provide a reference for healthcare professionals to provide more effective health education for lung cancer chemotherapy patients in their clinical work.
Conceptual Framework
The Behavior Change Wheel theory was proposed by Michie et al16 in 2011, combining 19 behavior change-related theoretical frameworks as shown in Figure 1. The BCW theory is shaped like a “wheel”, with the inner COM-B model (Figure 2) serving as the theoretical foundation of this study and the core essence of the Behavior Change Wheel theory. It can be used to comprehensively analyze the facilitating and hindering factors influencing individual behavior change. The COM-B model consists of three core elements: Capability, Opportunity, and Motivation. The theoretical model explicitly states that the generation and maintenance of individual behavior (Behavior) require the synergistic interaction of three dimensions: capability foundation, opportunity conditions, and motivational drive.17 “Capability” encompasses the physical and mental conditions individuals need to facilitate behavioral change. “Motivation” refers to the brain’s intrinsic mechanisms that direct and incentivize individual behavior, divided into automatic motivation and reflective motivation. “Opportunity” denotes all external conditions (ie, the external environment) that enable individuals to perform the relevant behavior, including the physical and social environments. The COM-B model has been widely applied in exploring factors that promote or hinder patients’ health behaviors, designing behavioral interventions, perioperative care, and other studies, with a significant portion involving qualitative research.18–20 This demonstrates the suitability of the COM-B model for conducting qualitative interviews.
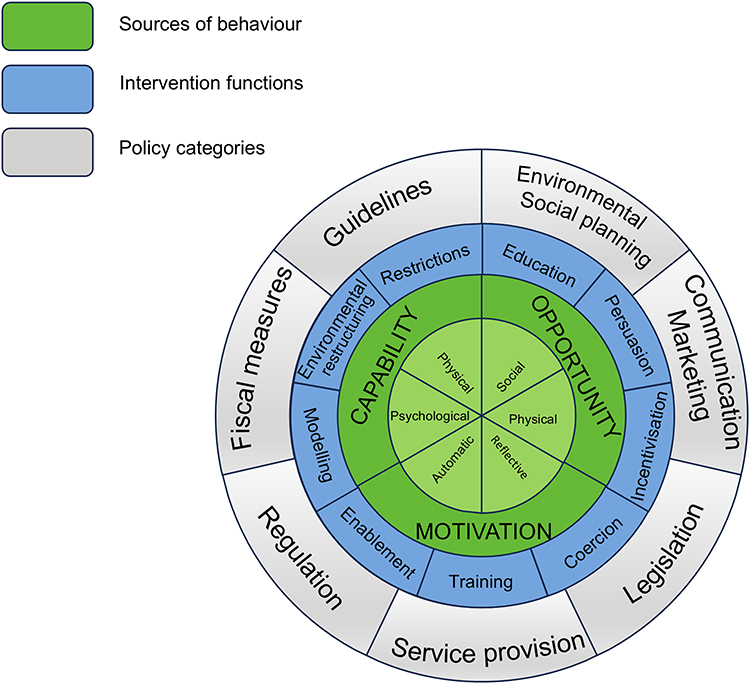 |
Figure 1 Behavior Change Wheel. |
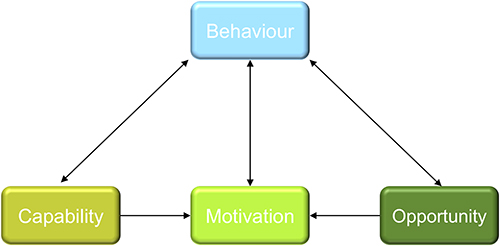 |
Figure 2 COM-B model. |
Materials and Methods
Recruitment
This study employed purposive sampling to select lung cancer patients undergoing chemotherapy in the oncology department of a tertiary Grade A specialized hospital in Xi’an, Shaanxi Province, from March to May 2024 as the research subjects. Based on the principle of maximum variation, patients with diverse experiences and backgrounds were chosen for in-depth interviews to ensure the richness and representativeness of the research findings. This study has been approved by the Ethics Committee of Shaanxi Cancer Hospital (Approval No.: Medical Ethics Review [2022] No. (18)) and complies with the Declaration of Helsinki. Before conducting formal interviews, the interviewer explained the purpose and methods of the study in detail to the patients and obtained informed consent from the participants. Inclusion criteria: 1) patients diagnosed with lung cancer and receiving chemotherapy by the diagnostic criteria of the Chinese Medical Association Lung Cancer Clinical Diagnosis and Treatment Guidelines (2023 Edition);21 2) patients without cognitive impairment and psychiatric disorders; 3) patients with clear consciousness and normal communication; 4) patients ≥18 years old; 5) patients with a Barthel Index score of ≥60; and 6) patients who are aware of their condition and voluntarily participate in this study. Exclusion criteria: 1) patients with other malignant tumors and major organ diseases such as heart, liver, spleen, lungs, and kidneys; 2) patients with major diseases of the nervous system, immune system, and hematological system; 3) patients with mental disorders or cognitive disorders.
Sample Size
The sample size of this study was based on the criteria of saturation of data and the absence of new themes.22 Qualitative research suggests that a minimum sample size of 12 participants is required to achieve information saturation.23 After interviewing 12 participants, it was found that the data was not saturated. Adding 2 more patients did not introduce new themes in the interview data. To further confirm thematic saturation, an additional interview was conducted, which resulted in data saturation. Therefore, this study ultimately determined 15 patients.
Research Methodology
Development of Interview Outlines
Based on searching for related literature,24,25 the preliminary interview outline was set up based on the COM-B model, and after discussion by the group, two lung cancer chemotherapy patients in the Department of Medical Oncology who met the inclusion conditions were selected for pre-interview, and the interview outline was adjusted according to the experts’ opinions and the patients’ feedbacks, The interview guideline is shown in Table 1.
 |
Table 1 Interview Guideline |
Methods of Data Collection
A descriptive qualitative research method was used, in which one researcher who had studied qualitative research methods and had experience in qualitative research conducted interviews with patients face-to-face. The interviewer communicated with the interviewee in advance and agreed with the patient on the time and place of the interview, which was selected in a quiet and private conference room. At the beginning of the interview, patients were briefly introduced to the purpose of the interview, the content and method of the interview to gain their trust, and were informed that the whole interview was recorded, and were invited to sign an informed consent form after obtaining their informed consent. During the interview, we flexibly adjusted the order of questions and the way of questioning according to the patient’s answers, and at the same time recorded non-verbal information such as the interviewee’s expression, tone of voice changes, and body movements, to avoid suggesting or guiding the interviewee’s behavior. The length of the interview was 20–30 min for each case.
Methods of Data Analysis
Within 24 hours after the interview, the interview recordings were transcribed into text. Two researchers who did not participate in the interview process organized the basic information of the interviewees and the text data of the interview recordings. The two exchanged materials for checking, and after the organization was completed, the materials were returned to the interviewees for confirmation to ensure the accuracy of the data. The text was imported into NVivo 14 software and analyzed using directed content analysis,26,27 and themes were summarized and extracted.
Results
This study finally identified eight factors influencing self-management in lung cancer chemotherapy patients were identified based on the COM-B model, For details, please refer to Table 2.
 |
Table 2 Factors of the COM-B Model-Based Framework Analysis |
Participants’ Demographic Characteristics
The lung cancer chemotherapy participants included 11 males and 4 females; ages ranged from 47 to 71 years (61.20±7.78). Table 3 shows in detail the demographic characteristics of the study participants.
 |
Table 3 Participants’ Sociodemographic Characteristics (n=15) |
Capacity Factors
Poor Management of Symptoms and Chemotherapy Side Effects
The various side effects of chemotherapy and the symptoms of the disease itself consume patients’ energy and strength, making it difficult for patients to manage themselves; (N7: After chemotherapy, my legs hurt, my feet are numb and I cannot move, so I can only lie down in bed, and getting up and moving around is all my companion’s help). (N11: My disease is coughing and shortness of breath, which is why I went for a physical examination and found out) (N14: After chemotherapy for three to five days a bit of regurgitation, nausea, and wanting to vomit can not be vomited, eat a little bit of food, but also hair loss, the heart is very difficult to accept at the beginning) (N12: One of the worst issues after chemotherapy is that I developed severe rashes. At night, the itching gets so bad that I cannot sleep, leaving me exhausted during the day).
Lack of Patient Self-Management Awareness
Elderly patients generally have a low literacy level and limited knowledge of chemotherapy (N6: I am illiterate, I have never been to school so I do not understand chemotherapy and I do not want to understand it); (N7: I do not know much about the side-effects of chemotherapy, I just listen to the doctors and nurses, and other people have not told me about it); it’s more difficult to understand self-management for the patients as opposed to healthy exercise, and the patients lack relevant knowledge and have doubts about the final (N3: I have not heard of self-management, and I usually do not manage it, I just do what I should do) (N7: After each chemotherapy session, my legs ache, feel weak, and go numb. The doctor previously prescribed herbal foot soaks for me, but they did not seem to help much, so I stopped using them. Now when I have no energy, I just stay in bed).
Opportunity Factors
Insufficient Family Support
Family support, as the most influential social support, can positively influence individual patient self-care behavior.28 Patients in the middle and advanced stages believe that they are already a burden to their families and are not willing to seek too much help from them (N7: Our home is closer to the hospital and I can still move myself, so I usually come to chemotherapy by myself); patients often need support from other people, especially their family members, to practice self-health management because of limitations of their age, condition, mobility, and level of knowledge and culture; and their children are in the middle and young ages, and it is difficult for them to take care of the elderly and the young while facing social pressures. (N11: I have a son and a daughter with two children; my daughter is married and lives close to me, while my son works overseas and is busy with his work, so my daughter accompanies me every time I go to the doctor, and she also has a child) (N10: My son works in another city, and my wife has gone to his place to help take care of the grandchildren. So, I am usually alone at home).
Lack of Access to Authoritative Knowledge
Peer support plays a great role in the home self-management of lung cancer chemotherapy patients, and some of the patients said that they can obtain health-related knowledge not only from health care but also from their peers, (N12: I have become quite close with several other patients who have undergone chemotherapy. They warned me that chemotherapy severely weakens the immune system, so I need to be extra careful about catching colds or the flu. That’s why I am now very mindful about staying warm); thus, it can be seen that peer support has a good role in health education for patients, and patients are more persuasive to other patients through their personal experiences. Support has a good role in health education for patients, patients through their own personal experience to other patients to persuade more convincing, but in this study peer education exposed a point, peers in the health education did not carry out a systematic study of the science of health education, which may lead to the transfer of experience and the correct behavioral guidance has a bias; (N6: people in the same ward said that after chemotherapy can not eat Fish and shrimp, so I do not eat these things at all now); younger lung cancer chemotherapy patients are more receptive to social media, and the rapid development of multimedia in the current stage of society has made a variety of short videos popular for popularizing science and technology, and there is a lot of false information that affects the judgment of the patients (N15: I saw a video online saying that chicken cannot be eaten after chemotherapy. When I arrived at the hospital, I saw a poster in the hospital hallway stating that chicken has the highest protein content and should be eaten more after chemotherapy. This contradicts the information I saw online, and I do not know which one is correct).
Lack of Opportunities for Self-Management Practices
In addition to these factors, the realization of self-management also needs the support of the external environment. However, at present, the whole society relies more on tertiary hospitals for the management of tumors, and the connection with community hospitals or lower-level hospitals is not perfect. (N14: My local community hospital cannot provide this treatment, so I have to come to this hospital instead); (N9: the hospitals in our home area do not maintain PICCs, but only the tertiary hospitals do, and it is inconvenient to go to the city every time for maintenance).
Motivating Factors
Complexity of Chemotherapy Regimens Reduces Patient Confidence in Treatment Management
The treatment plan of lung cancer patients is more complicated. Patients may need to adjust the treatment plan after using chemotherapy drugs for some time due to the emergence of drug resistance, and the frequent change of drugs makes the patients’ confidence in the treatment decrease (N7: the first few times of chemotherapy used another plan, but the plan changed in these two times, so I guessed whether the treatment effect was not good, and the doctor said that using one kind of drug all the time may produce drug resistance, so he adjusted the drug plan); (N6: I had been using another regimen before, and this time I was hospitalized and found that there was no change in the tumor I was ready to change the regimen, and I do not know what the regimen will be like this time); (N4: My chemotherapy markers still have not improved, which makes me question whether the current medication protocol is working).
Financial Burden Prevents Patients from Practicing Disease Self-Management
With the wide application of the DRG charging model, the burden on some patients has been greatly reduced. However, due to the special characteristics of chemotherapy drugs, the newly developed drugs are often not covered by medical insurance, and the long cycle of treatment leads to the fact that the patients still need to pay high treatment costs, and some of the patients often give up or interrupt the treatment due to financial or family reasons. (N4: I have changed to a new regimen this time. The drug is expensive and I have to pay for it out of my pocket. I have to spend more than 20,000 yuan for one chemotherapy treatment, which is not affordable); (N11: I could not afford the treatment after I finished chemotherapy in October last year, and I did not come for treatment for almost half a year because I did not finish the last cycle of chemotherapy)
Patient’s Lack of a Sense of Meaning in Life and Low Expectations for the Future
The condition of patients with middle and advanced lung cancer chemotherapy is more serious, the chemotherapy cycle is longer, and chemotherapy is one of the palliative treatments with almost no possibility of a complete cure, which leads to the patients’ low expectations of themselves; (N11:The treatment cycle is so long that it takes years of your life, and even if you are cured, you will not have time to finish what you want to do); (N3: I said at my age it makes little difference whether I get treatment or not, but my son and daughter insist that I continue with the therapy).
Discussion
Enhancing Self-Management Cognition and Symptom Management
The study results found that lung cancer chemotherapy patients, especially the elderly group, often because of disease progression, chemotherapy drugs to normal cells non-selective damage and physiological function, and face pain, fatigue, sleep disorders, depression, and a series of complex and diverse adverse reactions. Studies show that these adverse reactions not only affect the quality of life of patients but also seriously restrict the development of self-management ability.29 Based on extensive research evidence,30–32 effective self-management has been shown to significantly improve outcomes, reduce the incidence of adverse effects, and help control treatment costs in oncology patients, and inadequate self-management perceptions have the potential to affect the control and progression of patients’ symptoms.33 Therefore, to enhance the physical ability of lung cancer chemotherapy patients, healthcare personnel should play a central role in guiding patients to take effective preventive measures through systematic health education, discovering patients’ uncomfortable symptoms in time and treating them symptomatically, reducing the severity and incidence of adverse reactions, ensuring patients’ physical condition, and promoting better patient outcomes. At the same time, the training of medical and nursing staff on chemotherapy-related knowledge is strengthened to further enhance the nursing capacity of nurses.
Improving Self-Efficacy and Enhancing Patients’ Confidence in Self-Management
The diversity of chemotherapy treatment options and the incidence of side effects are high. At the beginning of chemotherapy, patients need health education and related guidance. However, clinical observation shows that patients often can not fully understand the interpretation of medicine.34 The research found that35 some patients who received health education after chemotherapy still experienced difficulties in managing daily activities, complications (such as constipation and nausea), and identifying risk factors like elevated body temperature. This is related to the fact that most of the lung cancer chemotherapy patients in this study were found to have a low level of literacy themselves, with less exposure to medical knowledge. And that self-management is a newer concept of care compared to health education. And that the patients did not have a deep understanding of self-management. Secondly, chemotherapy regimens are complex and change frequently, which makes patients question the effectiveness of chemotherapy and is not conducive to stimulating self-management behaviors. On the other hand, patients have low expectations for the future, and their negative expectations make them lose confidence in self-management, which leads to a low self-efficacy state. Therefore, healthcare professionals should pay attention to improving patients’ psychological ability and stimulating patients’ behavioral motivation. Through psychological guidance, the establishment of patient role models, verbal incentives and the setting of expected management goals to help patients to restore the expectations of the treatment, and timely understanding of the patient’s chemotherapy program updates, explained in advance to eliminate the patient’s doubts about the treatment, and enhance the patient’s confidence in self-management.
Building an Authoritative Health Platform to Help Patients Achieve Self-Management
This study found that with the rapid development of internet technology, patient groups tend to use online platforms to independently search for health information to achieve self-health management; however, the spread of false information and patients’ low discrimination ability regarding health information leads them to mistakenly trust and utilize poor-quality information from unclear sources, resulting in delays in disease treatment and management, ultimately affecting their overall health.36 Secondly, this study found that peer support plays a role in patient self-management, but it also exposed some drawbacks. The communication between patients is often based on their own experience or personal feelings, and they may ignore the differences between individuals which leads to differences in the taught experience and correct behavioral guidance. Therefore, medical staff should strengthen the health guidance of patients and help them master the correct knowledge of self-management through the form of health exhibition training or theme seminars. For false information on the Internet, medical institutions can build official, authoritative health information platforms or applications. The effectiveness of mobile health platform applications has been confirmed in some research.37 Or they can establish official media accounts and communication groups and regularly push high-quality popular science videos and articles to help patients correct misconceptions.
Enhancing Social Support and Providing Patients with Self-Management Opportunities
This study found that some patients attended medical visits unaccompanied or accompanied only by their spouses, lacking family members who could participate in decision-making or provide emotional support. As a result, these patients exhibited poorer self-management abilities and treatment adherence, which aligns with the findings of Anika Sparla et al.38 It is analyzed for three main reasons as follows: 1) Family factors: Some patients’ children are in their prime working years and serve as the primary economic pillars of their households, with responsibilities for both the elderly and the young, making it difficult to balance caregiving duties for their parents. 2) Environmental factors: Some patients live far from home and choose to temporarily rent near the hospital to avoid long commutes. The unfamiliarity of the new environment and the lack of familiar friends around them can lead to social isolation. 3) Social factors: The high cost of treatment prevents some patients from completing the full treatment cycle, resulting in interrupted care and leaving little room for managing their health. Based on the above three aspects of issues, medical staff should comprehensively consider the social factors affecting patients’ self-management when conducting health management education for lung cancer chemotherapy patients. For patients lacking family support, efforts should be made to strengthen their family support network by actively communicating with family members, reminding them to pay attention to the patient’s emotional needs, instilling the importance of self-management to family members, and guiding family members to assist patients with self-management. For patients lacking peer support, a hospital-community linkage mechanism should be established to set up mutual aid groups at the community level. Through organizing regular activities, patients can be helped to adapt to new environments and enhance mutual understanding and trust, thereby forming a positive social network to alleviate patients’ loneliness and provide them with a platform to exchange treatment experiences and encourage each other. For patients with financial difficulties, information about financial support such as medical assistance and charitable funds should be provided, and assistance should be given in applying for relevant aid programs. At the same time, professional psychological counseling services should be offered to help patients and their families alleviate anxiety caused by financial pressure and strengthen their courage and confidence in facing difficulties.
Strengths and Limitations
For the first time, the COM-B model was used to conduct qualitative interviews with lung cancer chemotherapy patients, comprehensively analyzing the internal and external factors affecting patients’ self-management from three levels: capability, motivation, and opportunity. The COM-B model is the core connotation of the BCW theory. Analysis based on the COM-B model facilitates the combination of the nine major intervention measures of the BCW theory to formulate specific and comprehensive intervention measures.
This study also has certain limitations. First, it only analyzed the influencing factors of self-management in lung cancer chemotherapy patients from the patient’s perspective. However, patient management should be multi-level and multidisciplinary, involving collaboration among various aspects such as doctors and family caregivers. Therefore, future research could consider conducting interviews at the level of patients’ family caregivers and doctors to understand the difficulties existing beyond the patients themselves, and to develop more comprehensive and multidimensional intervention measures. Second, although the sample size reached saturation with 15 patients, this study was only conducted in one hospital in the northwestern region. There may be differences in resources, regional diets, and cultures across hospitals at all levels nationwide. Thus, future studies could conduct multicenter, larger-sample research to reduce the heterogeneity of the results. Finally, the inherent limitations of qualitative research are also involved in this study, as the research data comes from patients’ subjective feelings. Respondents may conceal their true thoughts due to social desirability, power dynamics, or privacy concerns, or provide “idealized” responses, resulting in participant bias and social desirability bias in the findings.
Conclusion
Focusing on the real experiences of lung cancer chemotherapy patients in conducting self-management after treatment, this study conducted in-depth interviews with 15 lung cancer chemotherapy patients using the COM-B model as a theoretical framework. In this study, the capability factors affecting the self-management of lung cancer patients undergoing chemotherapy: are poor management of symptoms and chemotherapy side effects, as well as insufficient patient awareness of self-management; motivational factors: the complexity of chemotherapy regimens reduces patients’ confidence in treatment management, inadequate family support, lack of a sense of meaning in life, and low future expectations; opportunity factors: economic burden hinders patients from implementing disease self-management, lack of authoritative knowledge acquisition channels, and insufficient opportunities for self-management practice; these factors are barriers affecting patients’ self-management. Among the opportunity factors, patients’ ways of acquiring knowledge: peer communication, and online information retrieval, although having certain drawbacks, also promote patients’ self-management to some extent and are facilitating factors for self-management. Therefore, regarding patients’ barriers and facilitating factors, healthcare professionals should actively improve the symptoms of lung cancer patients after chemotherapy, develop individualized management plans, provide multi-channel educational resources, ensure the dissemination of correct health knowledge, pay attention to patients’ family and economic situations, help disadvantaged patients connect with social resources, and ensure the complete implementation of the treatment cycle.
In future research, we will base our work on the nine intervention functions of the Behavior Change Wheel theory. Through extensive literature retrieval and expert correspondence, we will further develop self-management intervention measures for lung cancer chemotherapy patients. The feasibility and effectiveness of the experiment will be verified through small-scale pilot testing. The intervention plan will then be revised accordingly to form a formal protocol. Subsequently, randomized controlled trials and long-term follow-up studies will be conducted to evaluate the impact of the interventions on patients’ self-management behaviors, self-efficacy, and quality of life, with the aim of further optimizing the design and implementation of the interventions.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee of Shaanxi Provincial Cancer Hospital, with the approval number of Medical Ethics Review [2022] No. (18). All methods were carried out in accordance with relevant guidelines and regulations. Written informed consent was obtained from all the participants. Participants were informed about the study and consented to the anonymous information including “publication of anonymized responses/direct quotes” being used for publication.
Acknowledgments
The authors are grateful for the assistance of the hospitals and wish to extend special thanks to all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by General Project of Shaanxi Province’s Key Research and Development Plan, grant number 2024SF-YBXM-389.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
2. Ma JS, Xu H, Liu S, Wang AP. Sentinel symptoms within symptom clusters in lung cancer patients during initial postoperative chemotherapy: a cross-sectional study. Nurs Res China. 2022;36(19):3528–3533. doi:10.12102/j.issn.1009-6493.2022.19.029
3. Borghetti P, Guerini AE, Sangalli C, et al. Unmet needs in the management of unresectable stage III non-small cell lung cancer: a review after the ‘radio talk’ webinars. Expert Rev Anticancer Ther. 2022;22(5):549–559. doi:10.1080/14737140.2022.2069098
4. Wang T, Zhang J, Yu M. Unmet needs trajectory in lung cancer patients undergoing chemotherapy: a longitudinal study. Chin J Nurs. 2022;57(17):2068–2072. doi:10.3761/j.issn.0254-1769.2022.17.003
5. Allegrante JP, Wells MT, Peterson JC. Interventions to support behavioral self-management of chronic diseases. Annu Rev Public Health. 2019;40:127–146. doi:10.1146/annurev-publhealth-040218-044008
6. Grady PA, Gough LL. Self-management: a comprehensive approach to management of chronic conditions. Am J Public Health. 2014;104(8):e25–e31. doi:10.2105/AJPH.2014.302041
7. Ory MG, Ahn S, Jiang L, et al. Successes of a national study of the chronic disease self-management program: meeting the triple aim of health care reform. Med Care. 2013;51(11):992–998. doi:10.1097/MLR.0b013e3182a95dd1
8. Ansari RM, Harris M, Hosseinzadeh H, Zwar N. Healthcare professionals’ perspectives of patients’ experiences of the self-management of type 2 diabetes in the rural areas of Pakistan: a qualitative analysis. Int J Environ Res Public Health. 2021;18(18):9869. doi:10.3390/ijerph18189869
9. Niknami M, Mirbalouchzehi A, Zareban I, Kalkalinia E, Rikhtgarha G, Hosseinzadeh H. Association of health literacy with type 2 diabetes mellitus self-management and clinical outcomes within the primary care setting of Iran. Aust J Prim Health. 2018;24(2):162–170. doi:10.1071/PY17064
10. Shnaigat M, Downie S, Hosseinzadeh H. Effectiveness of health literacy interventions on COPD self-management outcomes in outpatient settings: a systematic review. COPD. 2021;18(3):367–373. doi:10.1080/15412555.2021.1872061
11. Howell D, Richardson A, May C, et al. Implementation of self-management support in cancer care and normalization into routine practice: a systematic scoping literature review protocol. Syst Rev. 2019;8(1):37. doi:10.1186/s13643-019-0952-5
12. Liao R, Chen L, Chen J, et al. Effect of WeChat-based peer support education on psychological resilience and coping styles in patients with advanced lung cancer. Chin J Health Educ. 2020;36(10):942–945. doi:10.16168/j.cnki.issn.1002-9982.2020.10.015
13. Ni X, Lou Y, Hu W, et al. Development of mobile health-based self-management support for patients with lung cancer: a stepwise approach. Nurs Open. 2022;9(3):1612–1624. doi:10.1002/nop2.1185
14. Ni X, Zeng A, Pan R, et al. Construction of a structural equation model of factors influencing self-management behaviors in lung cancer patients receiving chemotherapy. Mil Nurs. 2022;39(12):10–13. doi:10.3969/j.issn.2097-1826.2022.12.003
15. Li H, Li Y, Wang J, Zhang Y, Ben S. Enablers and barriers to medication self-management in patients with type 2 diabetes: a qualitative study using the COM-B model. Patient Prefer Adherence. 2025;19:485–501. doi:10.2147/PPA.S503350
16. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
17. White LL, Cohen MZ, Berger AM, Kupzyk KA, Bierman PJ. Self-efficacy for management of symptoms and symptom distress in adults with cancer: an integrative review. Oncol Nurs Forum. 2019;46(1):113–128. doi:10.1188/19.ONF.113-128
18. Bhandari B, Narasimhan P, Vaidya A, Subedi M, Jayasuriya R. Barriers and facilitators for treatment and control of high blood pressure among hypertensive patients in Kathmandu, Nepal: a qualitative study informed by COM-B model of behavior change. BMC Public Health. 2021;21(1):1524. doi:10.1186/s12889-021-11548-4
19. O’Donovan B, Mooney T, Rimmer B, et al. Advancing understanding of influences on cervical screening (non)-participation among younger and older women: a qualitative study using the theoretical domains framework and the COM-B model. Health Expect. 2021;24(6):2023–2035. doi:10.1111/hex.13346
20. Pearse BL, Keogh S, Rickard CM, Fung YL. Barriers and facilitators to implementing evidence based bleeding management in Australian cardiac surgery units: a qualitative interview study analysed with the theoretical domains framework and COM-B model. BMC Health Serv Res. 2021;21(1):550. doi:10.1186/s12913-021-06269-8
21. Han BH, Wang J. Chinese medical association guidelines for clinical diagnosis and treatment of lung cancer (2023 version). Chin J Oncol. 2023;45(7). doi:10.3760/cma.j.cn112152-20230510-00200
22. Weller SC, Vickers B, Bernard HR, et al. Open-ended interview questions and saturation. PLoS One. 2018;13(6):e0198606. doi:10.1371/journal.pone.0198606
23. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18(1):148. doi:10.1186/s12874-018-0594-7
24. Zhu HX, Pang JM, Sun SN, et al. Factors influencing pulmonary rehabilitation behaviors in elderly lung cancer patients during postoperative transition: a qualitative study. Chin J Nurs. 2024;59(1):15–21. doi:10.3761/j.issn.0254-1769.2024.01.002
25. Sun JR. Effect of a COM-B model-based prenatal care program on childbirth fear in primiparous women during late pregnancy [master’s thesis]. Shanxi Medical University; 2023.
26. Tørring B, Gittell JH, Laursen M, Rasmussen BS, Sørensen EE. Communication and relationship dynamics in surgical teams in the operating room: an ethnographic study. BMC Health Serv Res. 2019;19(1):528. doi:10.1186/s12913-019-4362-0
27. Slater MD. Content analysis as a foundation for programmatic research in communication. Commun Methods Meas. 2013;7(2):85–93. doi:10.1080/19312458.2013.789836
28. Zhang Z, Koirala B, Gong G, Bai X, Mao J, Davidson PM. Predictors of self-care among Chinese patients with chronic heart failure: a situation-specific theory-guided structural equation model analysis. J Cardiovasc Nurs. 2023;38(3):E87–E97. doi:10.1097/JCN.0000000000000918
29. Ye YX, Qin L, Luo JH, et al. Prevalence and influencing factors of chemotherapy-related symptom clusters in lung cancer patients. Chin J Nurs. 2023;58(18):2230–2238. doi:10.3761/j.issn.0254-1769.2023.18.008
30. Rowntree RA, Hosseinzadeh H. Lung cancer and self-management interventions: a systematic review of randomised controlled trials. Int J Environ Res Public Health. 2022;19(1):536. doi:10.3390/ijerph19010536
31. Zhang H, Huang QM, Wu FL, et al. Development and usability evaluation of a visual assessment tool for chemotherapy-related adverse reactions in breast cancer patients. J Nurs Sci. 2024;39(5). doi:10.3870/j.issn.1001-4152.2024.05.010
32. Taylor JL, Roberts L, Hladek MD, et al. Achieving self-management goals among low income older adults with functional limitations. Geriatr Nurs. 2019;40(4):424–430. doi:10.1016/j.gerinurse.2019.01.003
33. Wang AZ, Mu WF, Gu F, et al. Latent profile analysis of self-management in elderly patients with lower extremity venous ulcers and its nursing implications. Chin J Nurs. 2024;59(12):1429–1436. doi:10.3761/j.issn.0254-1769.2024.12.003
34. Sibold HC, Thomson MC, Hianik R, et al. Videos improve patient understanding of chemotherapy terminology in a rural setting. Cancer. 2021;127(21):4015–4021. doi:10.1002/cncr.33810
35. Lee M, Kim N, Kim HY, Lee A, Yoon J, Cho J. Which chemotherapy-related terms were difficult for cancer patients, and who would have the most difficulties? Cancer Res Treat. 2024. doi:10.4143/crt.2024.485
36. Lin RJ, Liu CX, Duan LX, et al. Research progress on authoritative health information identification behaviors among middle-aged and elderly patients with chronic diseases. China Public Health. 2024;40(8):937–942. doi:10.11847/zgggws1142467
37. Tian T, Guan MJ, Liu LJ, Su XQ, Wang H, He L. Study on the efficacy of “information platform + self-care model” on the health status of discharged patients following vaginal natural orifice transluminal endoscopic surgery. Int J Women's Health. 2023;15:1185–1195. doi:10.2147/IJWH.S416134
38. Sparla A, Flach-Vorgang S, Villalobos M, et al. Individual difficulties and resources - a qualitative analysis in patients with advanced lung cancer and their relatives. Patient Prefer Adherence. 2016;10:2021–2029. doi:10.2147/PPA.S110667
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.